


Article Figures & Data
Figures
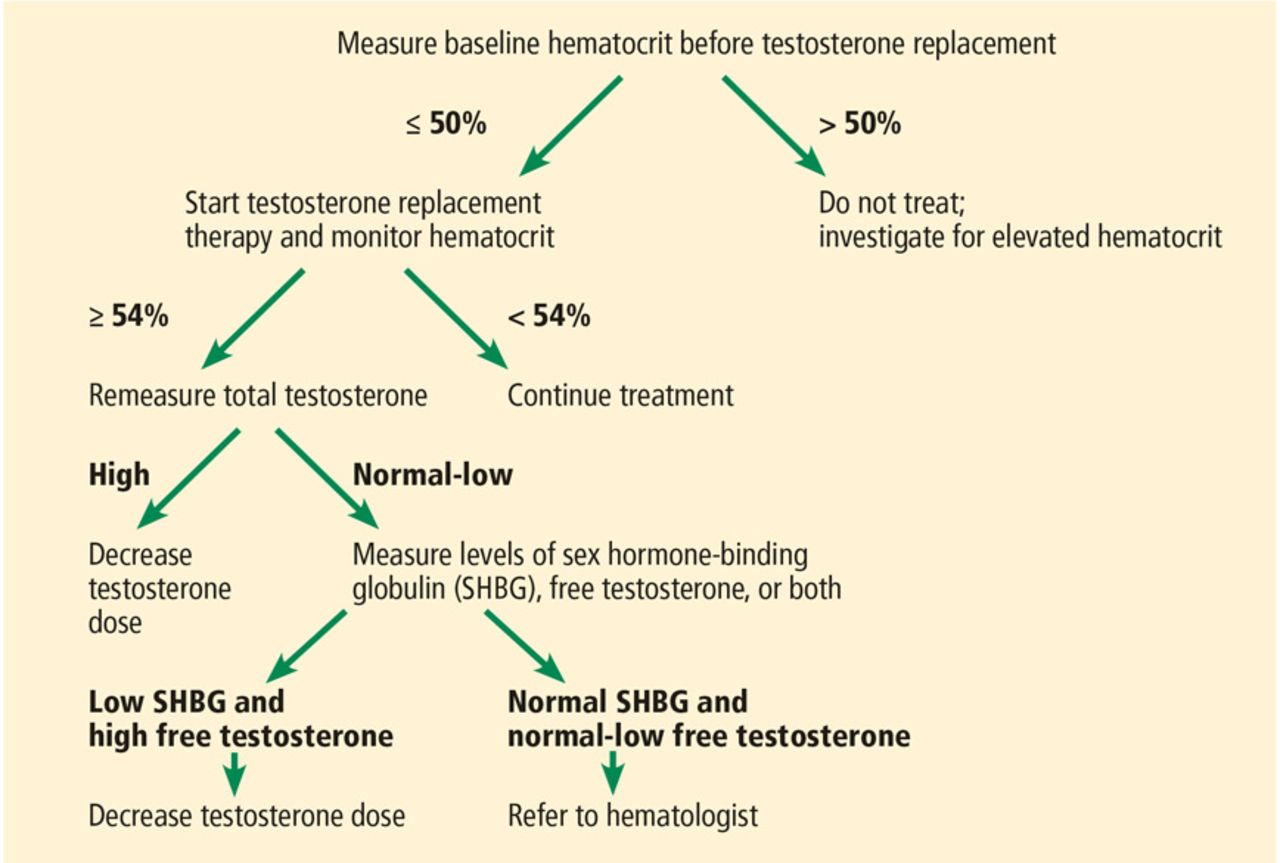
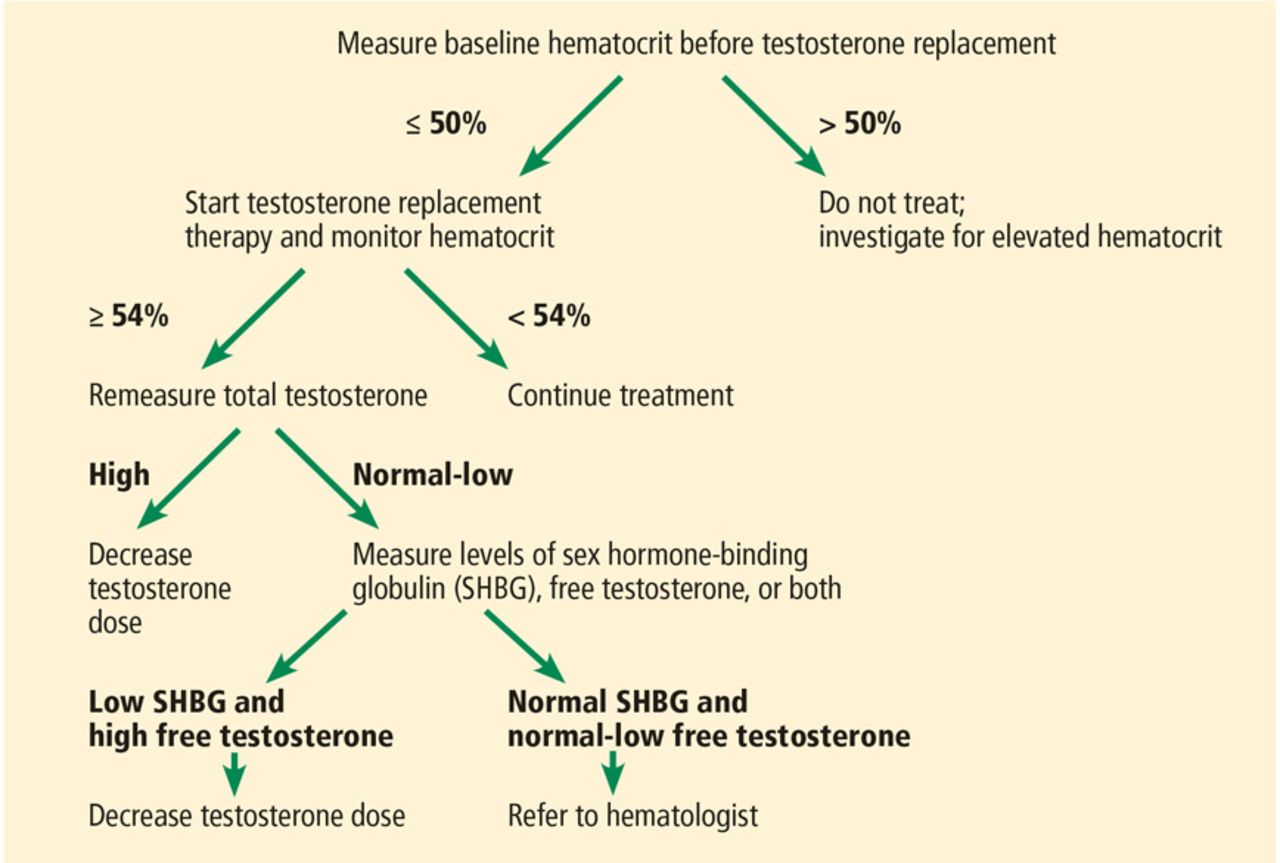
- FIGURE 1
Hematocrit monitoring for patients on testosterone replacement therapy.
Tables
Test Valuea Reference range Complete blood cell count Hemoglobin 14.5 g/dL 13–17 g/dL Hematocrit 44% 40%–54% Mean corpuscular volume 93 fL 80–100 fL Mean corpuscular hemoglobin 31 pg/cell 26–34 pg/cell Mean corpuscular hemoglobin concentration 33 g/dL 31–36 g/dL Red blood cell distribution width 13.5% 11.5%–14.5% White blood cell count 8.3 × 109/L 4.5–11.0 × 109/L Neutrophils 63% 40%–75% Lymphocytes 28% 20%–45% Monocytes 7% 2%–10% Eosinophils 2% 1%–6% Basophils 0% 0%–1% Platelet count 310 × 109/L 150–400 × 109/L Metabolic panel Serum creatinine 0.8 mg/dL 0.5–1.1 mg/dL Blood urea nitrogen 14 mg/dL 7–20 mg/dL Serum sodium 138 mmol/L 135–145 mmol/L Serum potassium 4.6 mmol/L 3.5–5.3 mmol/L Serum chloride 97 mmol/L 95–105 mmol/L Serum bicarbonate 23.6 mmol/L 22–26 mmol/L Alanine aminotransferase 37 IU/L 7–52 IU/L Aspartate aminotransferase 32 IU/L 10–40 IU/L Serum albumin 4.7 g/dL 3.5–5.5 g/dL Thyroid-stimulating hormone 2.3 mIU/L 0.5–5 mIU/L Fasting blood glucose 92 mg/dL < 100 mg/dL Morning total testosterone 120 ng/dL 270–1,000 ng/dL Erythrocyte sedimentation rate 13 mm/h 0–22 mm/h ↵a Abnormal results are shown in bold.
General and cognitive manifestations Fatigue, lack of energy Poor motivation Impaired concentration and memory Depressed mood Irritability Sleep disturbance Reproductive manifestations Decreased libido Decreased morning erections Erectile dysfunction Decreased shaving frequency Decreased body hair Gynecomastia Decreased size of testes Infertility (decreased sperm production) Other manifestations Decreased bone mineral density, osteoporosis, fractures Loss of muscle mass and strength Increased body fat and body mass index Hot flashes (with severe testosterone deficiency) Condition Comments Obesity Can cause central hypogonadism and is a predictor for testosterone replacement therapy Type 2 diabetes mellitus An independent association with male hypogonadism has been reported
One-third of men with type 2 diabetes mellitus have low testosterone in cross-sectional studiesMetabolic syndrome An association with low serum testosterone has been reported Unexplained anemia Moderate to severe testosterone deficiency is associated with lower hemoglobin Low bone mineral density The relationship between low testosterone and low bone mineral density is not definite, yet guidelines recommend measuring serum testosterone in men with osteoporosis or low-trauma fracture Chronic obstructive pulmonary disease 22%–69% of men with chronic obstructive pulmonary disease have been reported to have hypogonadism
Testosterone replacement may benefit patients in terms of exercise capacityHuman immunodeficiency virus (HIV) infection Cohort studies showed that 17%–38% of men who are HIV-positive have low testosterone
Testosterone replacement in men with HIV-associated weight loss can improve body weight, muscle mass, and moodInfertility Pituitary and testicular causes of infertility may also cause hypogonadism Hypothalamic and pituitary disorders Can cause central hypogonadism History of testicular radiation Direct or scatter radiation may damage Leydig cells leading to primary hypogonadism History of chemotherapy Chemotherapy may be a risk factor for low testosterone Opioid use Chronic opioid use can lead to testosterone deficiency in up to 50% of men
Hypogonadism in a young man should alert physicians to possible opioid abuseChronic glucocorticoid use A risk factor for low testosterone levels History of androgenic anabolic steroid use Chronic use can suppress hypothalamic-pituitary-testicular axis, causing hypogonadism upon withdrawal Local (pituitary and hypothalamus) Congenital Kallmann syndrome Prader-Willi syndrome Idiopathic panhypopituitarism Mutations in luteinizing hormone or follicle-stimulating hormone subunits Acquired Pituitary masses and tumors Pituitary destruction (surgery, radiation) Pituitary apoplexy Head trauma Meningitis (especially tuberculosis) Infiltrative diseases (eg, hemochromatosis) Idiopathic Systemic Metabolic Hyperprolactinemia Obesity Malnutrition Eating disorders (eg, anorexia nervosa) Excessive exercise Drug- or substance-related Glucocorticoids, opioids, estrogens, and progestins Androgen withdrawal Alcohol and marijuana abuse Others Acute critical illness (eg, myocardial infarction, surgery) Chronic systemic disease (eg, cirrhosis, organ failure, acquired immunodeficiency syndrome) Proven Virilization and maintenance of secondary sexual characteristics Improved sexual function: increased libido, better erectile function Increased muscles mass and strength Decreased fat mass Increased bone mineral density Not proven (conflicting or no evidence) Improved energy Improved cognitive function Improved mood Improved depressive symptoms - TABLE 6
Prostate monitoring for patients on testosterone replacement therapy, according to age
Age (years) Endocrine Society Guidelines5 < 40 No need for prostate monitoring 40–54 Baseline prostate-specific antigen and digital rectal examination if high risk,a repeat at 3 to 12 months after starting testosterone replacement therapy, then continue according to screening guidelines 55–69 Baseline prostate-specific antigen and digital rectal examination, repeat at 3 to 12 months after starting testosterone replacement therapy, then continue according to screening guidelines ≥ 70 No need for prostate monitoring ↵a High-risk patients include African Americans and patients with a first-degree relative with confirmed prostate cancer.




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.