


ABSTRACT
Pregnancy can exacerbate known cardiovascular disorders and unmask previously unrecognized problems. Patients with congenital heart disorders, valvular disease, primary pulmonary hypertension, hypertensive disorders of pregnancy, and acquired peripartum cardiomyopathy need a collaborative interdisciplinary team that includes a cardiologist with specialty training in obstetrics.
Several trends are increasing cardiovascular risk in pregnancy. The average maternal age at first pregnancy is increasing, survival in congenital heart disease has improved, and cardiovascular risk factors are developing at younger ages.
Maternal morbidity and mortality are increasing, with cardiovascular diseases accounting for over one-quarter of peripartum and postpartum deaths.
Rates of maternal mortality from cardiovascular disease are highest among low-income women and women of color.
The emergence of new cardiovascular complications during pregnancy is often considered a failed stress test and can increase the risk of future cardiovascular disease. Women should be monitored closely after pregnancy in order to improve maternal outcomes and prevent the development of future cardiovascular disease.
Cardiovascular complications during and after pregnancy are on the rise, but traditional cardiology and obstetric training programs do not adequately cover this topic. As a result, many family clinicians, obstetricians, and cardiologists are uncomfortable managing pregnant women with cardiovascular conditions.
In this review, we describe populations of women at risk for heart disease in pregnancy and discuss the most commonly encountered preexisting and incident types, with a focus on recognition, risk assessment, and management.
MATERNAL MORTALITY RATES RISING
In the United States, between the years 2000 and 2014, the maternal death rate increased by 6.6%.1 In the years 1998–2005, the rate of death during or within 1 year of pregnancy attributed to cardiovascular causes was 3.48 per 100,000 live births2; in 2006–2010 it was 4.23.3,4 A study in Hawaii from 1991 to 2007 found that 4.2% of all deaths occurred within 1 year of pregnancy, and heart disease was the leading cause of pregnancy-associated death (20.5%). The most prominent causes of maternal death were peripartum cardiomyopathy, myocardial infarction, and arrhythmias.5 Similar findings were reported in a 2002–2006 review in California.6
Ethnic and racial disparities in maternal outcomes exist in the United States: eg, in black women, the risk of pregnancy-related death is 3 times higher than in women of oth er races.3 This may partially be due to higher rates of preexisting cardiovascular disease and higher rates of new-onset hypertension of pregnancy and peripartum cardiomyopathy.7,8 Disparities may also result from poorer quality of care and provider bias.9,10
REASONS FOR THE INCREASE IN CARDIOVASCULAR RISK
Three major trends are contributing to the increase in maternal cardiovascular risk.
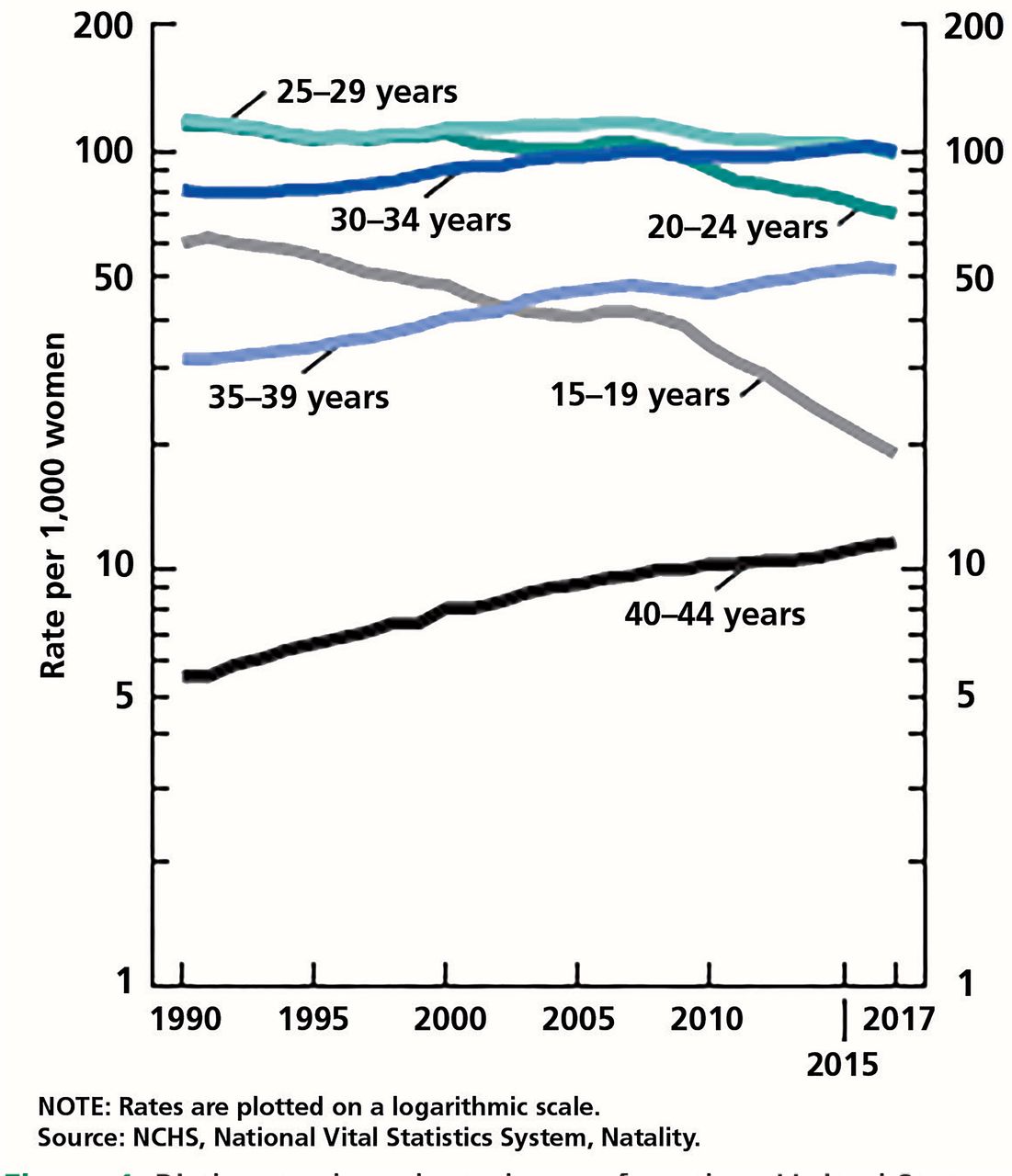
Older women are having children
Women are waiting longer to have children (Figure 1).11,12 Between 2000 and 2015, pregnancy rates increased from 40 to 52.3 per 1,000 in women ages 35 to 39 and from 8 to 11.6 per 1,000 in women ages 40 to 45.13,14 The average age of first-time mothers in the United States rose from 24.9 in 2000 to 26.8 in 2017.12,14 This trend is not limited to the United States—the mean age for first preg nancies is increasing around the world.15

Reasons for delaying pregnancy likely include increased availability and efficacy of contraception, more women pursuing higher education and careers, and economic uncertainty among younger women.16
More children with congenital heart disease now survive into adulthood
Thanks to advances in surgery and medical care, most children with congenital heart disease now survive to childbearing age.17
An estimated 1% of women giving birth in the United States have congenital heart disease.18 Between 2000 and 2010, the prevalence of maternal congenital heart disease increased from 6.4 to 9.0 per 10,000 hospitalizations for childbirth.19
Congenital heart diseases in adults range in severity from simple abnormalities such as atrial septal defects (17%) and ventricular septal defects (14%) to moderate ones such as repaired tetralogy of Fallot (11%) and more severe disease such as transposition of the great arteries (5%) and Ebstein anomaly (2%).20
Cardiovascular risk factors are increasing in young people
Rates of obesity, diabetes, hypertension, and atherosclerosis are increasing in the United States in younger adults,21 including women of childbearing age, placing them at risk of pregnancy complications.
PREGNANCY INCREASES CARDIOVASCULAR RISK
Hemodynamic and hormonal factors in pregnancy contribute to cardiac risk and exacerbate preexisting conditions.
Increased cardiac output
During pregnancy, plasma volume expands, leading to increased stroke volume, which may increase cardiac output by 30% to 50%.22 Cardiac output is further increased during labor—by 15% in the first stage, and by up to 50% in the second stage, due to pain, anxiety, and “autotransfusion” of blood into the circulation during uterine contractions, increasing the circulating volume by 300 to 500 mL (Table 1).23 Cardiac output also increases by 25% to 40% after delivery in addition to the increases during pregnancy and delivery, due to reduced vena cava compression and to uterine contractions, and then declines rapidly over the next hours.24
Physiologic changes of pregnancy
Other hemodynamic changes of pregnancy include increased heart rate, reduced systemic vascular resistance, and complex changes in systolic blood pressure, all of which contribute to a rise in cardiac output.25
Physiologic anemia
In conjunction with increased cardiac output, blood volume increases by about 1.5 L during pregnancy. Although red blood cell mass also increases, the increase is not proportionate to the plasma volume, resulting in physiologic anemia.26
Hormonal changes
Estrogen and progesterone levels rise during pregnancy, which increases sympathetic tone and can increase the risk for plaque rupture and thrombosis.27
CONGENITAL HEART DISEASE AND PREGNANCY
Congenital heart disease accounts for about 75% of cases of heart disease in pregnancy,28 and this percentage is increasing.
While some congenital heart problems (eg, atrial septal defect, patent ductus arteriosus) may be well tolerated during pregnancy, complex syndromes such as pulmonary hypertension from Eisenmenger physiology are associated with a risk of maternal death as high as 50%.29
Metabolic and physiologic changes of pregnancy may precipitate new heart failure or exacerbate existing cardiac disease, especially in women who underwent repair of congenital heart lesions as children. Even if the defect has been repaired, a patient can still be vulnerable to later complications such as heart failure, arrhythmia, pulmonary hypertension, and residual structural concerns.
Congenital heart disease also increases the risk of medical and obstetric complications during delivery.19
Management guidelines available
The 2008 American College of Cardiology and American Heart Association guidelines for managing adults with congenital heart disease include topics in pregnancy such as frequency of follow-up, stress testing, anticoagulation, anesthesia, monitoring during delivery, pregnancy counseling, genetic evaluation, review of medications, and fetal echocardiography.30 The following are a few highlights:
General risk. In general, if a patient’s functional class and systolic function are normal or near-normal, pregnancy tends to be uncomplicated. Nonetheless, all women with congenital heart disease who are considering pregnancy should be seen by an adult congenital heart disease specialist before conceiving.
Anticoagulation. The risks and benefits of continuing anticoagulation during pregnancy should be discussed with the patient. Warfarin is teratogenic and should be avoided during the first trimester. Warfarin should also be avoided during delivery, given the increased risk of fetal intracranial hemorrhage; low molecular weight heparin and unfractionated heparin should be used instead. The efficacy and safety of the direct-acting oral anticoagulants in pregnancy are still unknown, as data are scarce.31
Delivery method. In general, vaginal delivery is preferable for women with congenital heart disease unless cesarean delivery is indicated for obstetric reasons.
Breastfeeding is considered safe in patients with heart disease, although many cardiac medications may cross into breast milk. These issues should be discussed with the patient before restarting medications after delivery.
PREEXISTING ACQUIRED HEART DISEASE IN PREGNANCY
The prevalence of preexisting acquired heart disease (eg, valvular heart disease, pulmonary hypertension, arrhythmia) in pregnancy is difficult to ascertain, given that pregnancy can unmask previously unknown disease. A nationwide 2003–2012 study found 81,295 women with heart disease, representing 0.2% of all pregnant women in the sample. Of these women, 30.9% had valvular heart disease and 6.5% had pulmonary hypertension, both of which require specific management during pregnancy.32
Acquired valvular disease
Acquired valvular disease can lead to complications during pregnancy owing to hemodynamic changes. In some situations, valvular disease is first diagnosed during pregnancy, when hemodynamic changes may cause heart failure and arrhythmias.
Women with a stenotic valve can safely undergo balloon dilation by percutaneous catheter; cardiac surgery should be considered only in severe cases.33
Primary pulmonary hypertension
Primary pulmonary hypertension can cause right heart failure. Women with severe pulmonary hypertension have the highest maternal death rate, approaching 50%, which is attributed to high fixed pulmonary vascular resistance and an inability to increase pulmonary blood flow.34 Given the high risk, most providers and guidelines recommend against pregnancy for women with established pulmonary hypertension.
Pregnancy management. A woman who decides to continue her pregnancy should be followed closely with at least monthly visits. Given the dearth of data, it is unknown if patients with lower pulmonary pressures have a lower risk of complications; even some women with mild to moderate pulmonary hypertension deteriorate during pregnancy. Efforts should be made to reduce oxygen demand with rest and to use supplemental oxygen when indicated. Frequently, patients with severe pulmonary hypertension are admitted to the hospital in the second trimester and followed as inpatients.
It is often recommended that women continue their pulmonary hypertension medications during pregnancy, except for bosentan, a dual endothelin receptor antagonist with teratogenic effects. Other advanced therapies such as prostacyclin analogues and sildenafil are considered safe.35
Delivery. The preferred delivery method in patients with pulmonary hypertension is highly debated. Vaginal delivery increases cardiac output, and pushing during the second stage of labor can reduce venous return to the right side of the heart, both of which may be particularly dangerous for these patients. Additionally, because patients with pulmonary hypertension tend to go into labor early, induction of labor may be associated with increased length of labor and a likelier need for an emergency cesarean delivery, which entails additional risks.
For these reasons, many institutions (including ours) recommend elective cesarean delivery to avoid emergency procedures and minimize blood loss. General anesthesia is not recommended because of reports of cardiac failure owing to adverse effects of intubation and positive pressure ventilation on venous return. Instead, regional anesthesia with a combination of epidural and low-dose spinal anesthesia is preferred to avoid vasodilation and the associated risk of hypotension. During delivery, it is imperative to closely follow arterial and venous hemodynamics including blood pressure; in addition, the mother should be observed in the hospital after delivery for several days until stable.36–38
Preexisting hypertension
A physiologic drop in blood pressure in pregnancy may allow women with preexisting hypertension to avoid medication use early in pregnancy, although they should be monitored closely. Those who require ongoing medication should switch to a drug deemed safer for pregnancy such as labetalol, metoprolol, or a calcium channel blocker; labetalol and nifedipine are most commonly used. Angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, and direct renin inhibitors are contraindicated in pregnancy.
Hypertensive patients of African or Caribbean family origin should be treated with a calcium channel blocker as a first-line agent39 and should be carefully monitored for progression to preeclampsia or eclampsia.40
INCIDENT CARDIOVASCULAR DISEASE IN PREGNANCY
Cardiovascular disease can arise during pregnancy in women without preexisting conditions.
Hypertensive disorders of pregnancy
New-onset hypertension and maternal placental disorders such as preeclampsia occur in 1% to 5% of pregnancies. They are defined as blood pressure higher than 140/90 mm Hg arising after 20 weeks of gestation.
Risk factors for hypertensive disorders of pregnancy include genetics41,42 and, for preeclampsia, elevated body mass index (> 24 kg/m2).43
Future risk. Developing a hypertensive disorder of pregnancy has been compared to failing a stress test, in that it often presages later cardiovascular disease.44 Underlying or unrecognized risk factors may contribute not only to the development of hypertensive conditions in pregnancy, but also to subsequent cardiovascular disease.
Hypertensive disorders in pregnancy have been shown in numerous studies to increase the risks for metabolic syndrome, subsequent diagnosis of hypertension, and lifetime risk of cardiovascular disease.45–48 Problems may reveal themselves soon after giving birth: a study of all births in New York City from 1995 to 2004 found that women with gestational hypertension had a higher rate of hospitalizations in the year after delivery related to heart failure (adjusted odds ratio 2.6), and women with preeclampsia had higher rates of hospitalization for cardiovascular disease and stroke.49
The American Heart Association considers preeclampsia to be a cardiac risk factor and recommends monitoring women with preeclampsia for the first few years after delivery.50,51 Women with this condition have at least double the risk of stroke, cardiac ischemia, or venous thromboembolism for up to 20 years after pregnancy.
Peripartum cardiomyopathy
Peripartum cardiomyopathy occurs in about 1 in 1,000 to 4,000 live-birth pregnancies. Proposed causes include autoimmunity, genetics, nutritional deficiencies, and vascular dysfunction.52 Advanced maternal age, preeclampsia, gestational hypertension, multiparity, and African American race have been identified as risk factors.
Presentation. Peripartum cardiomyopathy classically presents during the first 6 months after delivery, but it may also present during the second or third trimester of pregnancy. The typical presentation is consistent with that of heart failure (eg, orthopnea, paroxysmal nocturnal dyspnea, significant peripheral edema, elevated jugular venous distention). This is often difficult to distinguish from signs and symptoms of normal pregnancy, especially during the third trimester, so a high index of suspicion is required.
Diagnosis. Other possible causes of heart failure (ie, ischemic, congenital) should first be ruled out. Echocardiography is required for evaluation.52
Pregnancy management. Patients are managed similarly to pregnant women with other forms of heart failure in pregnancy: beta-blockers and volume control agents, including diuretics, to reduce afterload are the mainstays of therapy.
Postpartum care. After delivery, patients should be managed with standard therapy consisting of beta-blockers, angiotensin-converting enzyme inhibitors, mineralocorticoid receptor antagonists, and diuretics. Patients with severe hemodynamic compromise and depressed left ventricular function may require inotropic support or mechanical circulatory devices.53
Prognosis. Most women recover from peripartum cardiomyopathy. The Investigations of Pregnancy-associated Cardiomyopathy study found that after 12 months, left ventricular ejection fraction had increased to greater than 50% in more than two-thirds of women. However, 13% had major events or persistent heart failure (ejection fraction < 35%).54 Even with full left ventricular recovery, there is a risk of recurrence with subsequent pregnancies, and this risk is higher in women with persistent left ventricular dysfunction. There are currently no firm recommendations to guide women on subsequent pregnancies,55 but they should be advised of the risks.52
Ischemic heart disease
New ischemic heart disease of pregnancy, which includes plaque rupture and thrombosis, spontaneous coronary artery dissection, coronary embolism, and vasospasm, is estimated to occur in 1 to 6.2 per 100,000 deliveries,56 a rate 3 to 4 times higher than in nonpregnant women of comparable age.57 The most common causes of new ischemic heart disease are coronary artery dissection and coronary artery thrombosis.
Spontaneous coronary artery dissection. Pregnancy-related spontaneous coronary artery dissection occurs by intimal rupture causing medial dissection, or by a spontaneous disruption of the vasa vasorum, which causes intra-medial hemorrhage and separation within the arterial wall. Proposed underlying causes include hormonally mediated structural changes of decreased collagen synthesis and increased polysaccharide content, which weakens the tunica media, predisposing it to dissection; underlying connective tissue disorders such as Marfan syndrome or Ehlers-Danlos syndrome; and inflammatory conditions such as lupus erythematosus. Such factors, when combined with the increased hemodynamic effects of pregnancy and labor, are thought to precipitate spontaneous artery dissection.58
Risk factors for ischemic heart disease during pregnancy are similar to those outside of pregnancy, ie, smoking, diabetes, family history, hyperlipidemia, and chronic hypertension. While rare, women with preexisting but undiagnosed coronary atherosclerosis have the greatest risk of myocardial ischemia during pregnancy,59 followed by those with pregnancy after age 40.60 Patients with congenital heart disease (eg, uncorrected anomalous origins of the coronary arteries) or severe aortic stenosis or those who have undergone previous surgical coronary manipulation are also at increased risk for ischemia.61
Pregnancy management. The goal of managing ischemic heart disease during pregnancy is to reduce oxygen demand to avoid progression to infarction. In the absence of ST-segment elevation acute coronary syndrome, patients can be managed with watchful waiting and medical therapy with beta-blockade and low-dose aspirin.
Infarction management. Should myocardial infarction occur, percutaneous coronary intervention is advised, given the risk of hemorrhage with thrombolysis. After percutaneous coronary intervention, routine management with dual antiplatelet inhibitors and beta-blockers is generally well tolerated. Angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers are contraindicated due to embryonic toxicity.
Delivery. Vaginal delivery is preferred over cesarean delivery to avoid the hemodynamic changes of anesthesia and the potential for blood loss. Epidural analgesia is advised for pain control, given its effects on reducing afterload, pain, stress, and anxiety.
RISK ASSESSMENT
Several tools have been developed to estimate morbidity and mortality risk in pregnant women with cardiac disease.
The Cardiac Disease in Pregnancy Study (CARPREG) risk score, developed in 1997, has been validated in several retrospective studies and is widely used. Applicable to pregnant women with acquired or congenital heart disease, the score stratifies risk according to the presence of poor functional class (New York Heart Association class III or IV), cyanosis, arrhythmias, prior cardiovascular events (heart failure, transient ischemic attack, stroke), left heart obstruction, and ejection fraction less than 40%.19
The CARPREG II study refined the initial score in 2018 by incorporating general characteristics with lesion-specific risk estimates (such as systemic right ventricle or peripartum cardiomyopathy with residual left ventricular dysfunction) to improve predictive accuracy (Table 2).62
The Cardiac Disease in Pregnancy (CARPREG II) modified risk score
The Pregnancy in Women With a Congenital Heart Defect (ZAHARA) risk score was developed in 2010 based on data from a retrospective study of 1,300 pregnancies (Table 3).63 It differs from the original CARPREG score by incorporating more specific details of prepregnancy cardiac disease, including valvular heart disease, and cardiac medications.
The Pregnancy in Women With a Congenital Heart Defect (ZAHARA) risk score
The World Health Organization (WHO) risk classification (Table 4), devised by the Task Force on the Management of Cardiovascular Diseases During Pregnancy of the European Society of Cardiology,40 the Working Group on Pregnancy and Contraception, and others, integrates congenital and acquired heart disease data with other comorbidities. It may better reflect the diversity of at-risk pregnant women and thus be more useful. One especially useful feature of the WHO score is that it has a 100% negative predictive value of cardiovascular events for class I patients (ie, uncomplicated or mild defect, repaired simple lesions, isolated premature ventricular beats and atrial ectopic beats), indicating that risk of pregnancy for that group is considered equivalent to that of the general population.
World Health Organization classes of pregnancy risk
Based on studies comparing the 3 scores, the WHO’s appears to best estimate the risk of cardiovascular events in pregnant women with preexisting heart disease. However, studies were performed using the first CARPREG model, so it is unclear how the CARPREG II model compares.64,65
SUBSEQUENT PREGNANCIES
Many women with cardiovascular complications in pregnancy, regardless of severity, desire additional pregnancies. The provider should engage the patient in shared decision-making with the goal of making as informed a decision as possible. Predicting outcomes for subsequent pregnancies can be challenging, and other than for preeclampsia and peripartum cardiomyopathy, few data exist regarding recurrent pregnancies in the setting of cardiac disease. With no firm guidelines or recommendations, guidance must rely heavily on a patient’s diagnosis and previous experience.
Women with structural or congenital heart disease that has remained stable can be managed similarly through subsequent pregnancies.
Preeclampsia. Published rates of recurrent preeclampsia range widely, from 5% to nearly 50%. Blood pressure and proteinuria should be monitored during subsequent pregnancy for early detection and consideration of aspirin use.48,51
Peripartum cardiomyopathy. Risk of relapse may be as high as 20% to 50% and is highest in patients with persistent left ventricular dysfunction from prior pregnancies. To reduce the risk of additional complications, women should be advised to wait until their left ventricular function has completely recovered before attempting pregnancy again.55
IMPROVING MATERNAL OUTCOMES
Cardiologists with expertise in managing cardiovascular disease in pregnancy are increasingly needed, as are multidisciplinary teams that can facilitate care for complex patients.
Lacking specific guidelines for pregnant women with a cardiovascular disorder, clinical practice varies, and knowledge is limited regarding best practices for detection and management. More research and opportunities for shared learning are needed, including establishing registries of pregnant women at risk of heart disease or with a known condition. Clinical trials of effective management approaches should be done.
Academic institutions should promote learning opportunities (eg, conferences, didactics, or specialized cross-disciplinary training). Our program at Yale has a monthly management conference attended by specialists in maternal fetal medicine, adult congenital heart disease, and cardiology.
The American College of Cardiology and American Heart Association recommend that patients with congenital heart disease be closely followed by a specialized team of providers, including specialists in adult congenital heart disease and maternal-fetal medicine, to assist in managing their pregnancies.30 Hospitals should organize and support collaborative multidisciplinary pregnancy care teams that include clinicians from the fields of family medicine, pediatrics, obstetrics, cardiology, endocrinology, and emergency medicine to facilitate care of complex patients.
In view of racial disparities in rates of maternal death, with especially high rates in black women, focused efforts are needed that engage health systems, providers, and communities to understand breakdowns in care.
Finally, better care systems need to be developed to focus on maternal health after delivery. Typically, medical attention tends to pivot toward the baby, resulting in missed opportunities for education, surveillance, and possible intervention for women at risk.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
Jump to section
- Article
- ABSTRACT
- MATERNAL MORTALITY RATES RISING
- REASONS FOR THE INCREASE IN CARDIOVASCULAR RISK
- PREGNANCY INCREASES CARDIOVASCULAR RISK
- CONGENITAL HEART DISEASE AND PREGNANCY
- PREEXISTING ACQUIRED HEART DISEASE IN PREGNANCY
- INCIDENT CARDIOVASCULAR DISEASE IN PREGNANCY
- RISK ASSESSMENT
- SUBSEQUENT PREGNANCIES
- IMPROVING MATERNAL OUTCOMES
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.