


A 59-year-old man presented to the emergency department with dizziness and fatigue. He had a history of alcoholic liver disease with cirrhosis, diagnosed 1 month prior, with small esophageal varices and a Model for End-Stage Liver Disease–Sodium score of 33 (indicating a high predicted mortality risk, 66% at 90 days). There was no hematemesis or melena.
Physical examination revealed scleral icterus, mild abdominal distention, and bilateral pitting edema, with scattered bruising.
Laboratory testing revealed the following:
Acute anemia, with a hemoglobin level of 6.3 g/dL, down from 10.6 g/dL 2 weeks earlier (reference range 13.0–17.0)
Macrocytosis, with a mean corpuscular volume of 109 fL, up from 92 fL (80–100)
Red blood cell distribution width 22% (11%–16%)
Reticulocyte count 9% (0.4%–2.0%), absolute count 194 × 109/L (18–100)
Lactate dehydrogenase 412 U/L (140–280). Stable thrombocytopenia and hyperbilirubinemia were also noted. Tests for human immunodeficiency virus and hepatitis were negative.
Computed tomography showed only diffuse edema and mild ascites, without hemorrhage or fluid collections.
The patient received a transfusion of 2 units of packed red blood cells, after which his hemoglobin level was even lower—5.9 g/dL. An additional 4 units were transfused over the next 48 hours, but his peak hemoglobin level was still only 6.5 g/dL.
Further testing showed rising bilirubin, an undetectable haptoglobin, elevated lactate dehydrogenase, and a negative direct Coombs test.
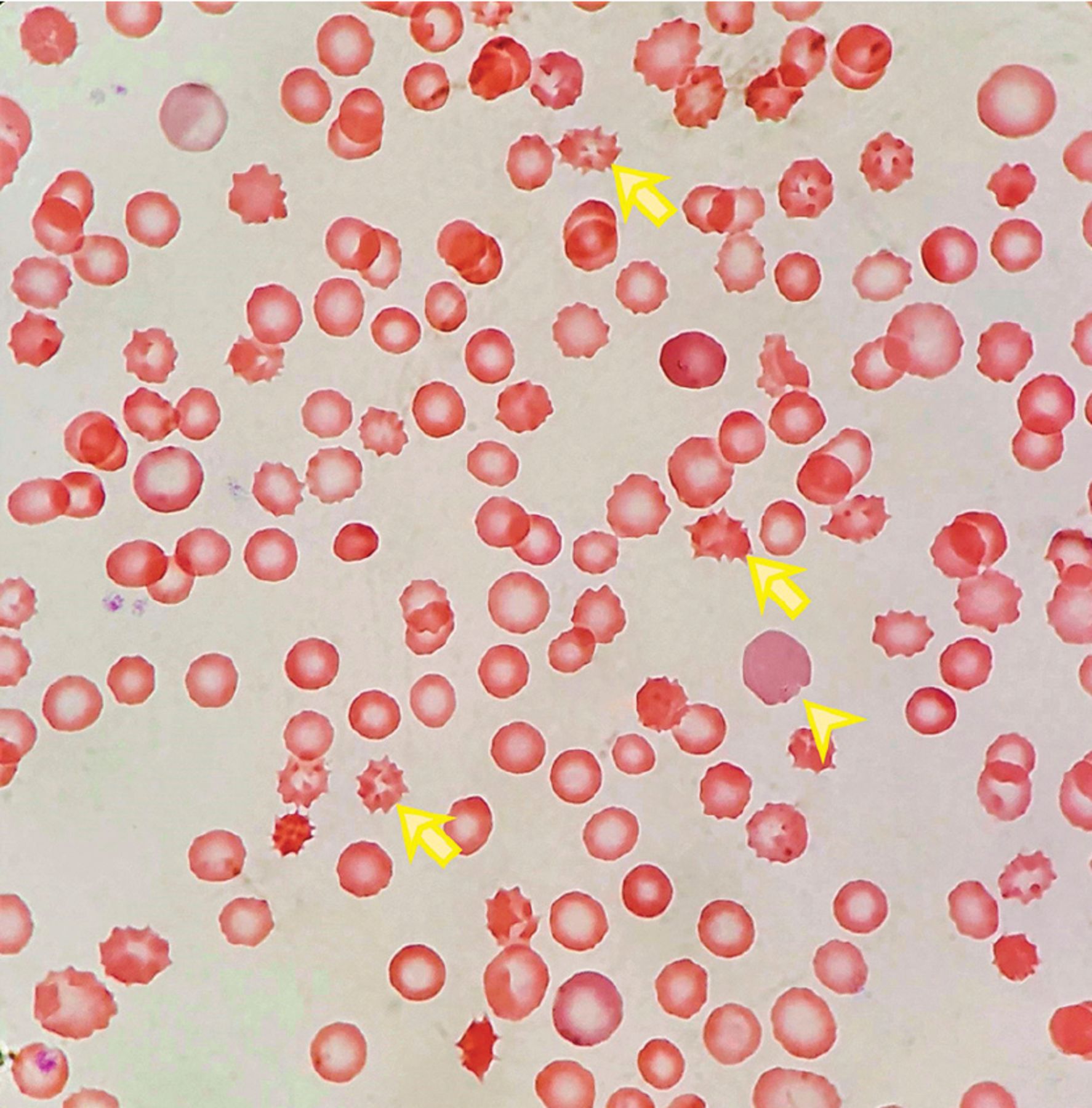
The peripheral blood smear (Figure 1) showed numerous irregularly shaped erythrocytes with spinous projections (ie, acanthocytes, or “spur cells”) and increased reticulocytes, confirming the diagnosis of spur-cell anemia.
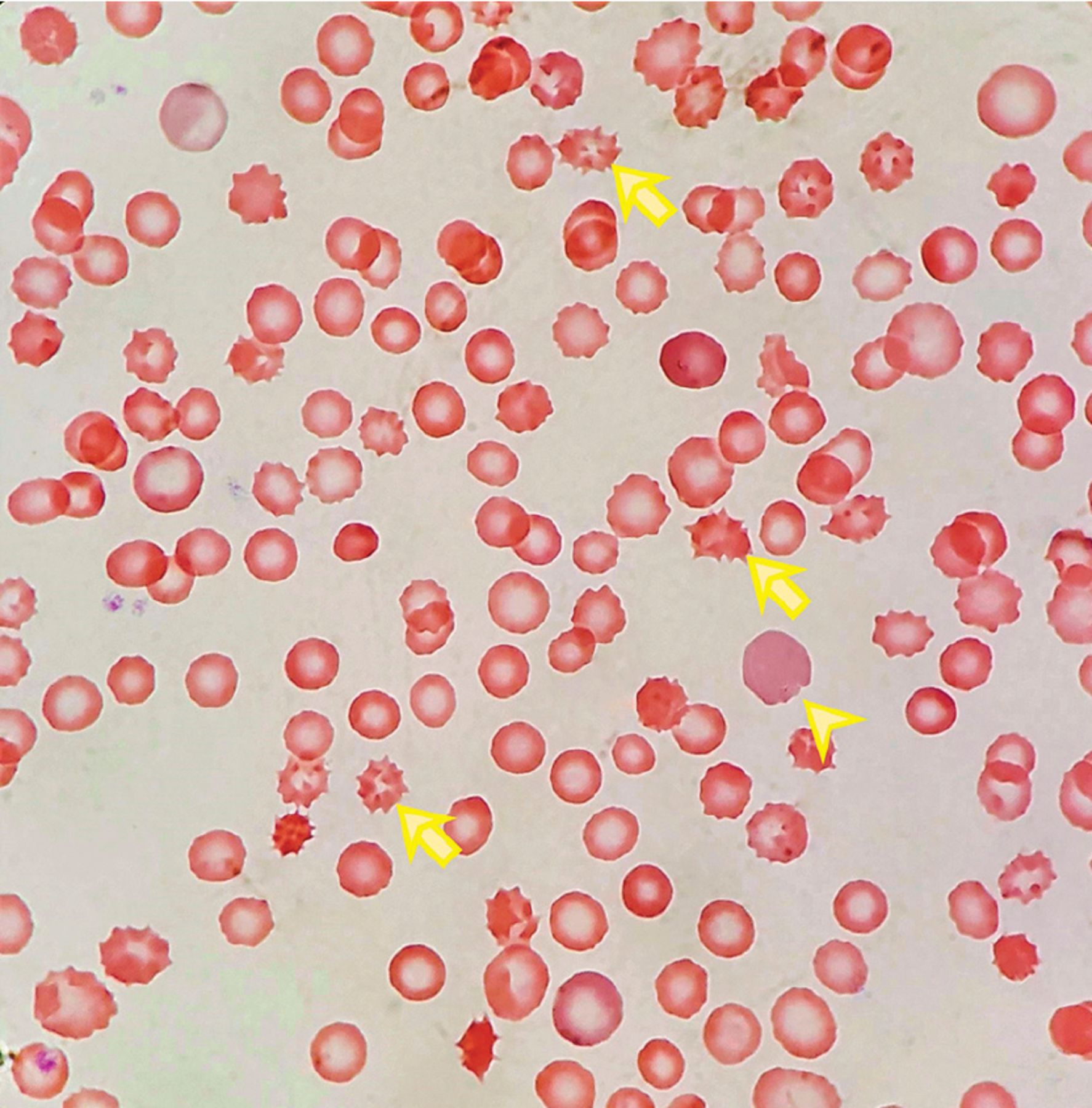
A peripheral blood smear showed numerous irregularly shaped erythrocytes with spinous projections (“spur cells”) and increased reticulocytes.
HEMOLYTIC ANEMIA IN HEPATIC FAILURE
Hemolysis in hepatic failure is often overlooked as a cause of anemia. These patients often have decreased haptoglobin, elevated lactate dehydrogenase, and hyperbilirubinemia at baseline.
When Coombs-negative hemolysis is suspected in liver failure, the peripheral blood smear should be reviewed for morphologic abnormalities. Abnormal lipid and protein metabolism results in erythrocyte membrane defects—commonly, macrocytosis and target cells. These erythrocytes lose their plasticity and are deformed as they travel through the spleen, resulting in the formation of spur cells and increased clearance in the reticuloendothelial system. Zieve syndrome is a triad of jaundice, hypertriglyceridemia, and hemolysis.1
MANAGEMENT IS MAINLY SUPPORTIVE
Spur-cell anemia is associated with a poor prognosis, and liver transplant is the only definitive management.2 Supportive management includes transfusion for symptomatic anemia, discontinuation of bone marrow-suppressive medications and alcohol, and appropriate treatment for the primary cause of liver disease. Medical management with prednisolone or pentoxifylline is based only on limited case reports, and further research is needed.3,4
Recurrence of spur-cell anemia after transplant can herald graft failure.5
Our patient’s care
Our patient was not a candidate for transplant because of his ongoing alcohol use. He was enrolled in palliative care and died 1 month later.
Footnotes
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.