


Article Figures & Data
Figures
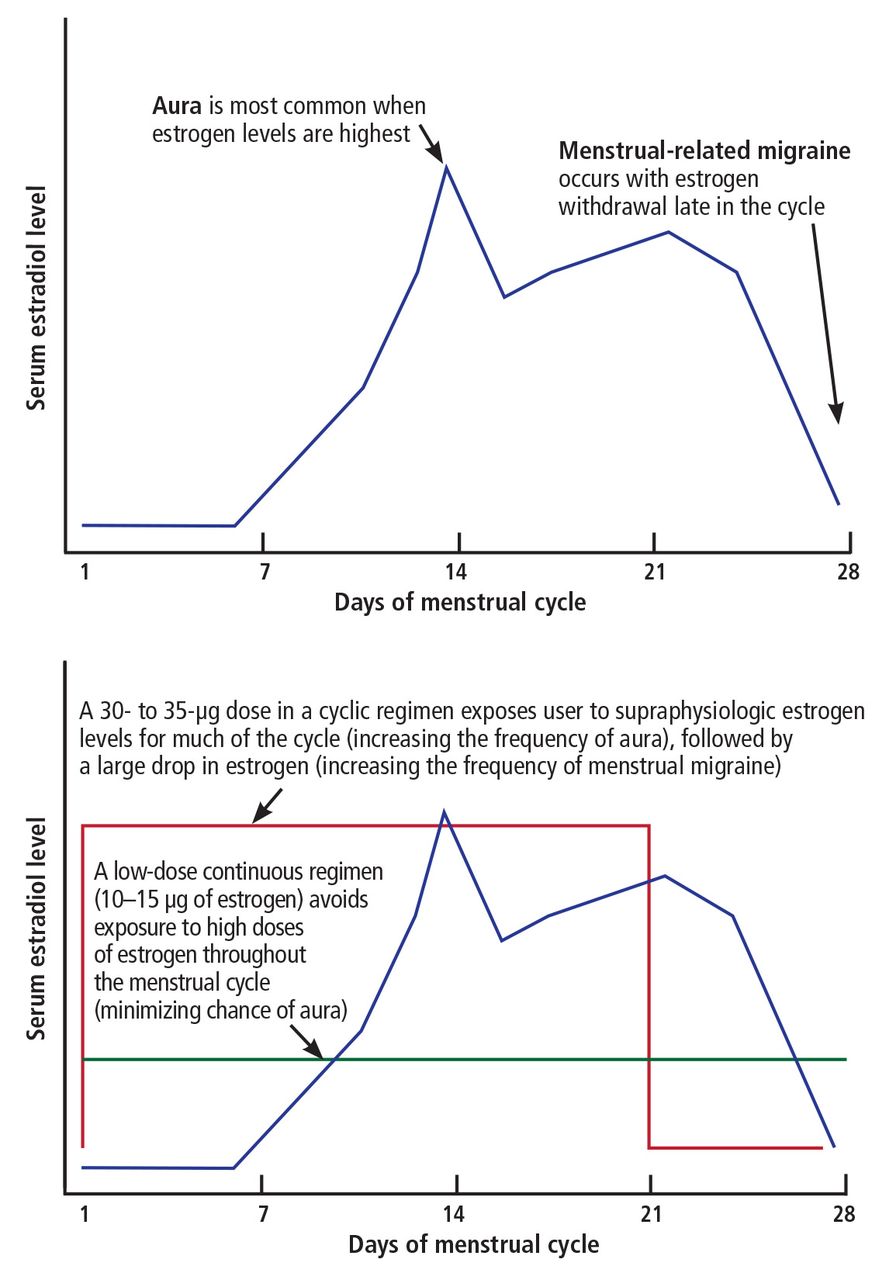
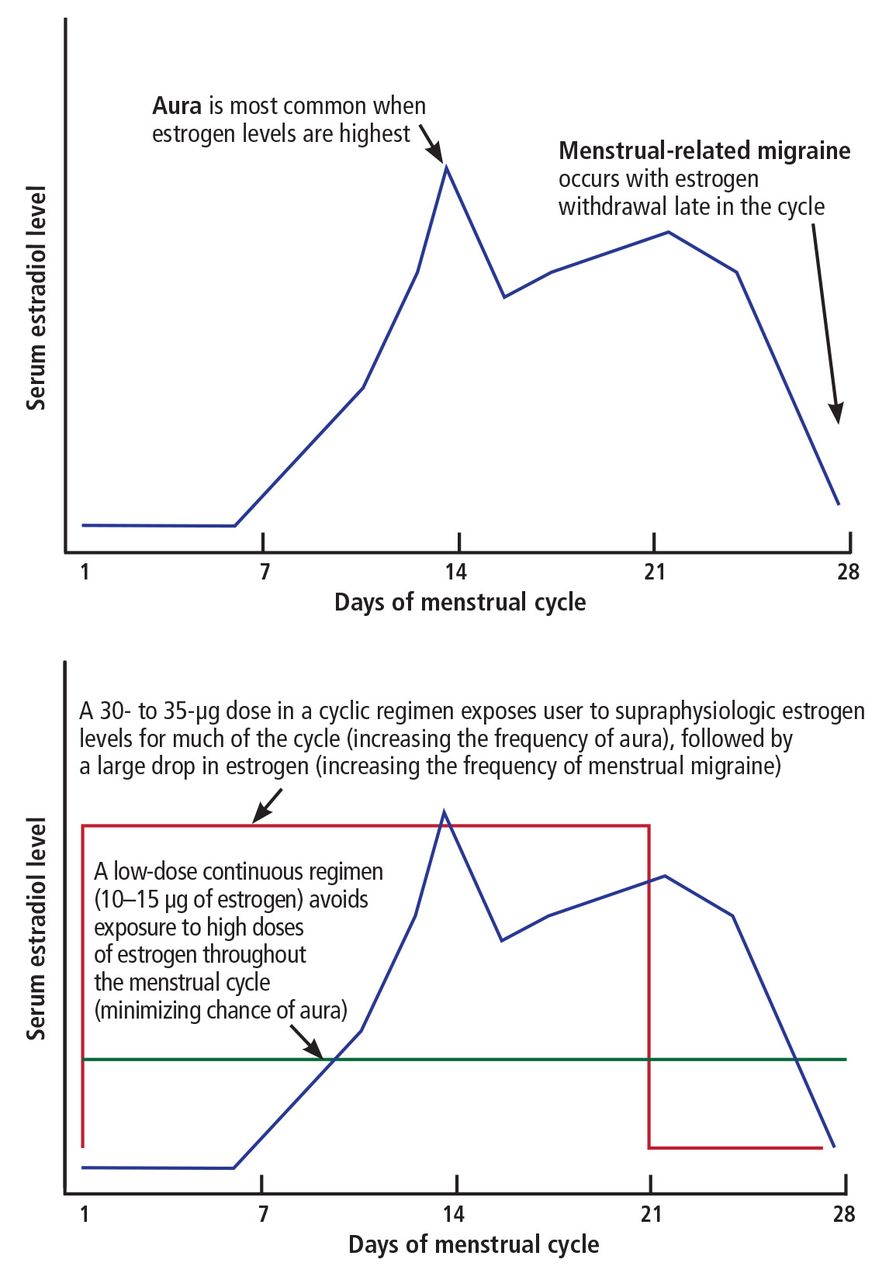
- FIGURE 1
Serum estradiol levels in the natural menstrual cycle (top) and with high-dose cyclic and low-dose continuous combined oral contraceptives (bottom).
Tables
Brand name Generic alternatives Dose Clinical pearls Continuous formulations Lybrela Ashlyna 28
Amethyst 28aEthinyl estradiol 20 µg and levonorgestrel 0.09 mg once daily for 365 days/year Can substitute any generic 20-µg ethinyl estradiol pill and continue without placebo pills NuvaRing None (though many insurance plans cover it) Vaginal ring
Delivers ethinyl estradiol 15 µg and etonogestrel 0.12 mg daily
Can be inserted once every 4 weeks to be used in a continuous fashionWomen who are sensitive to the drop in estrogen level in the last week may need to replace the ring every 3 weeks Extended formulations LoSeasonique Amethia Lo
Camrese LoEthinyl estradiol 20 µg and levonorgestrel 0.1 mg for 84 days, then ethinyl estradiol 10 µg for 7 days If a 30-µg ethinyl estradiol pill is used, will need to take it continuously to avoid triggering migraine Monthly formulations Lo Loestrin 1/10 None Ethinyl estradiol 10 µg and norethindrone 1 mg for 24 days, then ethinyl estradiol 10 µg for 2 days, then placebo for 2 days Ultra-low doses may be associated with increased breakthrough bleeding; the bleeding can improve over time Natazia None Estradiol valerate doses gradually decrease from 3 to 2 to 1 mg; dienogest dose increases from 2 to 3 mg This pill pack has a different missed-pill algorithm; refer to package insert for specific instructions ↵a Brand recently discontinued in the United States.




{kind=link}
Jump to section
- Article
- ABSTRACT
- WHAT THE GUIDELINES SAY
- EARLY ORAL CONTRACEPTIVES WERE ALL HIGH-DOSE
- DIAGNOSTIC CRITERIA FOR MIGRAINE
- MIGRAINE IS COMMON AND UNDERRECOGNIZED
- HOW ESTROGEN AFFECTS MIGRAINE
- STROKE RISK: ESTROGEN DOSE MATTERS
- STROKE RISK INCREASES WITH FREQUENCY OF MIGRAINE AURA
- CHOOSING THE OPTIMAL CONTRACEPTIVE FORMULATION
- ADVISING PATIENTS ON RISKS VS BENEFITS
- WHAT WOULD WE DO?
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics