


Article Figures & Data
Figures
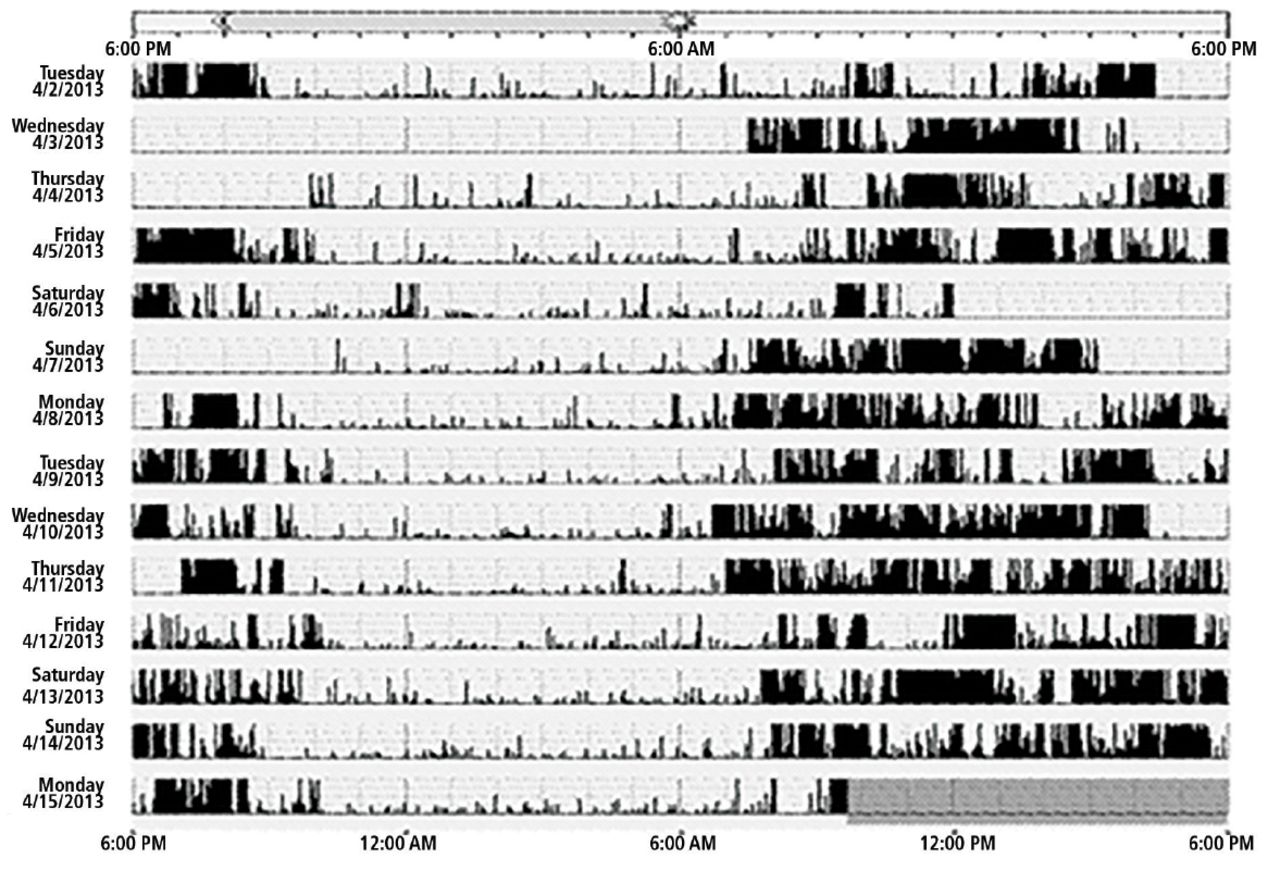
- Figure 1
Actigraphy report showing sleep schedule with relatively little variation, with bedtimes ranging from 8 to 10 PM and wake-up times from 6 to 9 AM.
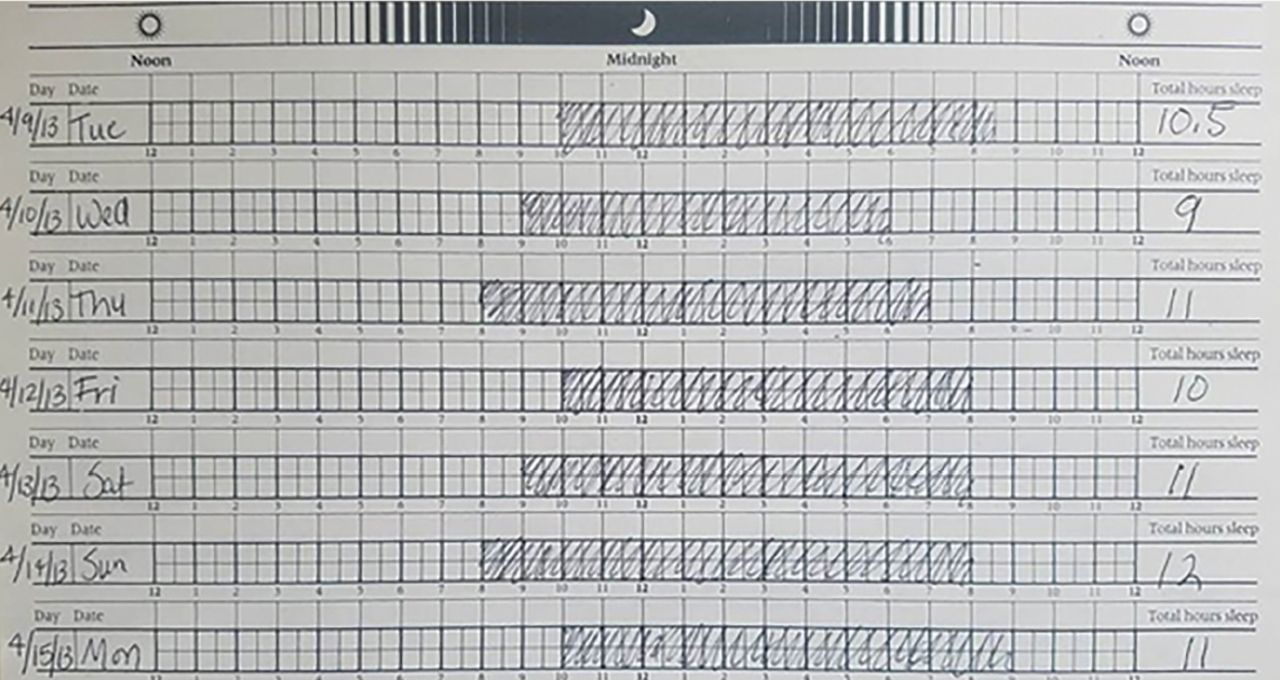
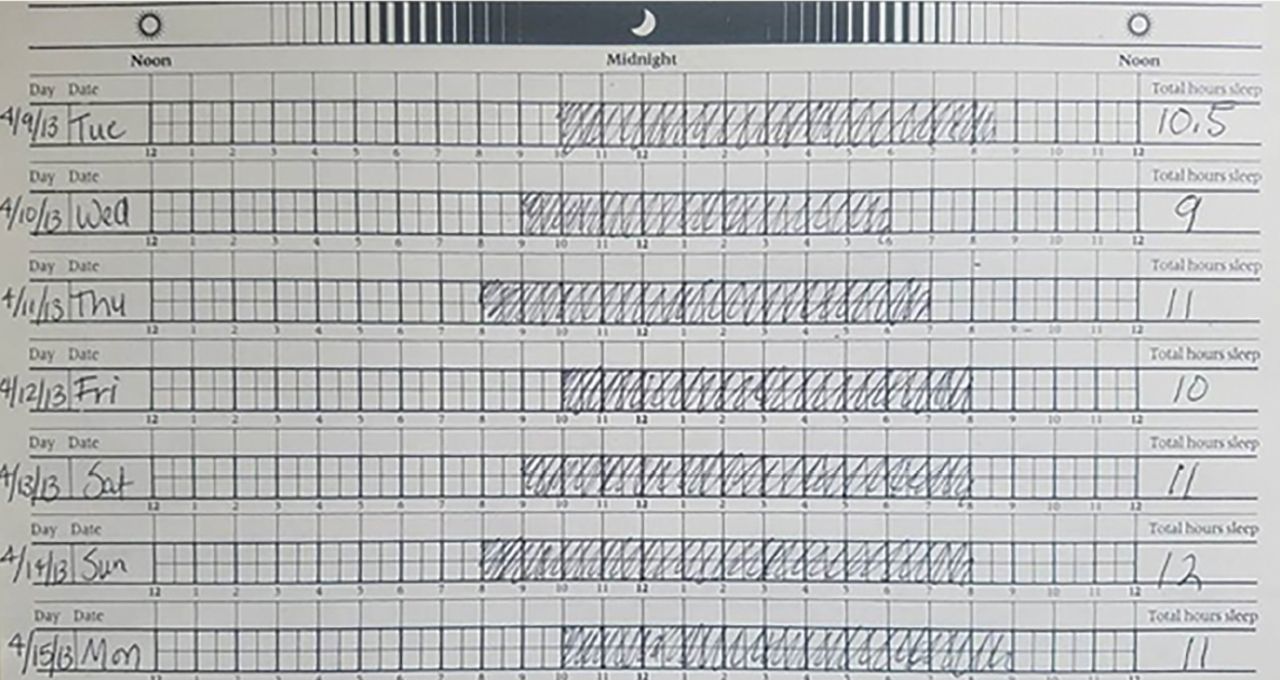
- Figure 2
Sleep log from the patient in Figure 1 shows relatively good concordance between perceived sleep schedule and actual sleep schedule.

Tables
Sleep disorders
Insufficient sleep syndrome
Delayed sleep-phase syndrome
Idiopathic hypersomnia
Sleep-disordered breathing (obstructive or central sleep apnea)
Periodic limb movement disorder
Kleine-Levin syndromeMedical disorders
Diencephalic lesions
Encephalopathy (metabolic, autoimmune, infectious)Psychiatric disorders
Depression
Bipolar disorderDrugs, other substances
Benzodiazepines
Opiates
Barbiturates
AlcoholMedication Dosage Side effects and federal schedule Modafinil 100–400 mg/day in 2 divided doses Headache, anxiety, nausea, dry mouth, anorexia, diarrhea, reduction of efficacy of oral contraceptives, Stevens-Johnson syndrome (rare)
Schedule IVaArmodafinil 150-250 mg once daily in the morning Same as modafinil Schedule IV Methylphenidate Immediate-release: 5 mg twice daily titrated up by 5-10 mg per dose weekly up to to 10-20 mg twice daily; once on stable dose, transition to extended- or sustained-release formulation Headache, anxiety, nausea, anorexia, tremor, psychosis, cardiovascular effects like hypertension and arrhythmias, abuse (rare)
Schedule IIbDextroamphetamine Short-acting: 5 mg twice daily titrated up by 5-10 mg per dose weekly up to 30 mg twice daily; once on stable dose, transition to long-acting formulation Headache, anxiety, nausea, anorexia, tremor, psychosis, cardiovascular effects like hypertension and arrhythmias, abuse (rare)
Schedule IIAmphetamine/dextroamphetamine Short-acting: 5–10 mg daily titrated up by 10 mg weekly up to 60 mg/ day or satisfactory clinical response; may add additional doses 4–6 hours after first dose; once on stable dose, transition to long-acting formulation Headache, anxiety, nausea, anorexia, tremor, psychosis, cardiovascular effects like hypertension and arrhythmias, abuse (rare)
Schedule II↵a Schedule IV drugs have a low potential for abuse and low risk of dependence. See www.dea.gov/druginfo/ds.shtml.
↵b Schedule II drugs have a high potential for abuse, with use potentially leading to severe psychological or physical dependence.
Medication Dose Side effects Sodium oxybatea 3 g/night in divided doses, once before bedtime and then 2.5-4 hours later, titrated up to 4.5-9 g in divided doses Nausea, mood swings, enuresis, headache, weight loss, sedation, sleepwalking, worsening of obstructive sleep apnea; High salt content can worsen preexisting hypertension, heart failure, and renal impairment
Schedule III, ie, moderate to low potential for physical and psychological dependence; see www.dea.gov/druginfo/ds.shtmlVenlafaxine Short-acting: 37.5–75 mg twice daily; may transition to long-acting formulation once on stable dose Nausea, dizziness, dry mouth, headache, insomnia, sexual dysfunction Fluoxetine 20–60 mg once daily Nausea, headache, dry mouth, diarrhea, sexual dysfunction Sertraline 50–150 mg once daily Nausea, headache, dry mouth, diarrhea, sexual dysfunction Protriptyline 5–10 mg twice daily Dry mouth, constipation, light-headedness, urinary retention ↵a Treats both daytime sleepiness and cataplexy.




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.