


ABSTRACT
Outcomes for patients with coronary artery disease (CAD) have improved in the past 20 years likely due to advances in clinical care such as angiotensin-converting enzyme inhibitors, antiplatelet agents, and reduced time to cardiac cauterization procedures. But how have the risk factors for CAD changed in the past 2 decades? Analysis of nearly 4,000 patients with ST-elevation myocardial infarction (STEMI) at a tertiary care center found that patients presenting with acute STEMI are younger and more obese than in the past. The prevalence of smoking, hypertension, and diabetes mellitus is also increasing. Primary and secondary prevention and aggressive efforts to modify risk factors for CAD is essential for further improvement in cardiovascular outcomes.
Advances in treatment of CAD have improved patient outcomes over the past 20 years.
Prevalence of risk factors for CAD has increased over the past 20 years in patients presenting with STEMI with patients now more likely to be younger and with higher prevalence of smoking, obesity, hypertension, and diabetes.
Emphasis on primary and secondary prevention to reduce CAD risk factors is needed to improve outcomes and reduce the cost of care.
Many clinical improvements in treating patients with acute ST-elevation myocardial infarction (STEMI) have been realized in the past 20 years, including angiotensin-converting enzyme inhibitors, antiplatelet agents, and reduced time to cardiac cauterization procedures for acute myocardial infaction.1 Presumably, primary and secondary prevention measures have also resulted in changes in coronary artery disease (CAD) risk factors over the past 20 years. We sought to quantify mortality outcomes for patients treated in our catherization laboratory and to investigate trends in cardiovascular risk factors in patients during the same period.2
STEMI OUTCOMES
Data from our catherization laboratory database of 3,913 patients treated for STEMI at our tertiary care center from 1995 through 2014 were analyzed. To evaluate outcomes over time, patients were grouped based on years treated in 5-year increments resulting in 4 groups spanning 20 years.2
Analysis showed reduced mortality rates for patients with STEMI over the past 20 years: the 30-day mortality rate in patients treated from 2010 to 2014 was 7.8%, nearly half the rate of 14% in patients treated from 1995 to 1999. The trend in reduced mortality rates for patients with STEMI was also noted at 1 year and 3 years (Figure 1).3
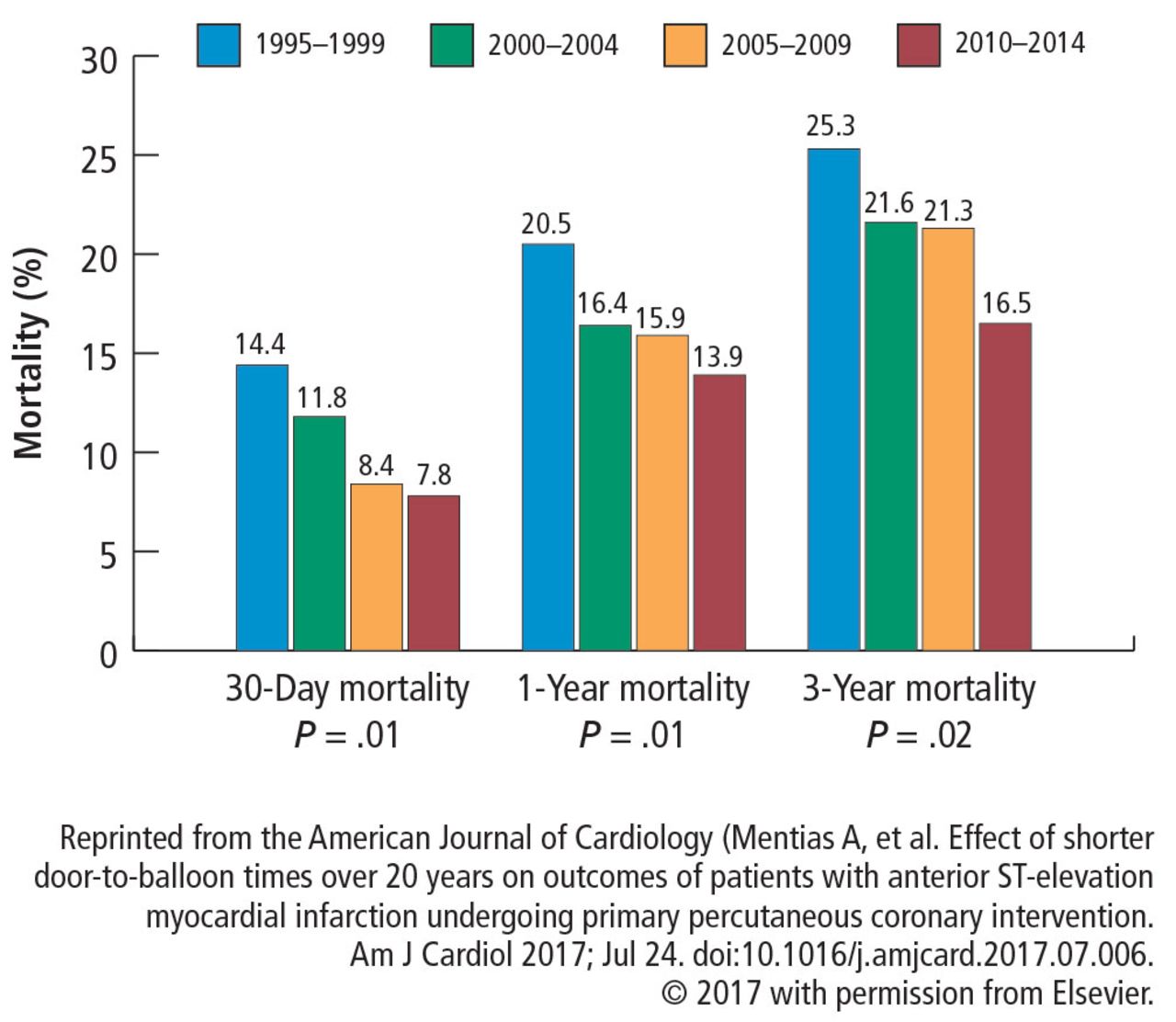
Rates of 30-day, 1-year, and 3-year mortality for patients treated for ST-elevation myocardial infarction.
CARDIOVASCULAR RISK FACTORS
A reduction in mortality rates in patients treated for STEMI is to be expected over time, given the improvements in clinical practices and procedures and novel medications developed since 1996. But it is also possible that patients presenting with STEMI are healthier than in the past as a result of primary prevention efforts to minimize CAD risk factors and changes in CAD risk factors over time.
To determine whether CAD risk factors have changed over time, we analyzed the risk factors in the 3,913 patients treated for STEMI in our database. Risk factors included in the analysis were:
Age
Sex
Diabetes mellitus
Hypertension
Smoking
Hyperlipidemia
Chronic renal impairment (serum creatinine greater than 1.5 mg/dL)
Obesity (body mass index greater than 30 kg/m2).2
The prevalence of risk factors was determined in the entire cohort as well as in the 34% (n = 1,325) of patients previously diagnosed with CAD. The trend in risk factors in patients previously diagnosed with CAD could indicate the effectiveness of secondary prevention efforts compared with primary prevention in the broader patient population.
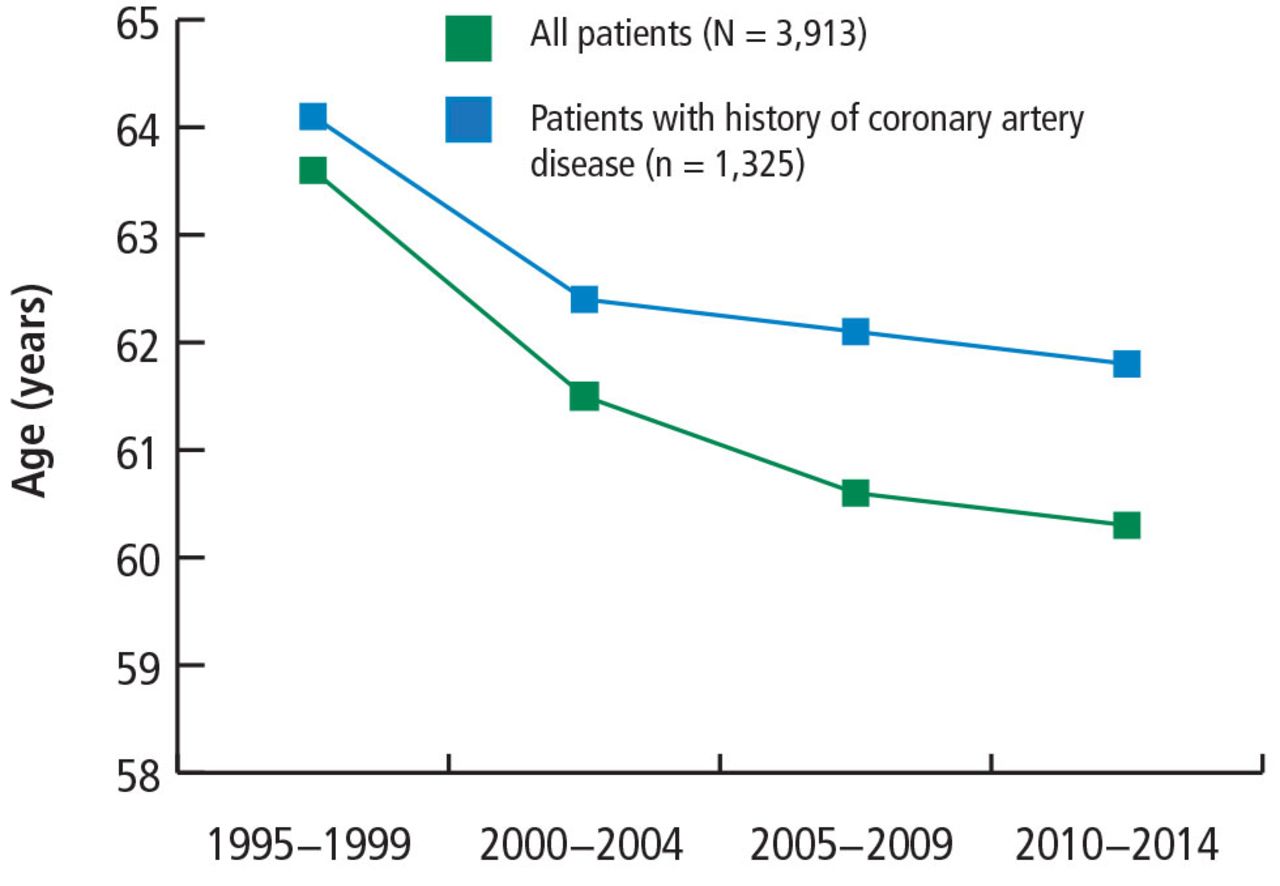
Results show that the average age of patients presenting with STEMI has decreased from 64 to 60 over the past 20 years, and the trend is consistent regardless of a history of CAD (Figure 2).2
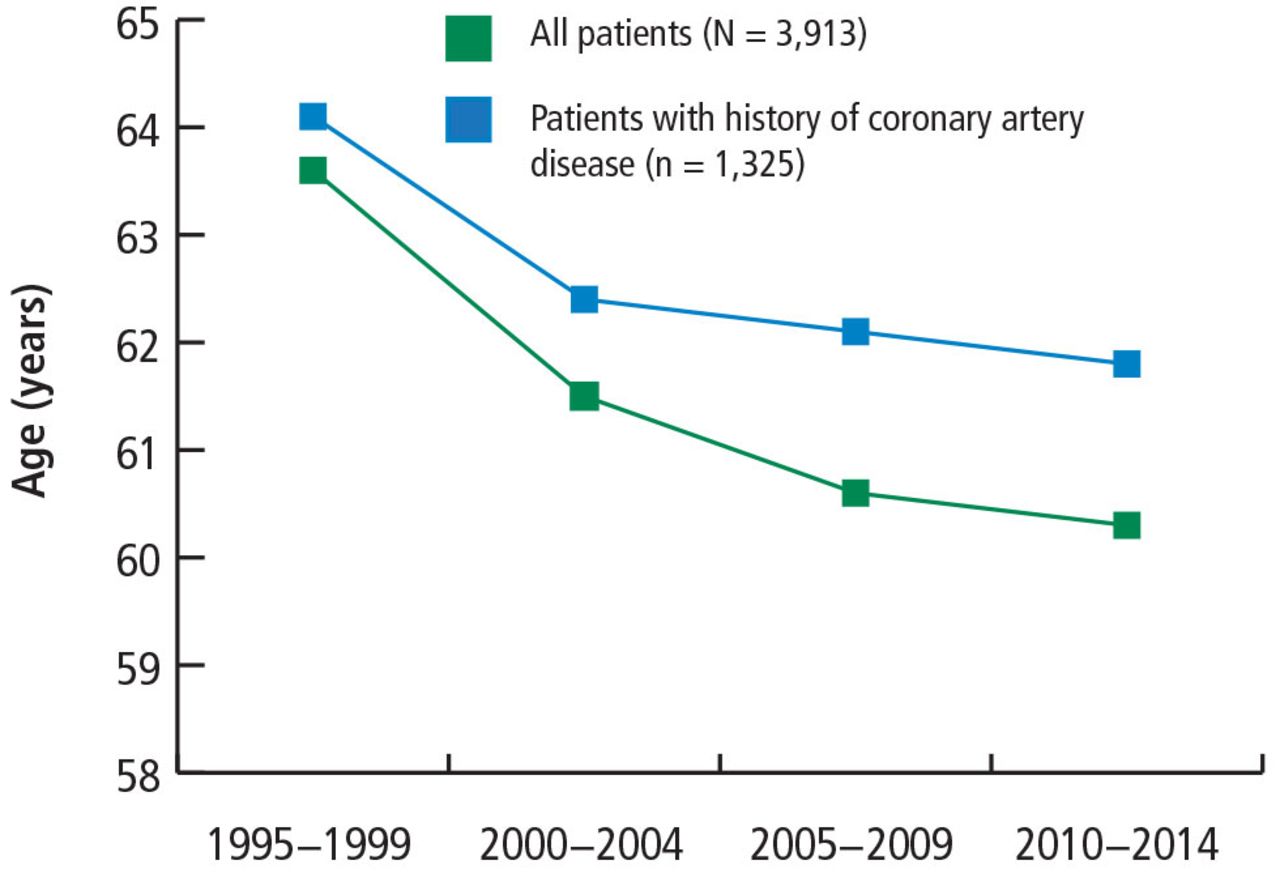
Patient age at presentation with ST-elevation myocardial infarction.
Based on data from reference 2.
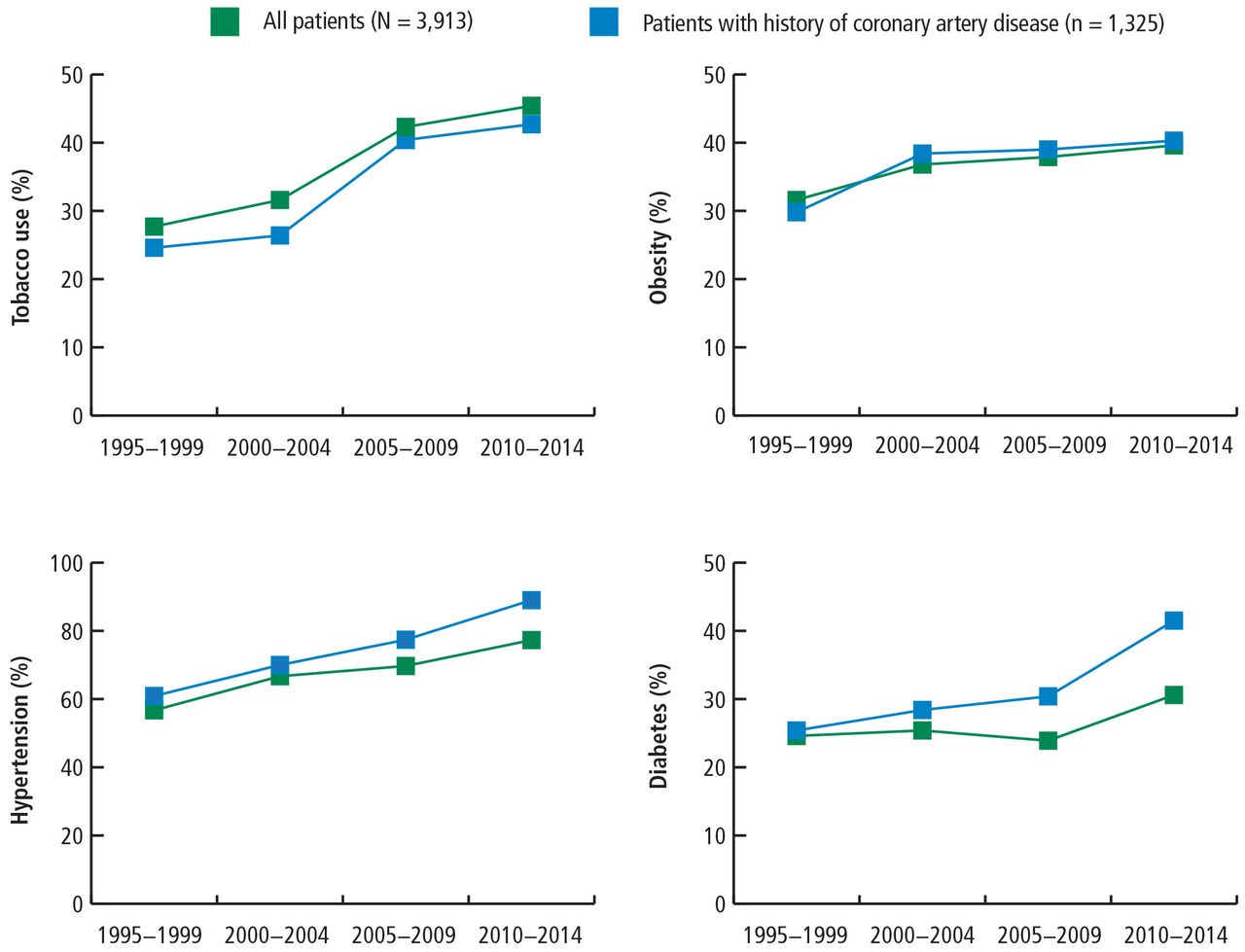
The prevalence of the cardiovascular risk factors of tobacco use, obesity, hypertension, and diabetes in patients with STEMI increased from 1995 to 2014, as well as patients with a history of CAD (Figure 3).2
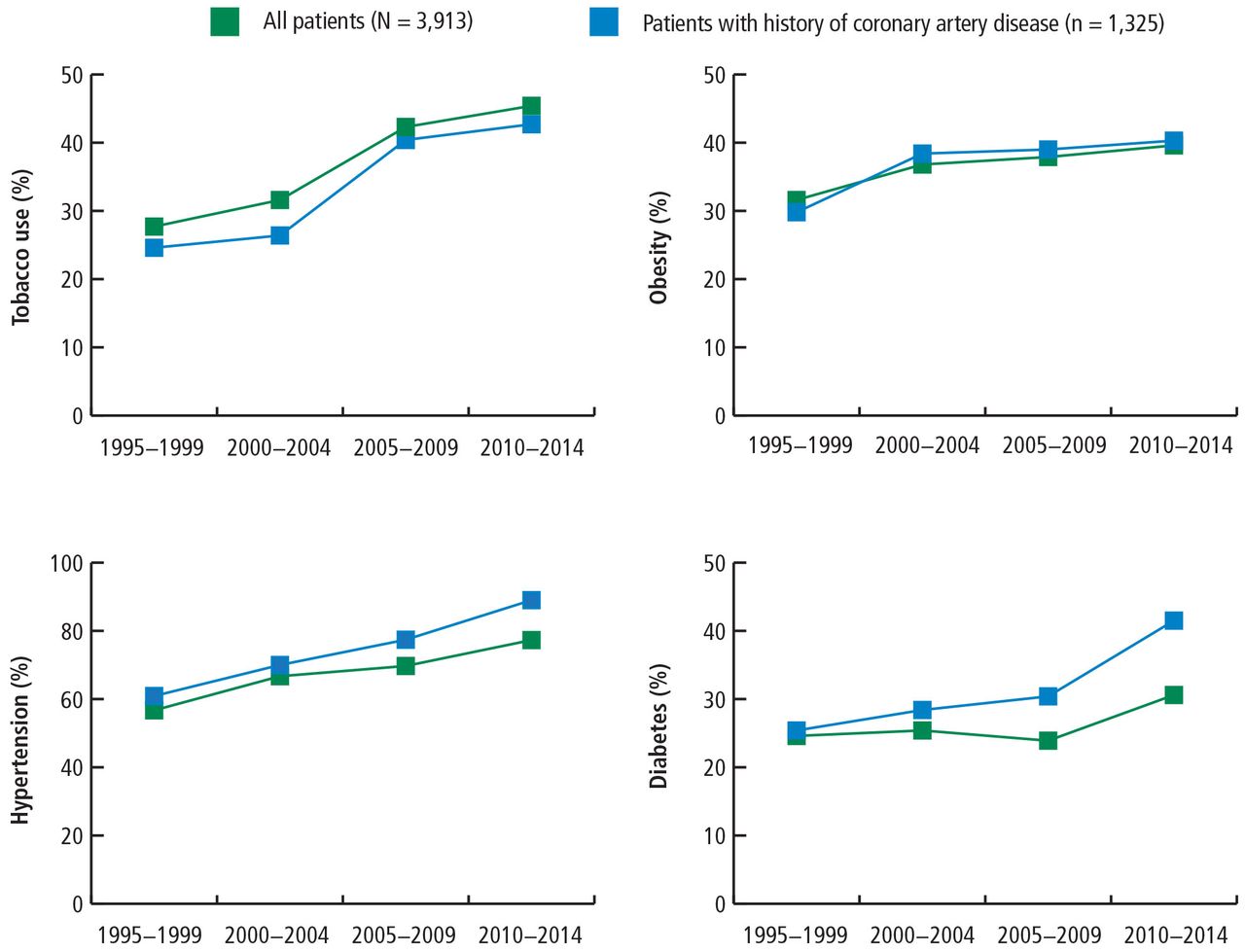
Prevalence of risk factors in patients presenting with ST-elevation myocardial infarction over time.
Based on data from reference 2.
These data suggest that despite a better understanding of cardiovascular risk factors, the cardiovascular risk profiles of patients with acute STEMI have deteriorated over the past 20 years: patients are younger at presentation and more likely to be obese, to smoke, and to have hypertension and diabetes. These trends hold true in patients with and without a history of CAD, suggesting primary and secondary prevention efforts are ineffective.
TRENDS IN THE UNITED STATES
To evaluate whether geographic or patient population characteristics could have biased our results, we analyzed mortality and risk factor data from the National (Nationwide) Inpatient Sample (NIS) for patients presenting with STEMI (N = 445,319), non-STEMI (N = 915,341), and stroke (N = 937,425) from 2003 to 2013.4,5
Mortality rates
Consistent with the trend in our data, the 10-year NIS data showed a lower mortality rate in 2003 compared with 2013 in patients admitted with extreme-severity STEMI (22% vs 18%), non-STEMI (13% vs 8%), and stroke (15% vs 10%), as well as in patients with moderate-severity disease.4
Risk factors
NIS data also revealed a reduction in the percentage of patients age 75 and older admitted for STEMI, non-STEMI, and stroke consistent with younger age at presentation and an increased prevalence of CAD risk factors from 2003 to 2013 (Table 1).4 The percentage of female patients admitted is also decreasing, indicating the increasing prevalence of these conditions in males.
Percent of patients admitted in 2003 and 2013 with ST-elevation MI, non-ST-elevation MI, and stroke by age, risk factor, female sex, and uninsured status
Unfortunately, the prevalence of these relatively preventable CAD risk factors is moving in the wrong direction. The prevalence of smoking in patients presenting with non-STEMI, STEMI, or acute stroke is higher than in the past, contrary to the nationwide trend of decreasing rates of smoking.6 The increased rate of obesity evident in our data and the NSI data is consistent with rising obesity rates in the United States, which went from 30% to 37% in adults and from 14% to 17% in youth from 2000 to 2014.7 The percentage of adults with diabetes has increased tremendously in the United States, from 4.4% of adults in 1994 to 9.1% of adults in 2015.8 The rise in diabetes has led to increased rates of CAD, heart disease, and stroke in patients with diabetes.9
OPPORTUNITIES AHEAD
Despite improved STEMI outcomes, trends in cardiovascular risk profiles are deteriorating, emphasizing the critical need to educate people about primary and secondary prevention. Folsom et al10 conducted an analysis of a community-based sample to determine the prevalence of ideal cardiovascular health based on 4 ideal health behaviors (nonsmoking, low body mass index, adequate physical activity, healthy diet) and 3 ideal risk health factors (total cholesterol, blood pressure, and moderate glucose control).10 Each of the 7 behavior and risk factors was defined by ideal, intermediate, and poor characteristics. Very few study participants (0.1%) had ideal levels for all 7 healthy cardiovascular behaviors and risk factors, and over 82% had poor levels for all 7 behaviors and characteristics. The need to educate and improve cardiovascular health exists for both adults and youth. Measures of cardiovascular health in the United States indicate that 18% of adults age 50 or older and 46% of youth (ages 12 to 19) have 5 or more of the 7 health cardiovascular behaviors and risk factors at ideal levels.11
Improvement in primary and secondary prevention measures may also present opportunities to contain or reduce the cost of care. Thus far, according to NIS registry data from 2003 to 2013, the mean adjusted cost of hospitalization for patients with STEMI increased about 14%, remained about the same for patients with non-STEMI, and increased about 3% for patients with stroke.4
CONCLUSION
Advances in clinical care have improved outcomes for patients with CAD during the past 2 decades. These gains have come despite a higher prevalence of CAD risk factors in patients. More emphasis on primary and secondary prevention to reduce CAD risk factors may further improve outcomes and possibly lower the cost of care. Aggressive encouragement of risk factor modification is necessary and should go beyond cardiologists to include primary care physicians, preventive clinics, secondary cardiovascular prevention, and population-based efforts.
Footnotes
This article is based on Dr. Kapadia’s presentation at the Sones/Favaloro Scientific Program, “Transforming the Delivery of Cardiovascular Care: Research and Innovation in the Heart & Vascular Institute,” held in Cleveland, OH, November 18, 2016. The article was drafted by Cleveland Clinic Journal of Medicine and was then reviewed, revised, and approved by Dr. Kapadia.
Dr. Kapadia reported no financial interests or relationships that pose a potential conflict of interest with this article.
- Copyright © 2017 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.