


Article Figures & Data
Figures
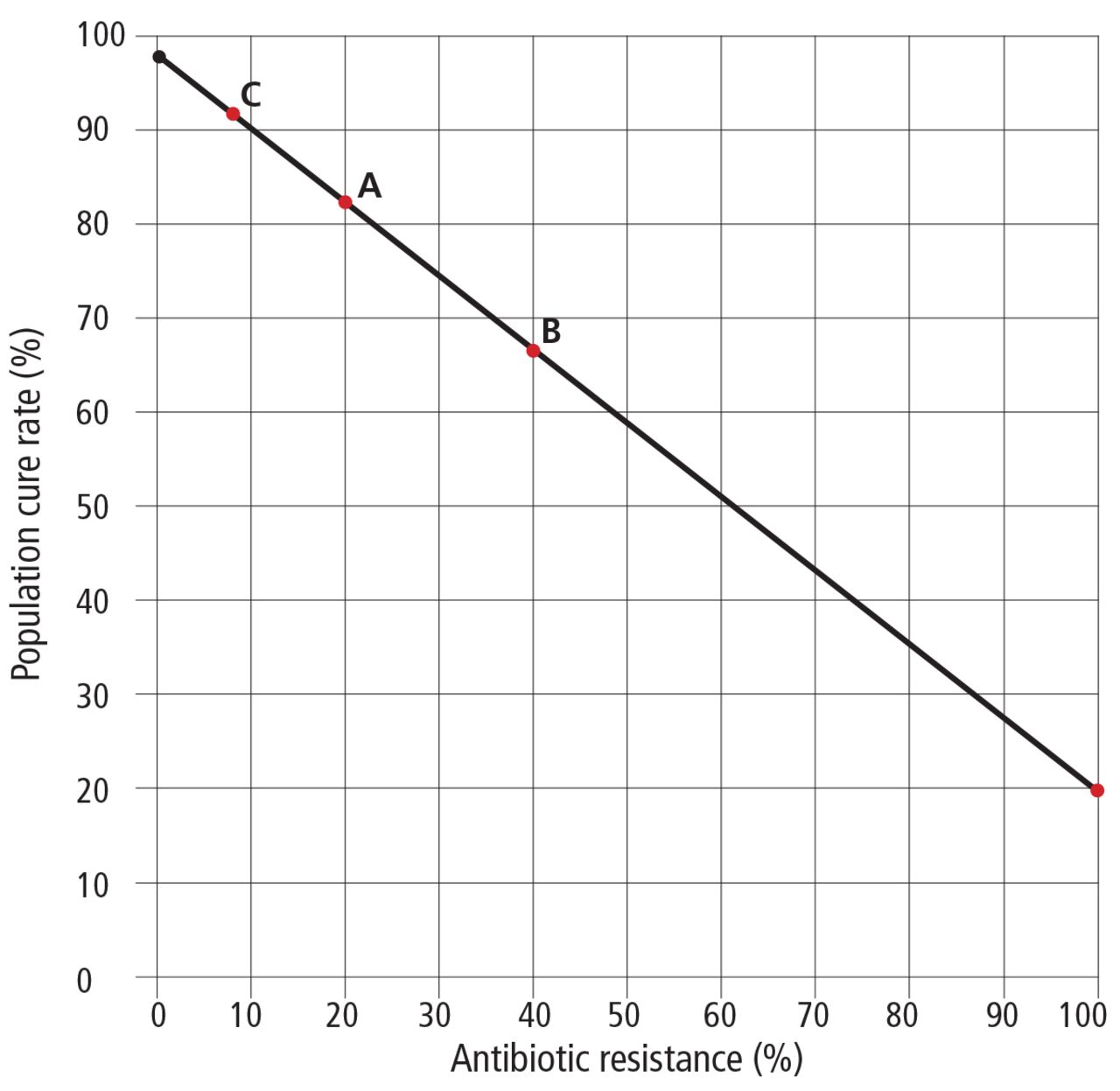
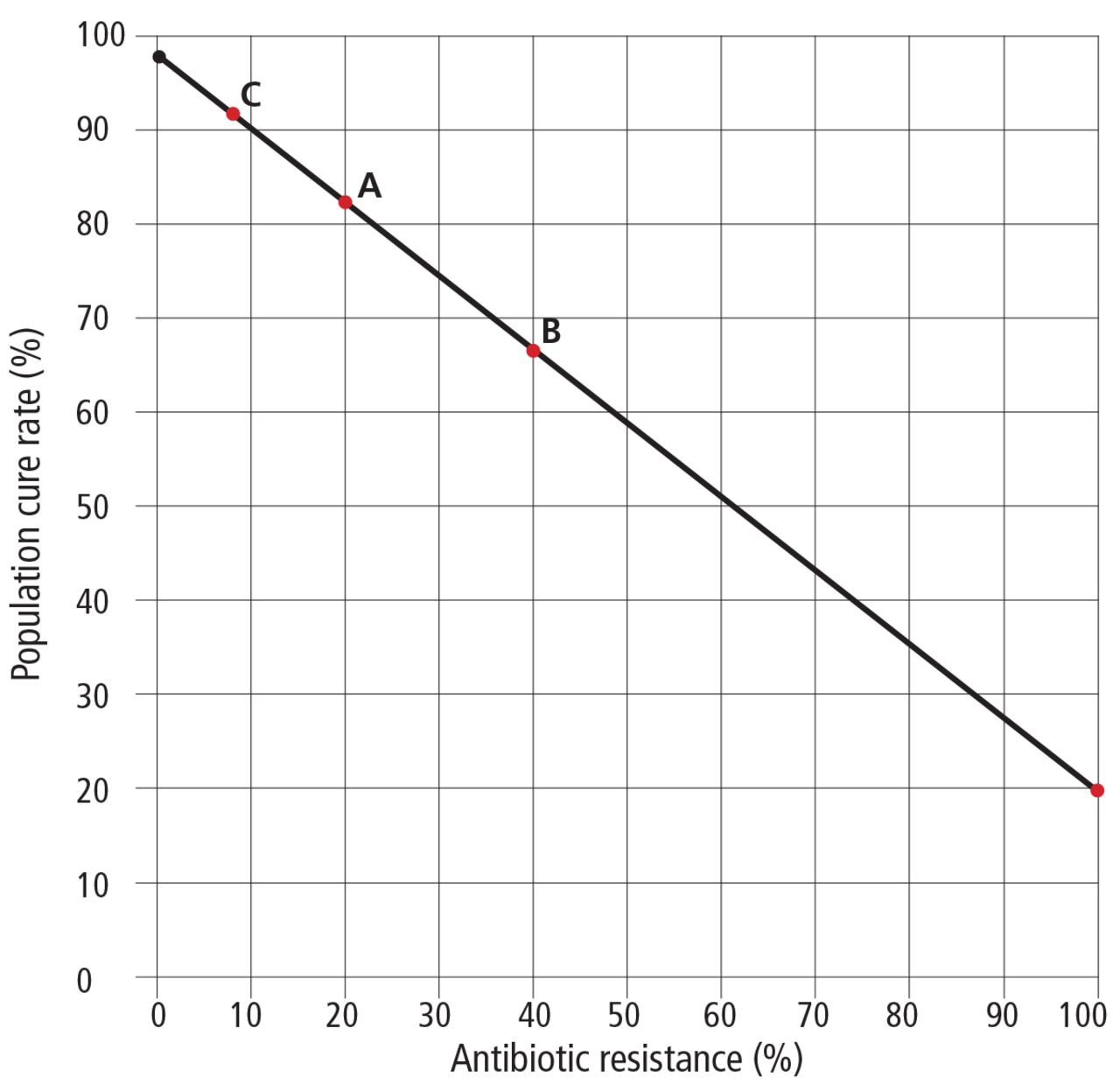
- FIGURE 1
Nomogram of expected rates of cure (vertical axis) with triple therapy (ie, either clarithromycin or metronidazole, plus amoxicillin, plus a proton pump inhibitor) for Helicobacter pylori infection if the prevalence of resistance to clarithromycin or metronidazole in the population (horizontal axis) is 20% (A), 40% (B), or 8% (C). Even if the prevalence of resistance to the clarithromycin or metronidazole component of the regimen is 100% (far right side of graph), the amoxicillin and proton pump inhibitor components of the regimen can be expected to cure approximately 20% of cases. A cure rate of at least 90% is desirable.
Based on Graham DY. Hp-normogram (normo-graham) for assessing the outcome of H. pylori therapy: effect of resistance, duration, and CYP2C19 genotype. Helicobacter 2015; 21:85-90.
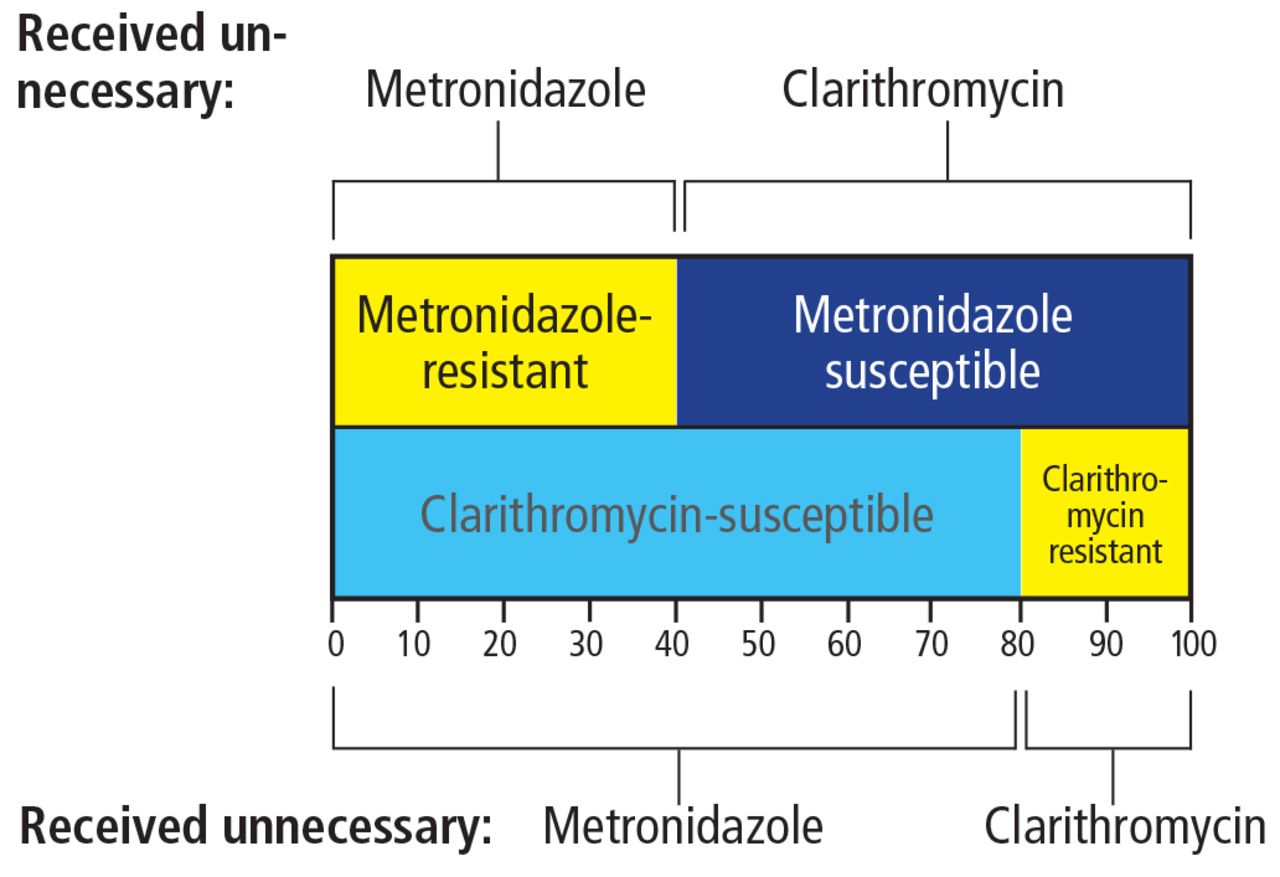
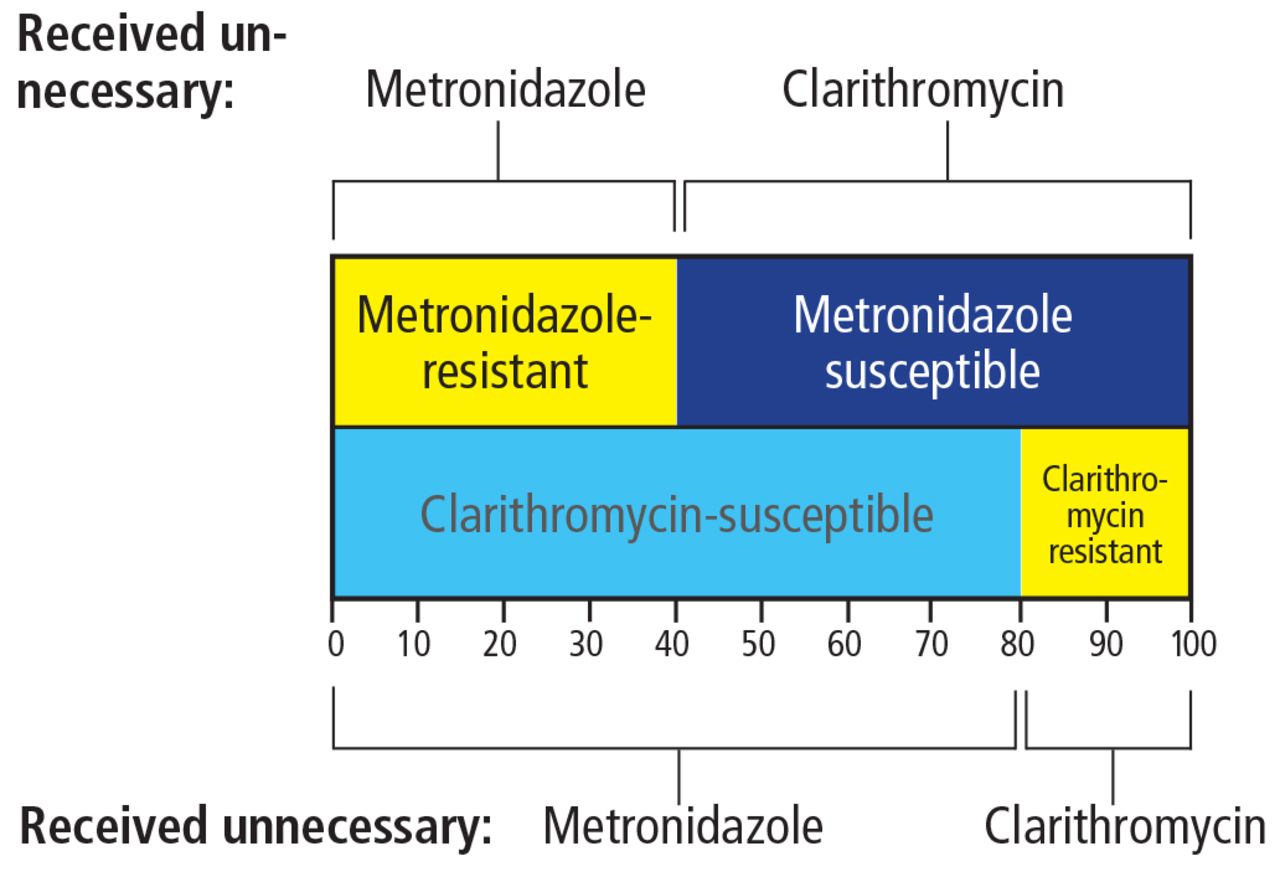
- FIGURE 2
The “dirty little secret” of concomitant therapy (the combination of amoxicillin, metronidazole, clarithromycin, and a proton pump inhibitor) for Helicobacter pylori infection is a high rate of unnecessary antibiotic use. Shown are rates of unnecessary antibiotic use in a population with 20% clarithromycin resistance, 40% metronidazole resistance, and 8% dual resistance.
Tables
Susceptibility-based, for patients with no drug allergies Clarithromycin triple therapy
(For infections susceptible to clarithromycin)
All of the following twice daily for 14 days:
Clarithromycin 500 mg
Amoxicillin 1 g
A proton pump inhibitor aMetronidazole triple therapy (For infections susceptible to metronidazole)
All of the following twice daily for 14 days:
Tinidazole 500 mg or metronidazole 500 mg
Amoxicillin 1 g
A proton pump inhibitor aFluoroquinolone triple therapy
(For infections susceptible to fluoroquinolones)
All of the following for 14 days:
A fluoroquinolone (eg, levofloxacin 500 mg once daily)
Amoxicillin 1 g twice a day
A proton pump inhibitor twice a dayaSusceptibility-based, for patients allergic to penicillin Bazzoli’s triple therapy
(For infections susceptible to clarithromycin and metronidazole)
All of the following twice daily for 14 days:
Clarithromycin 500 mg
Tinidazole 500 mg or metronidazole 500 mg
A proton pump inhibitor aBismuth quadruple therapy
(For infections resistant to clarithromycin or metronidazole)
All of the following for 14 days:
Bismuth subcitrate or subsalicylate 2 tablets 4 times daily with meals and at bedtime
Tetracycline hydrochloride 500 mg 4 times daily with meals and at bedtime
Metronidazole or tinidazole 500 mg 3 times daily with meals
A proton pump inhibitor twice a day aThese therapies are expected to achieve > 90% (often > 95%) cure rates with susceptible infections and adherent patients
↵a Preferred proton pump inhibitors are omeprazole 40 mg, lansoprazole 45 or 60 mg, rabeprazole 20 mg, or esomeprazole 20 mg; pantoprazole is not recommended as 40 mg is approximately equivalent to 9 mg omeprazole.
(After 2 or more failures with different drugs) Furazolidone quadruple therapy with tetracycline
Both of the following 4 times a day with meals and at bedtime:
Bismuth subsalicylate or bismuth subcitrate 2 tablets
Tetracycline hydrochloride 500 mg
Plus:
Furazolidone 100 mg 3 times a day with meals
A proton pump inhibitor twice daily a
All for 14 daysFurazolidone quadruple therapy with amoxicillin
All of the following for 14 days:
Bismuth subsalicylate or bismuth subcitrate 2 tablets 4 times daily with meals and at bedtime
Furazolidone 100 mg 3 times a day with meals
Amoxicillin 1 g 3 times a day with meals
A proton pump inhibitor twice daily aRifabutin therapies (see Table 3) These therapies are expected to achieve > 90% (often > 95%) cure rates with susceptible infections and adherent patients.
↵a Preferred proton pump inhibitors are omeprazole 40 mg, lansoprazole 45 or 60 mg, rabeprazole 20 mg, or esomeprazole 20 mg; pantoprazole is not recommended as 40 mg is approximately equivalent to 9 mg omeprazole.
Likely effective but not yet optimized empiric regimens Hybrid (sequential-concomitant) therapy
Both of the following twice a day for 7 days:
Amoxicillin 1 g
A proton pump inhibitor
Followed by all of the following twice a day for a further 7 days (total 14 days):
Amoxicillin 1 g
Clarithromycin 500 mg
Tinidazole 500 mg or metronidazole 500
A proton pump inhibitor bNew bismuth quadruple therapy
(amoxicillin replaces tetracycline)23
All of the following for 14 days:
Bismuth 2 tablets 2 to 4 times daily with meals and at bedtime
Metronidazole or tinidazole 500 mg 3 times daily (or 400 mg 4 times daily) with meals
Amoxicillin 1 g 3 times daily
A proton pump inhibitor twice daily for 14 days bRifabutin triple therapy33
All of the following for 14 days:
Rifabutin 150 mg once or twice daily
Amoxicillin 1.5 g twice daily
Omeprazole 20 mg (or an equivalent) every 8 hoursRifabutin-bismuth therapy34
All of the following twice daily for 14 days:
Rifabutin 150 mg
Bismuth subcitrate or subsalicylate 2 tablets
Amoxicillin 1 g
A proton pump inhibitor bPossible future regimens High-dose proton pump inhibitor-amoxicillin dual therapy
(effective for CYP2C19 poor metabolizers—see text)
Both of the following at approximately 6-hour intervals for 14 days
(can use 8-hour intervals at night):
A proton pump inhibitor
(eg, rabeprazole 40 mg or esomeprazole 40 mg)
Amoxicillin 500-750 mgVonoprazan-amoxicillin dual therapy
Both of the following for 14 days:
Vonoprazan 20 mg twice a day
Amoxicillin 500 mg every 6 hours for 14 daysa These therapies are not yet optimized to reliably achieve > 90% or preferably > 95% cure rates.
↵b Preferred proton pump inhibitors are omeprazole 40 mg, lansoprazole 45 or 60 mg, rabeprazole 20 mg, or esomeprazole 20 mg; pantoprazole is not recommended as 40 mg is approximately equivalent to 9 mg omeprazole.




{kind=link}
{kind=link}