


ABSTRACT
Transcatheter aortic valve replacement (TAVR) has steadily replaced surgical aortic valve replacement (SAVR) in symptomatic patients with severe aortic stenosis, primarily those at high risk for surgical complications. As TAVR use increases, spurred by technological advances in valve design and patient preferences for the less-invasive procedure, studies have provided data supporting the efficacy and safety of TAVR. Recently, TAVR has expanded to intermediate-risk patients, increasing the potential patient population. Although emerging evidence supports its use in lower-risk patients, some adverse events may limit its adoption in a wider patient population. These include stroke, paravalvular leak, valve durability, valve thrombosis, and need for pacemaker replacement. Ongoing clinical trials are expected to provide answers.
TAVR has become the preferred alternative to SAVR in inoperable and high-risk patients.
The US Food and Drug Administration has approved TAVR valves for use in patients with aortic valve stenosis who are at intermediate risk of morbidity or mortality associated with open-heart surgery.
Initial outcomes support expanding TAVR to intermediate-risk patients, including mortality and stroke data, but concerns exist related to valve durability, valve thrombosis, and rates of permanent pacemaker implantation.
Surgical aortic valve replacement (SAVR) started in the 1960s with a porcine aortic valve sutured to a stainless steel frame. The first human transcatheter aortic valve replacement (TAVR) procedure in the United States was in 2002. In the past 15 years, technological advances in heart valve design have made TAVR the preferred alternative in patients at high risk for surgical complications. This article outlines studies comparing balloon-expandable TAVR vs SAVR for patients at extreme, high, and intermediate surgical risk, and presents evidence that supports the expanded use of TAVR in patients at lower surgical risk.
TAVR: THE PREFERRED ALTERNATIVE TO SURGERY
For patients needing aortic valve replacement, the initial step was to show that TAVR recipients have better outcomes than those who receive no treatment. In the Placement of Aortic Transcatheter Valves (PARTNER) trial, investigators evaluated all-cause mortality in patients who needed valve replacement but were not candidates for surgery because of an extreme risk for complications (cohort B) (Table 1). In those who were not treated with TAVR, the mortality rate was 50% at 1 year. At 5 years, the mortality rate was 94%. In short, virtually all patients died under conservative medical management. For those undergoing TAVR, mortality rates were significantly lower: 31% at 1 year and 72% at 5 years (P < .0001).1
Defining surgical risk
Investigators next established TAVR outcomes as being noninferior to SAVR in high surgical risk patients (PARTNER trial cohort A) at 1 year.2 A midterm follow-up of this study published in 2015 reported comparable rates of all-cause mortality at 5 years in high-risk patients undergoing TAVR vs SAVR, thus confirming the noninferiority of TAVR vs a surgical approach in high-risk patients for the longest duration of follow-up currently available.3
For patients, if the results of 2 different procedures are similar, they are typically going to choose the less invasive option. As a result, use of TAVR has increased: nearly 300,000 procedures have been performed worldwide, and approximately 75,000 were completed in 2016 alone. These numbers are projected to increase fourfold in the next 10 years. In the United States, almost one-third of Medicare-reported aortic valve replacements in 2015 were performed using TAVR.4
These data show that TAVR has become the preferred alternative to SAVR in inoperable and high-risk patients.
TAVR IN INTERMEDIATE-RISK PATIENTS
The US Food and Drug Administration (FDA) initially approved TAVR for patients judged to be ineligible for open-chest valve replacement cardiac surgery or at high risk for SAVR. This represents a small percentage of the total patient population needing aortic valve replacement. The Society of Thoracic Surgeons database of aortic valve disease cases during 2002 to 2010 (N = 141,905) shows that just 6.2% were ranked as high risk (ie, population eligible for TAVR in 2016). Most patients (79.9%) were low risk, and 13.9% were intermediate risk.5
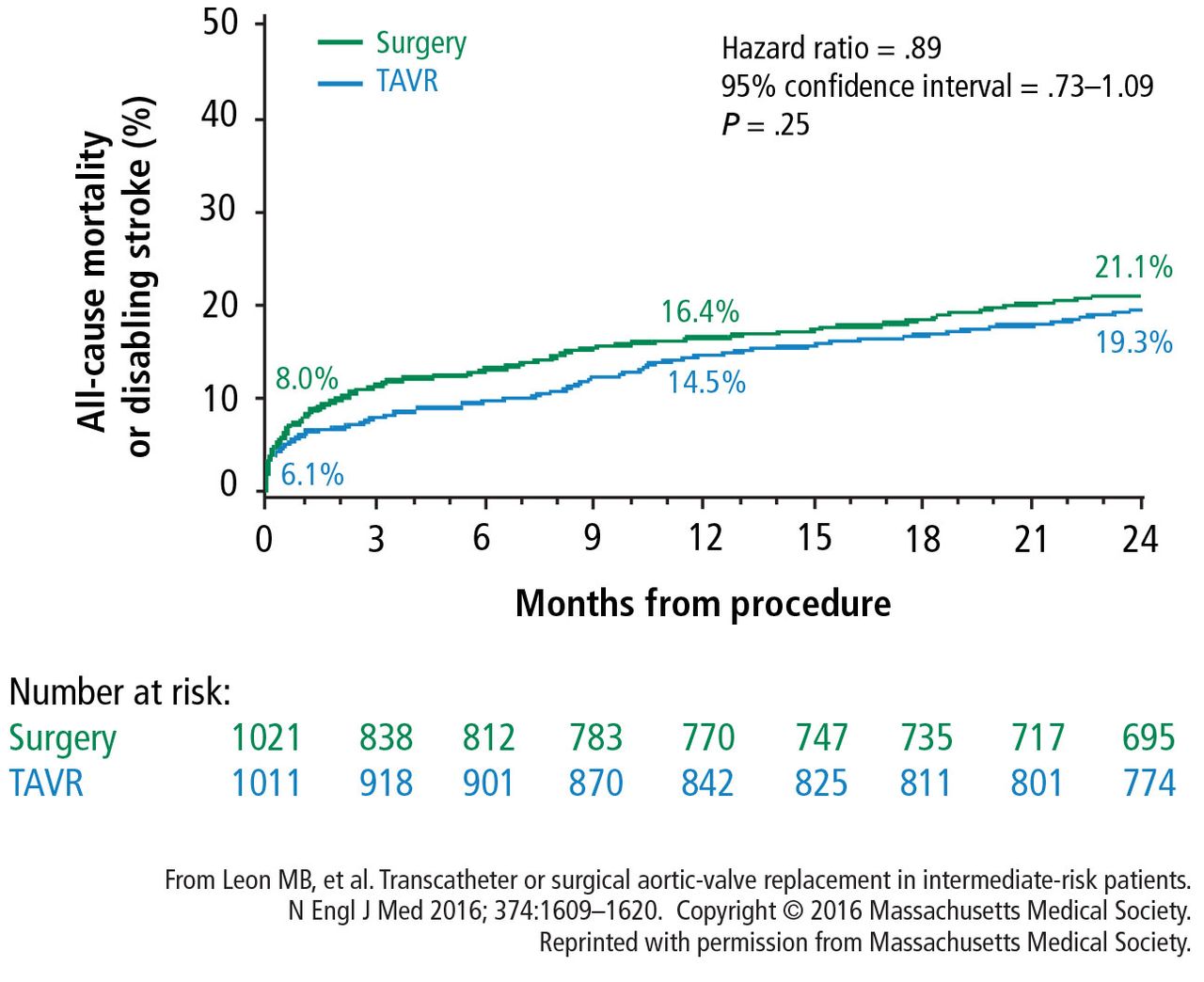
The PARTNER 2A and PARTNER S3i trials evaluated TAVR in intermediate-risk patients. In PARTNER 2A, 2,032 intermediate-risk patients were randomized to either TAVR or SAVR. Results after 2 years showed no difference between TAVR and SAVR in the primary end point of all-cause mortality or disabling stroke at 24 months (rates 19.3% vs 21.1% for SAVR) (Figure 1).1

All-cause mortality or disabiling stroke rates for TAVR vs SAVR in intermediate-risk patients during the PARTNER 2A trial showed no statistical difference.
SAVR = surgical aortic valve replacement; TAVR = transcatheter aortic valve replacement
A subanalysis of the transfemoral-access cohort provided additional support for TAVR. It showed that the rate of death and stroke in this cohort began to trend more favorably for TAVR. At 24 months, the difference in the primary end point was statistically significant in favor of TAVR (16.3% vs 20.0% for surgery; P = .04).1
One potential reason to explain the data in favor of TAVR was the introduction of the Sapien 3 valve midway through the PARTNER 2 trial. The FDA allowed the device to be evaluated in a propensity-score analysis comparing TAVR with the Sapien 3 valve vs results for the surgical arm in the PARTNER 2A trial in intermediate-risk patients.6 Results showed a 75% lower rate of all-cause mortality at 30 days with TAVR (1.1% vs 4.0% for surgery), which extended out to 12 months (7.4% vs 13.0%). Rates of disabling stroke were similar: 30-day rates were 1.0% for TAVR vs 4.4% for surgery; 12-month rates were 2.3% vs 5.9%. Data for combined mortality and stroke reflected the differences: 3.7% for TAVR vs 9.7% for SAVR at 30 days, and 10.8% vs 18.8% at 12 months (Figure 2). Both the noninferiority data and superiority data on the primary end point of mortality and stroke were statistically significant for TAVR vs SAVR (P < .001).6,7

The 1-year rates for all-cause mortality and all stroke show better outcomes for TAVR vs SAVR.7
Based on these data, in August 2016, the FDA approved the Sapien valves for use in patients with aortic valve stenosis who are at intermediate risk of death or complications associated with open-heart surgery. If the differences in outcomes reported during the PARTNER S3i trial are extrapolated to the total number of valve replacement surgeries performed worldwide, the potential number of patients who may benefit from TAVR is substantial.
DOWNSIDE OF TAVR
Although results with TAVR appear promising, there are important issues to address before it can be adopted in a wider patient population (ie, low-risk patients). These primarily focus on the following:
Stroke
Paravalvular leak
Need for pacemaker replacement
Valve durability
Leaflet immobility or valve thrombosis.
Stroke
The incidence of stroke associated with TAVR is a concern, but it has decreased with the introduction of the Sapien 3 valve. In the PARTNER 2 trial, the 30-day stroke rate in intermediate-risk patients who received the Sapien 3 valve was 2.6%.1 This compares with a 5.6% overall rate in the PARTNER 1A trials using the first Sapien valve.2 The rate of stroke events is expected to decrease further as TAVR is expanded into healthier populations with better vasculature.
Paravalvular leak
Rates of moderate or severe paravalvular leak at 30 days have also decreased with the Sapien 3 valve and were 4.2% overall in the PARTNER S3i trial.6 These rates have ranged from 11.5% overall in the PARTNER 1A trial2 to 4.2% in the PARTNER 2B trial1 that used the Sapien XT valve for transfemoral-access TAVR.
New pacemakers
The percentage of TAVR procedures that result in a new requirement for a pacemaker increased to about 11% in 2014, up from 6.8% in 2012 to 2013.8 The requirement for a new pacemaker within 30 days following TAVR appeared to decrease again in the PARTER 2 trial, to 8.5%.1
Durability
Evidence is emerging showing the limited durability of bioprosthetic aortic valve. Multiple studies have reportedly shown this, and this is true for all tissue valves, including those surgically inserted. A study assessing data from 357 patients showed that structural valve degeneration begins at 7 years post operatively. By 10 years, only about 86% of valves were free from degeneration. At 12 years, that dropped to 69%.9
A study comparing TAVR vs SAVR showed that under identical loading conditions and with identical leaflet tissue properties, leaflets of valves placed via TAVR sustained higher stresses, strains, and fatigue damage.10
Overall, these results provide the possibility that TAVR valves may have reduced valve life compared with SAVR valves. Unknown durability may be an issue to consider when evaluating TAVR for implantation in intermediate- and low-risk patients.
Leaflet immobility and valve thrombosis
In the past 2 years, the problem of potential subclinical valve leaflet thrombosis, on both surgically inserted and TAVR valves, has emerged.11 The FDA is monitoring these complications because of their potential impact on the safety and efficacy of these valves.
This complication was first reported as an unexpected finding of reduced leaflet motion on 4-dimensional computed tomography, a sign suspicious for valve thrombosis, in a subgroup of patients evaluated 30 days after implantation.12 A study from Denmark found a 7% incidence of valve thrombosis in TAVR valves. They reported that warfarin could prevent thrombosis.13
At the Heart Hospital Baylor Plano, our TAVR team has identified approximately 50 cases of thrombosis that caused partial valve occlusion. Administering warfarin for 3 months resolved the thrombosis in virtually all cases. In 1 case, a thrombosed valve was surgically explanted with good patient outcome. Pathological analysis confirmed that reduced leaflet motion seen on 4-dimensional CT was valve thrombosis, as suspected by imaging specialists.14
IS TAVR APPROPRIATE FOR INTERMEDIATE-RISK PATIENTS?
Although there are ample data supporting the use of TAVR in intermediate-risk patients, SAVR remains the most effective option in certain clinical situations:
Younger patients who will need valve replacement later in life
Bicuspid valves with eccentric bulky calcification
Aortopathy (aortic disease above the valve)
Small calcified roots
Severe calcification of left ventricular outflow tract
Low-lying coronary arteries (typically, ≤ 6 mm from the aortic annulus)
Severe septal bulging
Severe mitral regurgitation and/or tricuspid regurgitation
Conduction system disease that puts the patient at high risk for pacemaker implantation
Valve replacement in valves with a diameter 20 mm or smaller.
Nevertheless, outcomes seem to support TAVR in intermediate-risk patients. At the Heart Hospital Baylor Plano, 30-day outcomes with the Sapien 3 valve have shown all-cause mortality of 1.1% and all-stroke mortality of 2.6% (1.0% for disabling stroke). Large registries of the Sapien 3 valve have reported similar outcomes at 30 days: mortality 1%, disabling stroke 2%, major vascular complications 2%, and moderate to severe paravalvular leak 2%.15
Overall, the rates of major vascular complications and of life-threatening bleeding are 2%, and the need for new pacemakers is 4%. Results from several trials support TAVR as an alternative to surgery in intermediate-risk patients. In patients who are candidates for transfemoral access, TAVR may provide additional clinical advantages. However, questions about long-term durability and new requirements for pacemakers are issues for TAVR use in intermediate-and low-risk patients. More data are needed to answer these questions.
At the Heart Hospital Baylor Plano, the number of TAVR procedures from 2012 to 2015 increased from 49 cases to 215, while the number of SAVR procedures remained constant (166 in 2012 and 162 in 2015). During that time, outcomes improved dramatically: in-hospital mortality rates dropped from 2% to 0% and 30-day mortality dropped from 3% to 0%. There have been 227 consecutive SAVR patients with no in-hospital or 30-day mortality and 261 consecutive TAVR patients with no mortality.
These results support initiating clinical trials of TAVR in low-risk patients. In 2016, the FDA approved TAVR valves for 2 clinical trials in patients with aortic stenosis who are at low risk of surgical mortality. These large clinical trials, each with about 1,200 patients, are expected to provide data that will help determine whether TAVR is a safe and effective option for low-risk patients.
Footnotes
This article is based on Dr. Brown’s presentation at the Sones/Favaloro Scientific Program, “Transforming the Delivery of Cardiovascular Care: Research and Innovation in the Heart & Vascular Institute,” held in Cleveland, OH, November 18, 2016. The article was drafted by Cleveland Clinic Journal of Medicine and was then reviewed, revised, and approved by Dr. Brown.
Dr. Brown reported no financial interests or relationships that pose a potential conflict of interest with this article.
- Copyright © 2017 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.