


ABSTRACT
Chronic pelvic pain in women can arise from many causes and often results in significant declines in function and quality of life. A systematic approach for evaluating patients and initiating a management plan are recommended in the primary care setting. Comprehensive management strategies may include medication, pelvic physical therapy, and behavioral interventions.
Diagnosing and managing chronic pelvic pain may be difficult, but patients are often best served when their primary care provider directs a team-based approach to their care.
A detailed history, thorough abdominal and pelvic examinations, and targeted testing facilitate the diagnosis.
As in other chronic pain syndromes, the goals of therapy should be incremental and meaningful improvements in pain, function, and overall well-being.
Chronic pelvic pain is a common clinical problem in women, as prevalent in primary care as asthma or back pain.1,2 It is often associated with lost work days and decreased productivity, increased healthcare spending, mood disorders, and negative effects on personal relationships.1–3
While specialty care referral may eventually be indicated, primary care doctors can take steps to diagnose and effectively manage the condition.
COMPREHENSIVE MANAGEMENT LED BY PRIMARY CARE
Chronic pelvic pain is defined as pain in the lower abdomen persisting for 3 to 6 months and of sufficient severity to require medical care or cause a functional disability.3 It is often detrimental to a woman’s personal life and overall health, making a comprehensive assessment and multidisciplinary approach to management especially important.
The ideal care-delivery model is the patient-centered medical home, whereby a primary care physician coordinates comprehensive care with the help of an interdisciplinary team.4,5 For complex cases, referral may be needed to other specialties (eg, obstetrics and gynecology, pain medicine) to help manage care.
TARGETED EVALUATION
Chronic pelvic pain often coexists with other systemic pain syndromes or psychiatric conditions common in primary care. Table 1 lists common causes and associated findings.
Common causes of chronic pelvic pain and associated findings
Detailed history is critical
The history is of utmost importance. Clinicians should query patients about the char acteristics of the pain as well as their medical and surgical history. Particular attention should be given to obtaining a complete gynecologic history, including pregnancy, delivery complications, dyspareunia, sexual assault, and trauma. A detailed review of systems should focus on the reproductive, gastroenterologic, musculoskeletal, urologic, and neuropsychiatric systems.
As with many pain syndromes, allowing the patient to “tell her story” helps to establish rapport and obtain a more complete assessment. Chronic pelvic pain has been associated with physical or sexual abuse as a child or adult, so is essential to foster the doctor-patient relationship and create a safe and open space for disclosure.3,6 It is important to screen women for safety at home as well as for satisfaction or dissatisfaction with their relationships with their spouse or partner and family.
Physical examination
The physical examination should be directed by the history but should always include abdominal and pelvic examinations. These should be conducted slowly and gently, assessing for areas of tenderness, masses, and other abnormalities. Clinicians should aim to pinpoint the exact anatomic locations of tenderness if possible. Ongoing dialogue facilitates this process by inquiring about pain at each point of the examination.
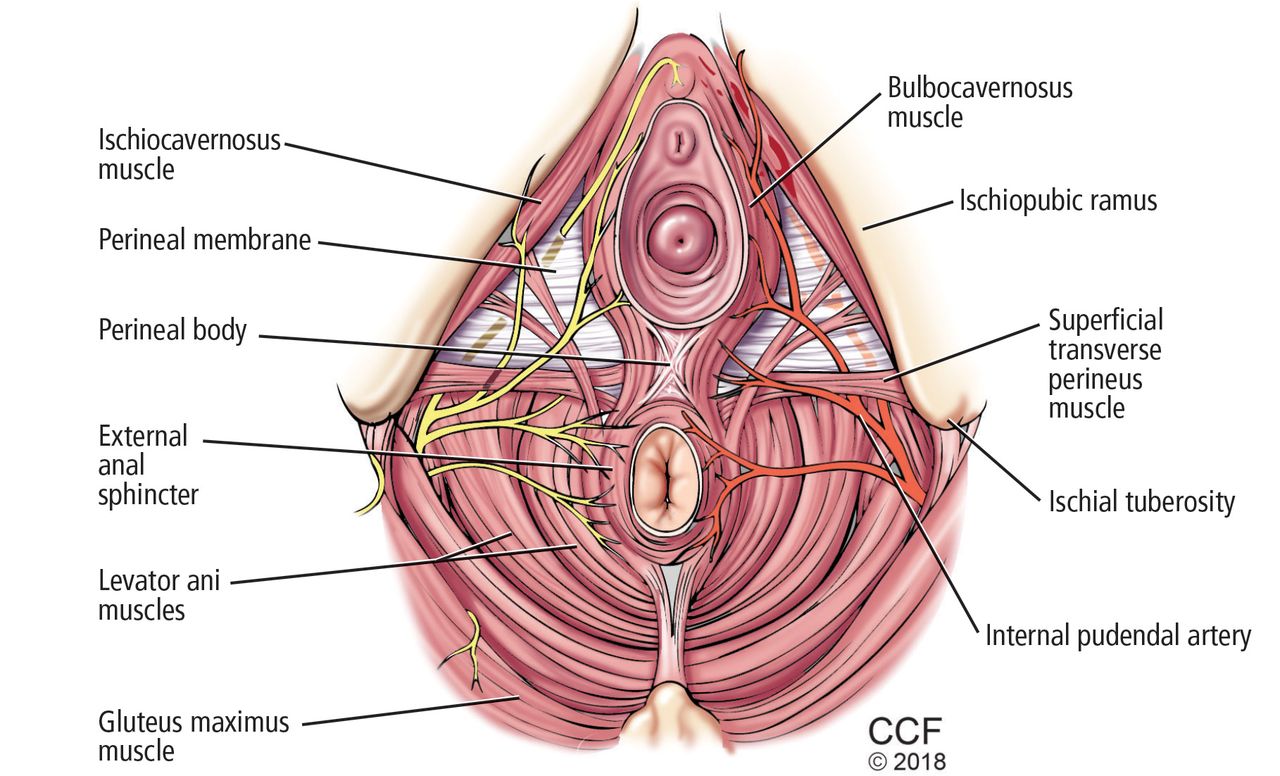
The pelvic examination should begin with visual inspection for redness, discharge, lesions, fissures, excoriations, and other abnormalities. A moistened cotton swab may be used to evaluate the vulva and vestibule for localized tenderness. The manual portion of the pelvic examination should begin with a single digit, noting any introital tenderness or spasm. Next, the levator ani muscles should be directly palpated for tone and tenderness. The pelvic floor should be evaluated with attention to tenderness of the bladder or musculoskeletal structures (Figure 1). A bimanual examination assessing uterine size and tenderness, nodularity, or a fixed, immobile uterus should be conducted.
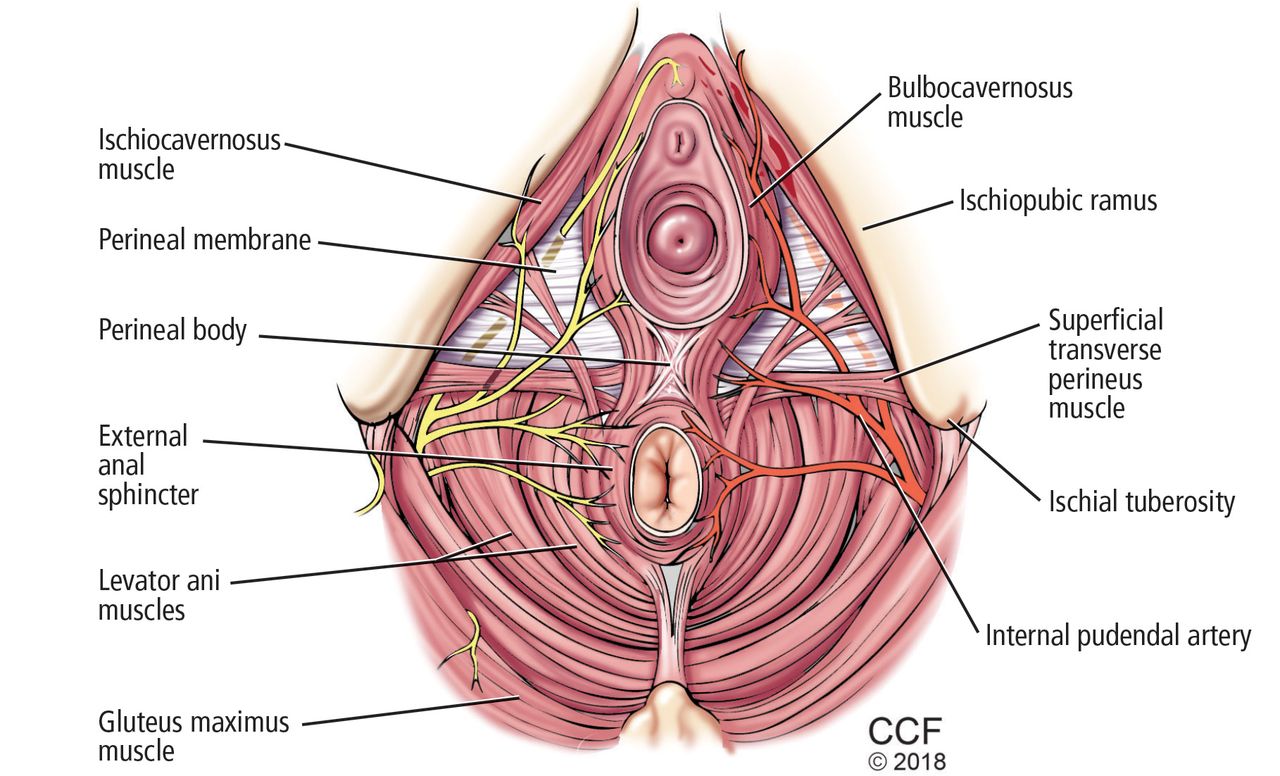
Pelvic floor anatomy. During the pelvic examination, the levator ani muscles should be directly palpated for tone and tenderness, and the pelvic floor should be evaluated with attention to any tenderness of the bladder and musculoskeletal structures.
Diagnostic workup
Because the differential diagnosis of chronic pelvic pain is broad, the diagnostic workup and testing should be based on findings of the history and physical examination. In general, extensive laboratory testing is of limited use for evaluating women with chronic pelvic pain.3,7
Urinalysis should be obtained for symptoms suggesting bladder involvement such as interstitial cystitis.
Pelvic ultrasonography can help identify pelvic masses palpated during the physical examination, but routine use of imaging is not recommended.3,7 If pelvic congestion syndrome is suspected, starting with pelvic ultrasonography is reasonable before incurring the risk or cost of computed tomography or magnetic resonance imaging.8
GENERAL TREATMENT
A holistic approach ensures that the treatment plan adequately addresses the physical, social, and psychological aspects of chronic pelvic pain.9 Treatments may include medication, pelvic physical therapy, and behavioral therapies (Table 2). As with other chronic pain syndromes commonly seen in primary care, the treatment plan may develop over multiple visits as the patient-provider relationship grows and as treatment response is evaluated.
Treatment options for chronic pelvic pain in primary care
Medical therapy
The main goals of medical therapy are to improve function and quality of life while minimizing adverse effects. General treatments include the following:
Analgesics. Nonsteroidal anti-inflammatory drugs and acetaminophen may provide pain relief, although there is weak evidence for their efficacy in treating chronic pelvic pain.9
Neuropathic agents. One of several available neuropathic agents commonly used in the treatment of chronic pain can be tried on patients who fail to respond to analgesics. Tricyclic antidepressants such as amitriptyline and imipramine decrease pain, reduce symptoms of depression, and improve sleep.10 The results of a small randomized controlled trial suggest that gabapentin is more effective than amitriptyline for reducing chronic pelvic pain.11,12 Published guidelines currently list both amitriptyline and gabapentin as first-line agents; nortriptyline and pregabalin are considered acceptable initial alternatives.9
Venlafaxine and duloxetine may help chronic pelvic pain, although specific evi dence is lacking. Duloxetine may be an appropriate choice for women with chronic pelvic pain who also experience depression and urinary stress incontinence.9
Opioids. Opioid therapy should be considered only when all other reasonable therapies have failed.10 Patients may develop tolerance or dependence, as well as opioid-induced adverse effects such as hyperalgesia.9,10 Guidelines recommend that primary care providers consult with a pain management specialist before prescribing opioids, and that patients be thoroughly counseled about the risks and side effects.9
Nerve block and neuromodulation. There is weak evidence for the use of these modalities for treating chronic pelvic pain.9 If used, they should be part of a broader treatment plan and should be performed by providers who specialize in management of chronic pain.
DISEASE-SPECIFIC TREATMENT
Endometriosis: Hormonal therapy
Pelvic pain that significantly fluctuates with the menstrual cycle may be caused by endometriosis, the most common gynecologic cause of chronic pelvic pain. Women with cyclic chronic pelvic pain should be empirically treated with hormonal therapy for at least 3 to 6 months before diagnostic laparoscopy is performed.13
Oral contraceptives, gonadotropin-releasing hormone (GnRH) analogues, progestogens, and danazol have proven efficacy, although side-effect profiles differ significantly. In a comparative trial, patients treated with GnRH analogues had more improvement in pain scores compared with those treated with oral contraceptives, but they experienced a significant decrease in bone mineral density.11 The effects on bone mineral density associated with GnRH analogue therapy can be mitigated by “add-back” low-dose hormonal therapy (norethindrone, low-dose estrogen, or a combination of estrogen and progesterone), which may also provide symptomatic relief for associated hot flashes and vaginal symptoms.11
Interstitial cystitis often accompanies endometriosis
Recognizing that chronic pelvic pain may have more than one cause is important when developing a comprehensive care plan. In terstitial cystitis coexists with endometriosis in up to 60% of patients.14 Initial treatment is pentosan polysulfate sodium, an oral treatment approved by the US Food and Drug Administration for interstitial cystitis that works by restoring the protective glycosaminoglycan layer in the bladder.14,15 Amitriptyline may also be used to treat interstitial cystitis-associated nocturia.
Myofascial pain: Neuromuscular blockers
According to a recent systematic review of therapies for chronic pelvic pain, patients with symptoms related to myofascial pain may benefit from neuromuscular blockade.12 One randomized controlled trial of the effectiveness of botulinum toxin A vs saline for the treatment of chronic pelvic pain secondary to pelvic floor spasm found that after 6 months of observation, women who received botulinum toxin had significantly lower pain scores than those who received saline.12
Pelvic congestion syndrome:
Multiple options Pelvic congestion syndrome may be treated with hormonal, radiologic, or surgical therapy.16 A randomized controlled trial involving patients with chronic pelvic pain secondary to pelvic congestion demonstrated that treatment with medroxyprogesterone acetate or a GnRH agonist (goserelin) improved pelvic symptoms.17
A Cochrane review of nonsurgical interventions for chronic pelvic pain included women with a diagnosis of pelvic congestion syndrome or adhesions. It found that patients treated with medroxyprogesterone acetate were more likely to have 50% pain reduction lasting up to 9 months compared with patients taking placebo.12 In comparative studies, GnRH analogues were more effective in relieving pelvic pain than progestogen therapy.
Radiologic embolization therapy is as effective as hysterectomy for the relief of chronic pelvic pain related to pelvic congestion syndrome, and it can be performed in the outpatient setting.
Irritable bowel syndrome: Try dietary changes
Symptoms of chronic pelvic pain that are associated with changes in stool consistency and frequency suggest irritable bowel syndrome. Symptoms may improve with dietary changes and fiber supplementation. Antispasmodic agents are frequently used but their anticholinergic effects may worsen constipation.14
PELVIC PHYSICAL THERAPY
Pelvic physical therapy targets the musculoskeletal components of bowel, bladder, and sexual function to restore strength, flexibility, balance, and coordination to the pelvic floor and surrounding lumbopelvic muscles. Pa tients with dyspareunia, pain with activity, or a significant musculoskeletal abnormality (eg, vaginismus or point tenderness on examination) are particularly good candidates for this therapy. It is done by a physical therapist with special training in techniques to manipulate the pelvic floor to address pelvic pain.
Educating the patient
Informing the patient before the initial physical therapy visit is essential for success. Referring clinicians should emphasize to patients that treatment response can help to guide further physician intervention. Patients should be counseled that pelvic physical therapy includes a pelvic examination and an expectation to participate in a home program. Although noticeable improvement takes time, encouragement provided by the entire team, including medical providers, can help a patient maintain her care plan.
Therapists typically see a patient once a week for 8 to 12 visits initially. Insurance usually covers pelvic physical therapy through the same policy as routine physical therapy.
During the initial evaluation, the patient receives an external and internal pelvic examination assessing muscle length, strength, and coordination of the back, hip, and internal pelvic floor. Internal evaluation can be done vaginally or rectally, with one gloved finger, without the need for speculum or stirrups. Biofeedback and surface electromyography (using either perianal or internal electrode placement) are used to evaluate muscle activity and to assist the patient in developing appropriate motor control during strengthening or relaxation.18
Up-training (or strengthening) aims to improve pelvic floor endurance. It can improve pelvic instability and symptoms of heaviness and discomfort from prolapse. Patients learn to appropriately utilize the pelvic floor in isolation. If a patient is too weak to contract on her own, neuromuscular electrical stimulation is used with an internal electrode to provide an assisted contraction.
Down-training (or relaxation) focuses on reducing tone in overactive pelvic muscles. It can improve symptoms of chronic pelvic pain, sexual pain, vulvodynia, and pudendal neuralgias. Patients are made aware of chron ic holding patterns that lead to excess tone in the pelvic floor and learn how to release them through stretching, cardiovascular activity, meditation, and manual release of the involved muscle groups internally and externally. Internal musculature can be manipulated by a therapist in clinic or by the patient’s trained partner; the patient can also reach necessary areas with a vaginal dilator.
Functional coordination of the pelvic floor is needed for comfortable vaginal penetration and defecation. Training with biofeedback improves a patient’s ability to relax and open the pelvic floor.18 Vaginal dilators with surface electromyography are used to treat vaginismus to eliminate reflexive pelvic floor spasm during penetration. Perineal and vaginal compliance can be improved through manual release techniques with hands or vaginal dilators to restore normal mobility of tissues. This can reduce pain from postsurgical changes, postpartum sequelae, atrophic vaginal changes, shortened muscles from chronic holding, and adhesions.
PSYCHOSOCIAL INTERVENTIONS
Pelvic pain is not only a biomedical difficulty; psychosocial factors can contribute to and be affected by pelvic pain. Patients with pelvic pain often experience lower quality of life, higher rates of anxiety and depression, and increased stress compared with others.19,20 People with pain also have more relationship stress, and patients’ partners often experience emotional distress, isolation, and feelings of powerlessness in the relationship.21
Psychosocial interventions, provided along with biomedical treatment, can help to reduce pain, anxiety, and depression and improve relational well-being.22,23 In addition to attending to pain-related symptoms, comprehensive care involves recognizing and treating coexisting anxiety, depression, stress, and relationship conflict. Interventions for these difficulties are many, and a comprehensive list of interventions is beyond the focus of this section.19
Cognitive behavioral therapy
Cognitive behavioral therapy is based on the idea that maladaptive cognitions can lead to problematic behaviors and emotional distress.24 Interventions are carried out by a provider with specialized training in its use (eg, therapist, pain psychologist, psychiatrist).
Meta-analyses of studies that investigated the efficacy of cognitive behavioral therapy for chronic pain found consistent small to medium improvement in pain-related symptoms.24 Studies that used cognitive behavioral therapy for pelvic pain found reduced overall pain severity and pain during intercourse, increased sexual satisfaction, enhanced sexual function, and less-exaggerated responses to pain.25–27
Although cognitive behavioral therapy and mindfulness-based interventions produce positive outcomes, research on these interventions typically includes treatment carried out over a span of weeks. Common barriers to such care include lack of patient motivation, financial limitations, transportation problems, and time constraints.
The following psychosocial interventions have been chosen because they can be delivered in a short amount of time and integrated into a patient’s medical care by a medical or behavioral health provider. Because of the brevity and simplicity of these interventions, more patients with pelvic pain can receive psychosocial care as part of their usual medical encounters.
Behavioral activation
People experiencing depressive symptoms tend to isolate themselves and stop participating in activities they enjoy, including spending time with family and friends. Behavioral activation interventions that address such isolating behaviors have been shown to be effective in improving depressive symptoms.28–30
A simple, brief intervention can be administered during routine medical care,28 involving the following steps:
Determine activities that the patient might implement that would decrease depressive symptoms. Questions such as, “When do you feel less depressed?” or “What brings you some happiness in your life?” can generate possible activities.
Ask the patient to identify people in her life who have been supportive and with whom she could engage.
Create with the patient a list of possible activities and social interactions that may enhance well-being.
Make a schedule for participating in activities, possibly with rewards for completing them. Patients should be encouraged to follow the prescribed schedule of activities rather than make decisions based on mood or other factors.
Relaxation strategies
Relaxation can help patients reduce stress and anxiety, and can also help reduce pain.31–33
Diaphragmatic or “belly breathing” is a deep-breathing technique in which participants are asked to take in air through the nose and fully fill the lungs and lower belly. This technique allows the body to take in more oxygen, helping to lower blood pressure and slow the heartbeat. In addition to physiologic benefits, concentrating on deep breathing can help slow down or stop intrusive thoughts and distressing physical sensations.34
Progressive muscle relaxation involves the systematic tensing and relaxing of each large muscle group in the body.35 The goal is to eliminate physical and emotional stress through focusing on the sensations of tension and relaxation.
Scripts and audio and video resources for belly breathing and progressive muscle relaxation can be found on the Internet. The techniques can be taught during the medical appointment or offered as resources for home practice.
Couple-based care
Targeting couples is more effective for improving well-being than focusing solely on a patient’s psychosocial difficulties, so each of the above interventions may be more effective if tailored to include the patient’s partner.36 If the partner is with the patient during medical visits or is included in long-term psychosocial treatment, he or she can be directly involved in learning and practicing interventions with the patient. If the partner is not present, the patient can be asked to practice newly learned well-being-enhancing strategies with her partner outside the appointment time. Couples therapy can improve psychosocial well-being for both partners.
Setting goals
For all interventions, setting goals is important. Using collaborative goal-setting, patients and providers together should develop goals that specifically attend to reducing pain-related difficulties and comorbid anxiety, stress, and depression.22 For example, if a patient has found that belly breathing helps reduce anxiety, a goal may be for the patient to practice belly breathing with her partner 3 times per week for 10 minutes, until her next medical appointment in 1 month. After the patient and provider have codeveloped goals for improving psychosocial well-being, provider and patient can discuss progress made toward goals during each subsequent visit. Depending on progress, providers can highlight patient success and modify goals as needed. Table 3 provides an example outline of collaborative goal-setting.
Collaborative goal-setting
- Copyright © 2018 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.