


ABSTRACT
Management of chronic pain is one of the most challenging medical issues in primary care. Effective pain management requires an understanding of nociplastic pain, a condition characterized by amplification of pain transmission and pain perception. Unlike nociceptive and neuropathic pain, nociplastic pain does not involve visible tissue injury or damage, which makes it difficult to understand and manage. This review discusses practical ways for primary care clinicians to identify and manage nociplastic pain at the point of care.
The most common barriers to effective pain management should be identified and addressed in the primary care setting, along with mitigation strategies, to achieve better pain control.
An alliance between the patient and primary care clinician is important because it increases treatment receptiveness, motivation, and adherence.
Nonpharmacologic treatment options are preferred because they have fewer side effects, greater availability, and sustained positive effects.
Pain is defined by the International Association for the Study of Pain as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage.”1 Pain that persists beyond the expected healing period of 3 months is defined as chronic pain.2 Chronic pain can have a profound negative impact on a patient’s emotional and social well-being2 and exacts high societal costs as well. In the United States, the estimated societal cost of chronic pain is $560 to $635 billion per year, much higher than the economic impact of heart disease, diabetes mellitus, human immunodeficiency virus infection, Alzheimer disease, and even cancer,3 and chronic pain accounts for 53% of indirect costs.4 Moreover, 2.5% to 4.5% of gross domestic product in the United States is spent on chronic pain.3
More than half of patients receive care for chronic pain in the primary care setting.5 Given that chronic pain is highly prevalent—more than the combined incidences of diabetes, heart disease, and cancer in the United States—a large percentage of primary care clinicians will manage chronic pain in their practices.3 Thus, it is imperative that they understand how to manage pain safely and effectively.
PAIN CATEGORIZATION
Pain can be characterized into 3 mechanistic phenotypes.6
Nociceptive pain arises from tissue damage, injury, or degeneration caused by trauma, osteoarthritis, and joint inflammation (eg, rheumatoid arthritis). It is localized to the area of the damage, injury, or inflammation, and can respond to topical or systemic therapies, including nonsteroidal anti-inflammatory drugs, opioids, and corticosteroids.7
Neuropathic pain is a result of nerve injury or damage, such as traumatic nerve injury, diabetic neuropathy, sciatica or radiculopathy from mechanical nerve compression, or medication- or chemotherapy-induced neuropathy. The pain can be localized to the area of nerve injury or damage, or it can follow a dermatomal distribution, causing characteristic features of sharp, shooting, burning pain along with tingling and numbness.7 It can respond to local therapy and systemic neuropathic medications like gabapentin, pregabalin, and tricyclic antidepressants.
Nociplastic pain, the third and less well-known category of pain, arises from a sensitized nervous system, a condition known as central sensitization syndrome.7 Nociplastic pain involves dysfunction in the central nervous system pathways, including amplified pain-signal processing, decreased signaling of the descending pain inhibitory pathway, or both.8 In contrast to nociceptive pain, there is no demonstrable tissue damage. Nociplastic pain is usually associated with more subjective symptoms rather than objective findings, which makes understanding and managing it a formidable task.
Table 1 summarizes the 3 mechanistic phenotypes of chronic pain.6
Mechanistic types of pain
MECHANISMS OF NOCIPLASTIC PAIN
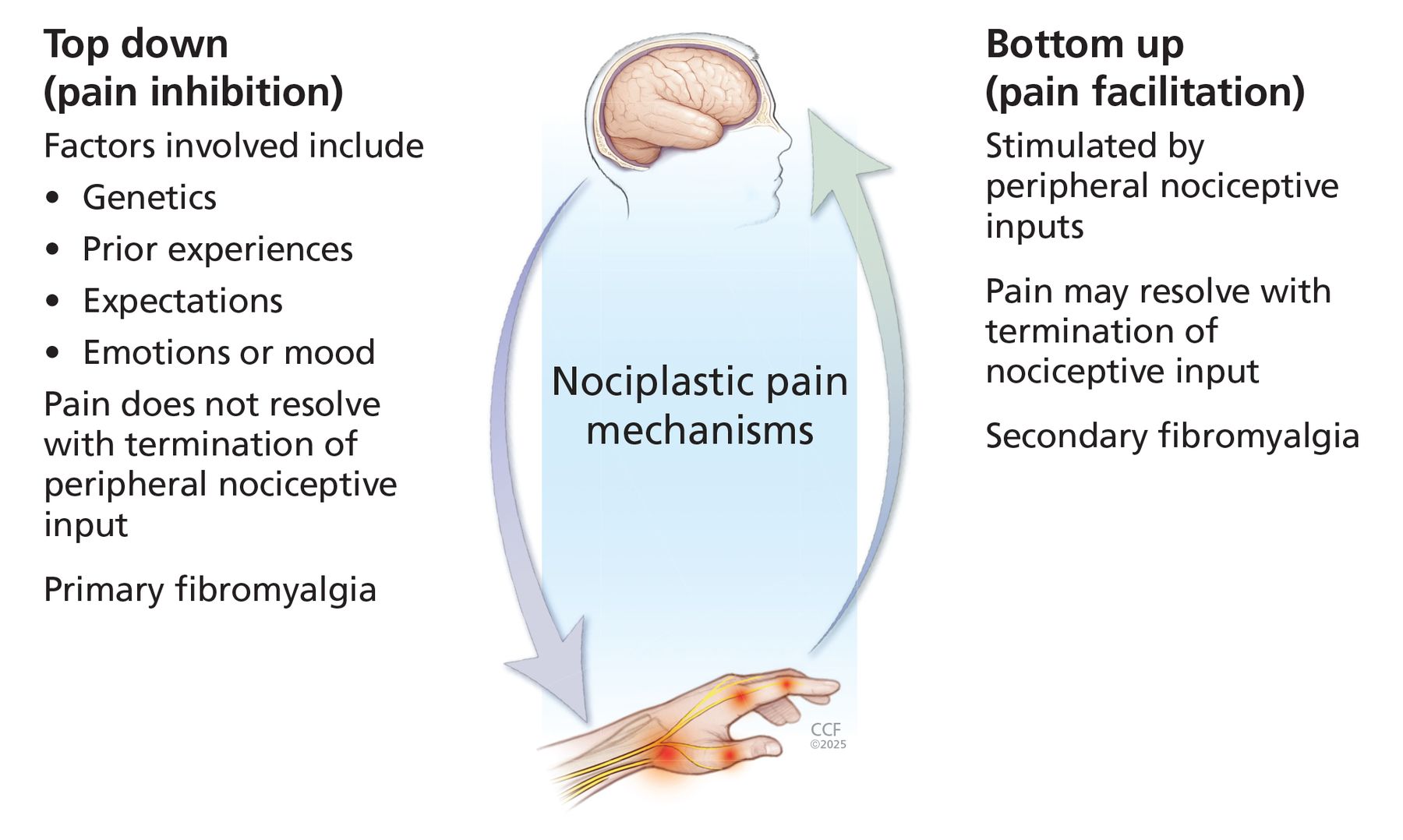
The basic mechanism of nociplastic pain is a heightened pain sensor with amplification of pain transmission and pain perception.8 Specifically, nociplastic pain can be explained by top-down pain amplification (via alteration in the descending pain-modulatory pathway, causing diminished efficacy of the pain-inhibitory pathway and increased activity of the pain-facilitatory pathway) and bottom-up pain facilitation (the ascending pathways in the central nervous system become overstimulated by peripheral inputs), leading to hyperalgesia and allodynia (Figure 1).7

The mechanisms underlying nociplastic pain can be grouped into 2 broad categories: top-down (dysregulation in descending pathways involved primarily in pain inhibition) and bottom-up (dysregulation in ascending pathways primarily involved in pain facilitation).
Based on information from reference 7.
The heightened pain sensitivity and associated features in nociplastic pain conditions (eg, fatigue, poor sleep, brain fog) are driven by central nervous system and peripheral mechanisms.9
Supraspinal mechanisms
Hyperactivity and connectivity in and between brain regions involved in pain, but decreased activity of regions involved in pain inhibition
Altered size and shape of brain regions involved in pain processing
Increased levels of neurotransmitters associated with pain signaling (substance P, glutamate) in cerebrospinal fluid and decreased gamma-aminobutyric acid neurotransmission
Glial cell activation
Spinal mechanisms
Clustering and convergence of signals from different pain loci
Spinal cord reorganization
Increased spinal reflex transmission and diminished spinal inhibition
Temporal summation (repeated stimulus evokes increased pain sensation)
Glial cell activation
Peripheral mechanisms
Minor local muscle pathology (eg, latent and active trigger points)
Peripheral sensitization (eg, expansion of receptive fields, increased concentrations of cytokines and chemokines)
Hyperalgesia, dysesthesia, and allodynia
Localized or diffuse tenderness, or both
This pain-enhancement phenomenon may help explain how nociceptive and neuropathic pain lead to the evolution of nociplastic pain. For example, a patient with acute lower back pain and lumbar disc herniation often has nociceptive pain from the degenerated disc and neuropathic pain (radiculopathy) from nerve compression. Over time, the patient may also develop nociplastic pain. This highlights the importance of adequate and timely control of nociceptive and neuropathic pain in reducing the risk of developing coexisting chronic nociplastic pain.10
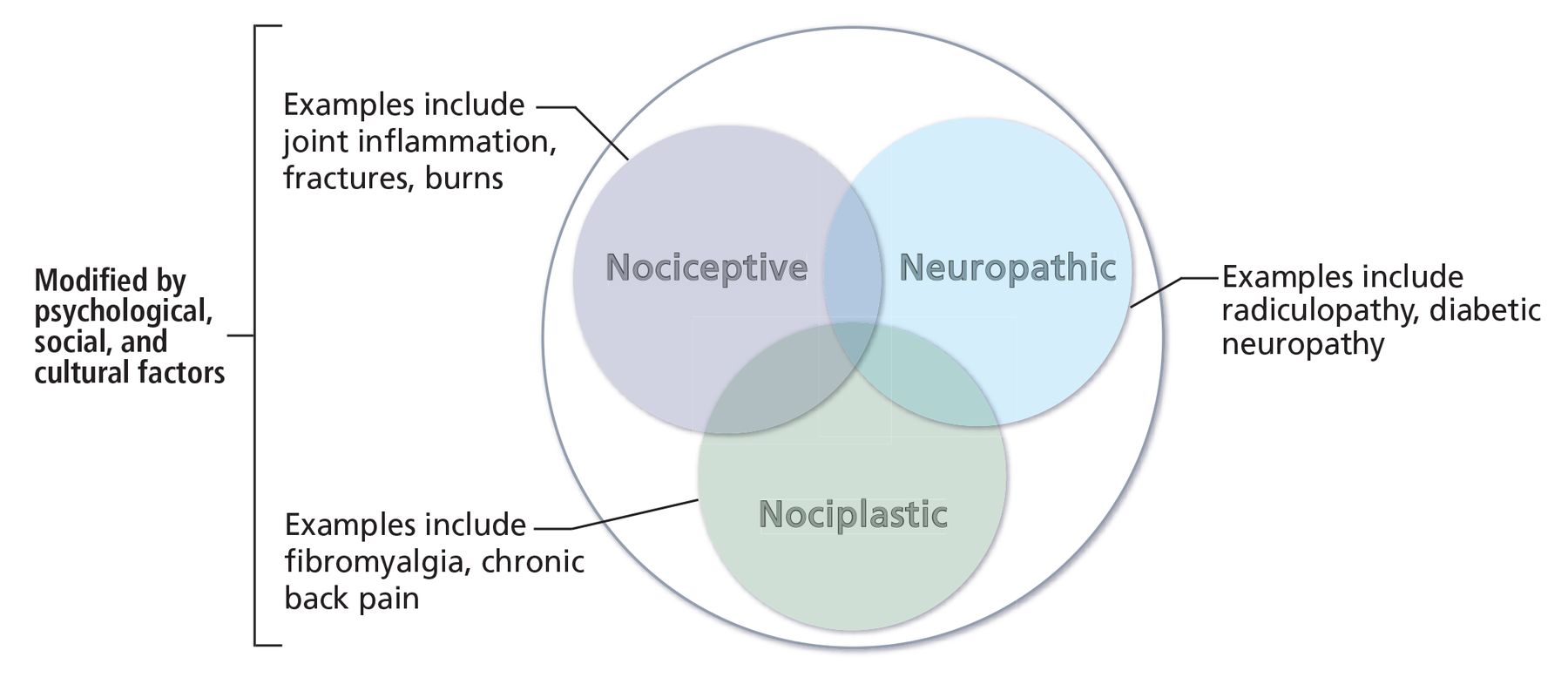
Chronic lower back pain is also an example of a condition in which nociceptive, neuropathic, and nociplastic pain can coexist, even though the 3 categories of pain remain distinct. Such conditions lend credence to the concept of a pain continuum,9 as shown in Figure 2.7 Given this pain continuum, effective management should address all 3 types of pain, as managing 1 type without addressing the others can result in inadequate pain control.

The pain continuum. There are 3 main categories of pain—nociceptive, neuropathic, and nociplastic—and these 3 types of pain can coexist.
Based on information from reference 7.
CHALLENGES AND MITIGATION STRATEGIES
Chronic pain is often frustrating to both patients and primary care clinicians because identifying nociplastic pain can be difficult and take time, and effective treatment modalities are limited. Further, when a patient visits their primary care clinician for chronic pain, they may worry about how their complaint will be perceived. Because nociplastic pain has no visible tissue injury or damage, patients may fear it will be mistakenly labeled by primary care clinicians as “made-up pain,” “all in your head,” “mental illness,” or “drug-seeking behavior.” This fear can prevent them from talking freely about their pain,11 and can make them apprehensive about following the clinician’s recommendations. Moreover, primary care clinicians often lack the knowledge and training needed to identify and manage nociplastic pain, a problem compounded by the nature of the primary care setting, where multiple medical issues must be addressed within a short period of time. It is important to identify and address these barriers with patients to achieve better pain control. Table 210–15 outlines the most common barriers to effective pain management in primary care along with strategies to mitigate them.
Barriers and mitigation strategies for appropriate pain management
Patients with chronic pain can fear having conditions like autoimmune arthritis, multiple sclerosis, or even malignancy. This fear can fuel the patient’s anxiety and contribute immensely to the pain-amplification process, making it imperative that primary care clinicians explore and resolve any of these concerns. Explaining the symptom differences between inflammatory arthritis and osteoarthritis or mechanical arthritis and nociplastic or fibromyalgia-like pain can help reduce anxiety.7 Table 3 provides simple explanations of the 3 pain types that patients can understand easily.7
Simplified ways to explain and compare different types of pain
HOW TO IDENTIFY NOCIPLASTIC PAIN
Conditions that typically cause nociplastic pain can be localized (Table 4)9 or widespread (eg, fibromyalgia) and are known as chronic overlapping pain conditions.7 These conditions often occur together. Widespread nociplastic pain is often accompanied by diffuse tenderness, disabling fatigue, cognitive symptoms, and nonrestorative sleep.16
Localized conditions that cause nociplastic pain
Concurrent symptoms
Nociplastic pain commonly occurs in combination with certain symptoms (Table 5).9 Central sensitization, generalized hypersensitivity, and associated autonomic dysfunction possibly contribute to these concurrent symptoms.8 Some patients with nociplastic pain may also have postural orthostatic tachycardia syndrome due to the same mechanisms.17
Symptoms and factors indicative of nociplastic pain
Standardized scales
Several standardized scales can be used to estimate the probability that nociplastic pain is present. The 2 scales that are most feasible to implement in the primary care setting are the Central Sensitization Inventory and the Central Aspects of Pain questionnaire.
The Central Sensitization Inventory is a simple, validated questionnaire developed to help identify patients with central sensitization, which would indicate they are also experiencing central sensitivity syndrome.18 It has 2 sections. Part A measures 25 health-related symptoms common to central sensitivity syndrome, such as pain, hypersensitivity, mood, and energy, on a numeric scale; a score of 40 or higher out of 100 indicates central sensitivity syndrome. Part B lists previous diagnoses specific to central sensitivity syndrome. The more of these diagnoses a patient has, the greater the likelihood of central sensitization.19 The questionnaire, including instructions, can be accessed at pridedallas.com/questionnaires/.
The self-reported Central Aspects of Pain questionnaire consists of 8 items related to depression, anxiety, catastrophizing, cognition, sleep, and fatigue, and includes a body-pain manikin.20 The questionnaire is a validated measure that assesses the centrality of chronic pain; it best assesses widespread pain in patients who mark 10 or more painful sites out of 26 on the body manikin. Studies have shown that a body manikin, or body map, can be the single most helpful tool to diagnose nociplastic pain.21 The questionnaire, body manikin, and scoring guide can be accessed at academic.oup.com/rheumatology/article-lookup/doi/10.1093/rheumatology/keae342#supplementary-data
Beighton criteria
The Beighton criteria should be used to check for evidence of joint hypermobility.22 Hypermobility arthralgia is a specific type of nociceptive pain that is more common in younger patients. It is often described as pain in multiple joints after overuse, especially after playing sports. Physical therapy and using splints to help prevent joint hyperextension can make a significant difference in the patient’s quality of life.
UTILITY OF AUTOIMMUNE LABORATORY TESTS FOR CHRONIC PAIN
Because pain is a prominent symptom of autoimmune connective tissue diseases, primary care clinicians often order laboratory tests such as antinuclear antibody, rheumatoid factor, and inflammatory markers in patients with chronic pain. Notably, these tests can be nonspecific. For example, up to 20% of the general population test positive for antinuclear antibodies, and a positive test by itself is not sufficient to diagnose systemic lupus erythematosus.23 Moreover, inflammatory markers can be elevated in conditions like infection, malignancy, high body mass index, and untreated obstructive sleep apnea.24 We strongly discourage ordering these tests in the absence of appropriate clinical manifestations (eg, persistently swollen joints, photosensitive rash, unexplained cytopenia or proteinuria, or pleural effusions) given the potential negative outcomes such as increased psychological distress and unnecessary healthcare spending.
NOCIPLASTIC PAIN MANAGEMENT
Effective pain management starts with following barrier mitigation strategies (Table 2), exhibiting empathy, and securing the patient’s trust.7 An alliance between the patient and primary care clinician is important because it increases treatment receptiveness, motivation, and adherence.
Nonpharmacologic treatment options should be the first line of therapy because they have fewer side effects, are widely available, and have sustained positive effects.25
Self-care and management
Social support. When a patient has chronic pain, it affects not only the patient but also the family. Sharing frustrations and anxiety with family and support groups can provide catharsis and increase motivation to learn pain-coping skills.11 Learning how other patients successfully manage similar pain can be helpful and inspiring.
Healthy lifestyle. Adopting general healthy lifestyle measures like regular exercise, good nutrition, proper sleep hygiene, smoking cessation, and ergonomic modifications can have a positive impact on pain control.9
Good communication skills and awareness of sensitive topics. For example, a discussion about weight loss, when appropriate, should be done in a nonthreatening manner because some patients may find it offensive, which could act as a barrier to further care.
Mental health. Seeking help from a mental health professional can enable patients to learn adaptive pain-coping skills in challenging situations. The timing of a referral to a mental health professional depends on the patient’s receptiveness and degree of trust toward the primary care clinician. The topic should be introduced cautiously because a blunt presentation could sever the established relationship with the patient.
Graded aerobic exercise
Short-term aerobic training. Training at the intensity recommended to increase cardiorespiratory fitness provides important benefits, including improved physical function and possible pain relief.16 Getting to the aerobic stage of exercise (with heart-rate increase and sweating) can result in activation of pain-inhibitory and endogenous endorphin pathways and release of “feel good” hormones.26 Exercise can reduce fatigue, improve depression and fitness, and positively affect neuroplasticity, leading to improvements in sleep, memory, and emotional and cognitive functioning.16,27
When patients with nociplastic pain start exercising, they tend to hurt more initially due to their heightened pain sensitivity. Therefore, preparing patients psychologically, reiterating the importance of a graded approach and stressing the need to start slowly, can improve adherence to exercise.28 Patients should be reassured that maintaining a consistent aerobic exercise program will make them feel better over time, which can also help with long-term adherence.
Even if patients are not able to achieve an aerobic level of exercise, movement itself can be beneficial for pain control. For patients with available resources, aquatic aerobics or water therapy (preferably in warm water due to temperature sensitivity) can be particularly helpful for those with underlying arthritis and high body mass index because it can be less painful than land-based exercise.
See the Resources section below for recommended forms of exercise.
Psychoeducational therapy
Different forms of psychotherapy can have a positive impact on nociplastic pain.9 The main goal with these therapies is to “turn down the symptom dial” of the body’s pain sensor (like turning down a volume dial). Options include the following:
Cognitive behavioral therapy
Mindfulness and acceptance-based interventions
Psychodynamic therapies
Biofeedback
Hypnotherapy.
Table 629–36 outlines the components and benefits of various psychoeducational therapies. The Resources section also lists links to online resources that patients can access.
Psychoeducational therapies for nociplastic pain
Physical and alternative therapies
Other nonpharmacologic therapies like acupuncture, massage therapy, virtual reality, transcutaneous electrical nerve stimulation, heat therapy, and cryotherapy have been shown to have some role in managing chronic pain and are thought to work by modulating chronic pain signals through physiologic mechanisms.32
Sleep hygiene
Nonrestorative or poor-quality sleep is associated with fatigue and tiredness and can contribute to pain amplification. Nonrestorative sleep is a strong predictor of chronic widespread pain because sleep is necessary to repair the body and decrease neuronal activity.7
Evaluation and treatment of obstructive sleep apnea and insomnia (difficulty falling asleep, staying asleep, or both) is vital to mitigate the pain amplification and fatigue that results from poor-quality sleep.
Sleep hygiene techniques like yoga, blue-light avoidance, changes to the sleeping environment (eg, removing televisions, screen-time reduction), avoiding exercise close to bedtime, and limiting caffeine can help patients achieve restorative sleep. Sleep-specific cognitive behavioral therapy can help improve insomnia and thereby improve pain.
As a last resort, low-dose trazodone, doxepin, or cyclobenzaprine can be considered for coexisting sleep disturbances that can amplify pain.37,38
Pharmacotherapy
Different medications are used on- and off-label to treat nociplastic pain. It is important to note that these medications have shown only modest efficacy and are fraught with adverse side effects39 and a low adherence rate.40
Traditional analgesic treatments such as muscle relaxants, nonsteroidal anti-inflammatory drugs, acetaminophen, and opioids are less effective for nociplastic pain than for nociceptive pain, and the use of opioid analgesics is strongly discouraged.9,41
Low-dose naltrexone, an opioid antagonist, has shown some benefit for chronic back pain and complex regional pain.9 It is thought to work by activating more opioid receptors, leading to increased response to endogenous opiates. Low-dose naltrexone may also improve memory problems commonly seen in patients with fibromyalgia.42
Duloxetine, milnacipran, and pregabalin are the 3 US Food and Drug Administration–approved medications for the treatment of fibromyalgia.43 Duloxetine had greater efficacy in treating pain and depression. Pregabalin was effective in reducing pain and improving sleep and quality of life.44
Tricyclic antidepressants such as amitriptyline,43 nortriptyline,45 and cyclobenzaprine as well as the alpha 2 delta ligand gabapentin43 are frequently used off-label. Amitriptyline has the most evidence for improving pain, sleep, fatigue, and overall quality of life.43
A summary of pharmacologic approaches is outlined in Table 7.14,46
Pharmacotherapy options for nociplastic pain
COORDINATED CARE
The management of nociplastic pain involves a multidisciplinary approach, including referrals to other specialties (eg, pain specialists). Although referral to pain management can be helpful, the general management principle is to use nonpharmacologic and intervention techniques as described above. Referrals to several different healthcare professionals and time-consuming appointments, especially if not coordinated (ie, each professional trying to manage the disease in their own way), can be exhausting to patients and may hinder improvement. In contrast, coordinated care managed by a primary care clinician can have a favorable outcome.12
FINAL THOUGHTS
Management of chronic pain, particularly of the nociplastic type, is challenging and, at times, may seem like fighting an invisible enemy. We must use all available resources, and that starts with securing buy-in from patients with nociplastic pain. If patients are not invested, all management strategies are set to fail from the start.
The vast array of treatment modalities can be overwhelming for primary care clinicians. In our opinion, the best approach is to select a few options that are accessible to and practical for patients because they will be more likely to adhere to them. An initial approach could be starting with simpler self-management recommendations like regular exercise and pleasant activity scheduling followed by activity pacing. In more severe cases, healthcare professional–directed talk therapy or prescription medications can be considered.
RESOURCES
Primary care clinician training
Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians (acpjournals.org/doi/10.7326/M16-2367)
American Geriatrics Society guideline for the pharmacological management of persistent pain in older persons (agsjournals.onlinelibrary.wiley.com/doi/10.1111/j.1532-5415.2009.02376.x)
Exercise regimens
Fibromyalgia-friendly exercises (www.webmd.com/fibromyalgia/ss/slideshow-fibromyalgia-friendly-exercises)
Physical activity and self-management education program for persons with arthritis from the Centers for Disease Control and Prevention(www.cdc.gov/arthritis/programs)
Pilates for persons with fibromyalgia (youtube.com/watch?v=PnKbwr5WuTw)
The FibroManual: A Complete Fibromyalgia Treatment Guide for You and Your Doctor by Ginevra Liptan, MD (Ballantine Books, 2016)
Water therapy program
Exercise and aquatic therapy videos from the Aquatic Exercise Association (aeawave.org/Arthritis/At-Home-Exercise-for-Arthritis)
Tai chi programs
American Tai Chi and Qigong Association (amtaichi.org/tai-chi-qigong-classes-near-you)
Tai chi for arthritis video lessons by Dr. Paul Lam (youtube.com/watch?v=tAOuEpa01j4)
Tai chi health benefits (health.clevelandclinic.org/the-health-benefits-of-tai-chi)
Cognitive behavioral therapy
Online cognitive behavioral therapy program; a referral is required and there is a fee to enroll (thiswayup.org.au/programs/chronic-pain-program)
Society of Clinical Psychology cognitive behavioral therapy for fibromyalgia (div12.org/treatment/multi-component-cognitive-behavioral-therapy-for-fibromyalgia)
Pacing resource from the Department of Health, Western Australia (painhealth.csse.uwa.edu.au/pain-module/pacing-and-goal-setting)
Patient-perspective video about fibromyalgia and successful pain management (youtube.com/watch?v=tFDsdByqkM0)
Cognitive restructuring (concordia.ca/cunews/offices/provost/health/topics/stress-management/cognitive-restructuring-examples.html)
Psychodynamic therapy (psychologytoday.com/us/therapy-types/psychodynamic-therapy)
Cognitive behavioral therapy for insomnia (sleepfoundation.org/insomnia/treatment/cognitive-behavioral-therapy-insomnia)
Managing insomnia for those with chronic pain (health.clevelandclinic.org/managing-insomnia-for-those-with-chronic-pain)
University of Michigan pain guide
Chronic pain management (painguide.com/pain-care)
Self-care videos (painguide.com/pain-care/self-care)
Cognitive behavioral therapy (painguide.com/pain-care/professional-care/therapies/cbt)
Acupuncture (painguide.com/pain-care/professional-care/therapies/acupuncture)
Acceptance and commitment therapy (painguide.com/pain-care/professional-care/therapies/act)
Tai chi (painguide.com/pain-care/professional-care/therapies/tai-chi)
Yoga (painguide.com/pain-care/professional-care/therapies/yoga)
Massage and spa therapy (painguide.com/pain-care/professional-care/therapies/massage-spa)
Emotional awareness and expression therapy (painguide.com/pain-care/professional-care/therapies/eaet)
Mindfulness
American Mindfulness Association (goamra.org)
Mindfulness for chronic pain from Extension Utah State University (extension.usu.edu/heart/files/mindfulnessforchronicpainmanagement.pdf)
Mindfulness tips from Cleveland Clinic (health.clevelandclinic.org/what-is-mindfulness)
Breathing, body scan, and compassion exercises (livinginthegap.org/blog/3-mindfulness-activities-to-use-in-your-new-daily-practice)
Mindfulness exercises from the Mayo Clinic (mayoclinic.org/healthy-lifestyle/consumer-health/in-depth/mindfulness-exercises/art-20046356)
Pain: Considering Complementary Approaches eBook from the National Institutes of Health (nccih.nih.gov/health/pain-considering-complementary-approaches-ebook)
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
Acknowledgments
The authors gratefully acknowledge the editorial assistance of Indra M. Newman, PhD, of the Wake Forest Clinical and Translational Science Institute (WF CTSI), which is supported by the National Center for Advancing Translational Sciences (NCATS) and National Institutes of Health under award number UM1TR004929.
Footnotes
The views expressed in this review are those of the authors and do not represent an official position of any institution.
- Copyright © 2025 The Cleveland Clinic Foundation. All Rights Reserved.
![]()
Clicking the link below will connect you to begin the credit-claiming process for CME and MOC. After clicking on the link, scroll to the bottom of the page and click on “Complete the CME/MOC Process.” You will need your myCME login information to access this.
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.