


Article Figures & Data
Figures
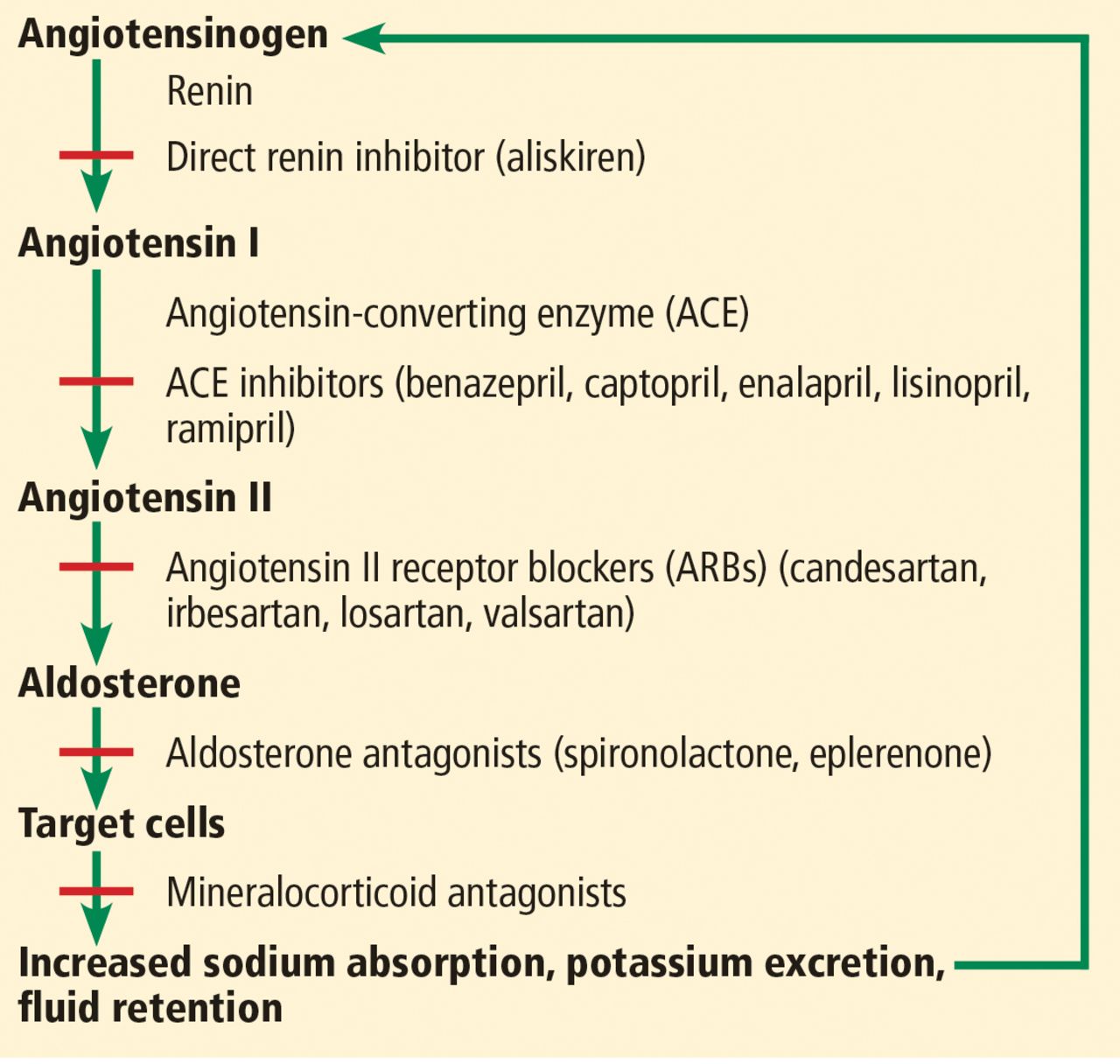
- Figure 1
The renin-angiotensin-aldosterone system and drugs that inhibit it.

Tables
Before starting or changing the dose Review medications Check baseline blood values of potassium, bicarbonate, and creatinine; assess proteinuria Ensure patient is volume-replete Do not start or increase the dose of a renin-angiotensin-aldosterone system inhibitor if serum potassium is elevated Use an ACE inhibitor or ARB cautiously; start with a low dose and titrate upward slowly every 2 weeks if creatinine rises < 30% from baseline and GFR drops < 25% Reduce dose if maximal doses are not tolerated (see below) Repeat blood testing 10–14 days after starting or changing the dose Check potassium and renal function after each dose escalation If serum potassium is persistently > 5.0 mmol/L Give dietary advice Review medications again Consider a thiazide or loop diuretic to reduce potassium level Consider adding sodium bicarbonate if serum bicarbonate level is < 22 mmol/L Remeasure potassium after 10–14 days If > 5.0 mmol/L, continue If 5.0–5.5 mmol/L, reduce dose and monitor closely if >5.5 mmol/L, consider stopping If renal function declines, ie, if creatinine rises > 30% from baseline or GFR drops > 25% after starting an ACE inhibitor or ARB: Investigate for any other underlying cause, eg, bilateral renal artery stenosis Repeat blood tests after 10–14 days If no improvement, reduce dose by 50% If still no improvement, reduce the dose further or stop the drug For patients with illness or dehydration Temporarily stop the ACE inhibitor or ARB, diuretics, and other antihypertensive and nephrotoxic drugs Avoid medications that may impair renal function Restart once symptoms resolve and the patient is rehydrated and biochemically stable Recheck renal function after starting to ensure it remains stable Ongoing monitoring Continue to monitor once patient is established and stabilized on treatment with an ACE inhibitor or ARB according to the stage of their chronic kidney disease and heart failure, their medication history, and clinical condition. Monitoring every 3–6 months, as well as when patients have an intercurrent illness, is usually adequate. ACE = angiotensin-converting enzyme, ARB = angiotensin II receptor blocker




{kind=link}
Jump to section
Related Articles
Cited By...
- The Effects of Medication Strategies on Cardiovascular Outcomes in Patients with Marfan Syndrome: A Consistency Model Analysis
- In reply: Is diabetes still a compelling indication for renin-angiotensin-aldosterone system inhibitors?
- Is diabetes still a compelling indication for renin-angiotensin-aldosterone system inhibitors?
- ACE inhibitor and ARB therapy: Practical recommendations