


Article Figures & Data
Figures
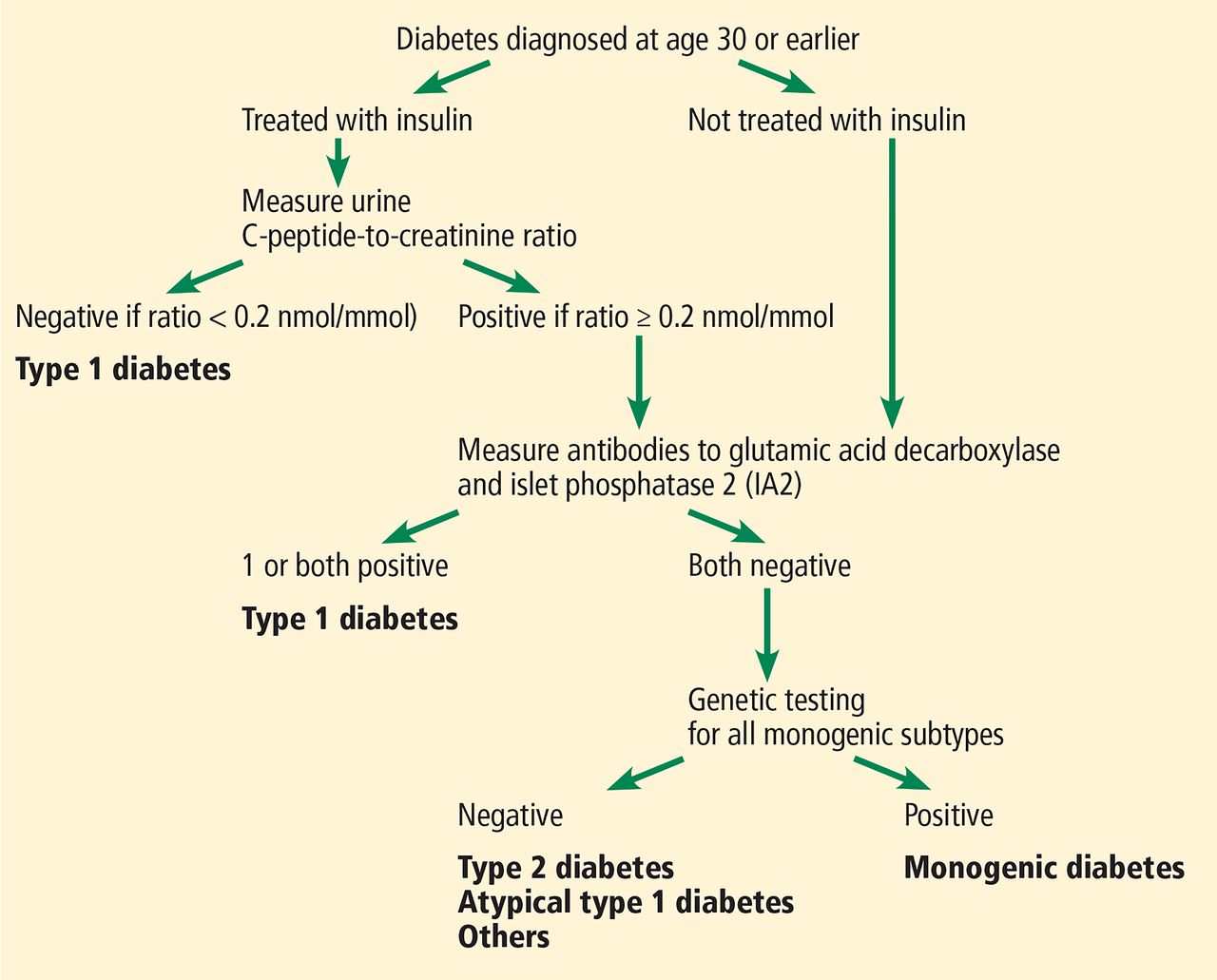
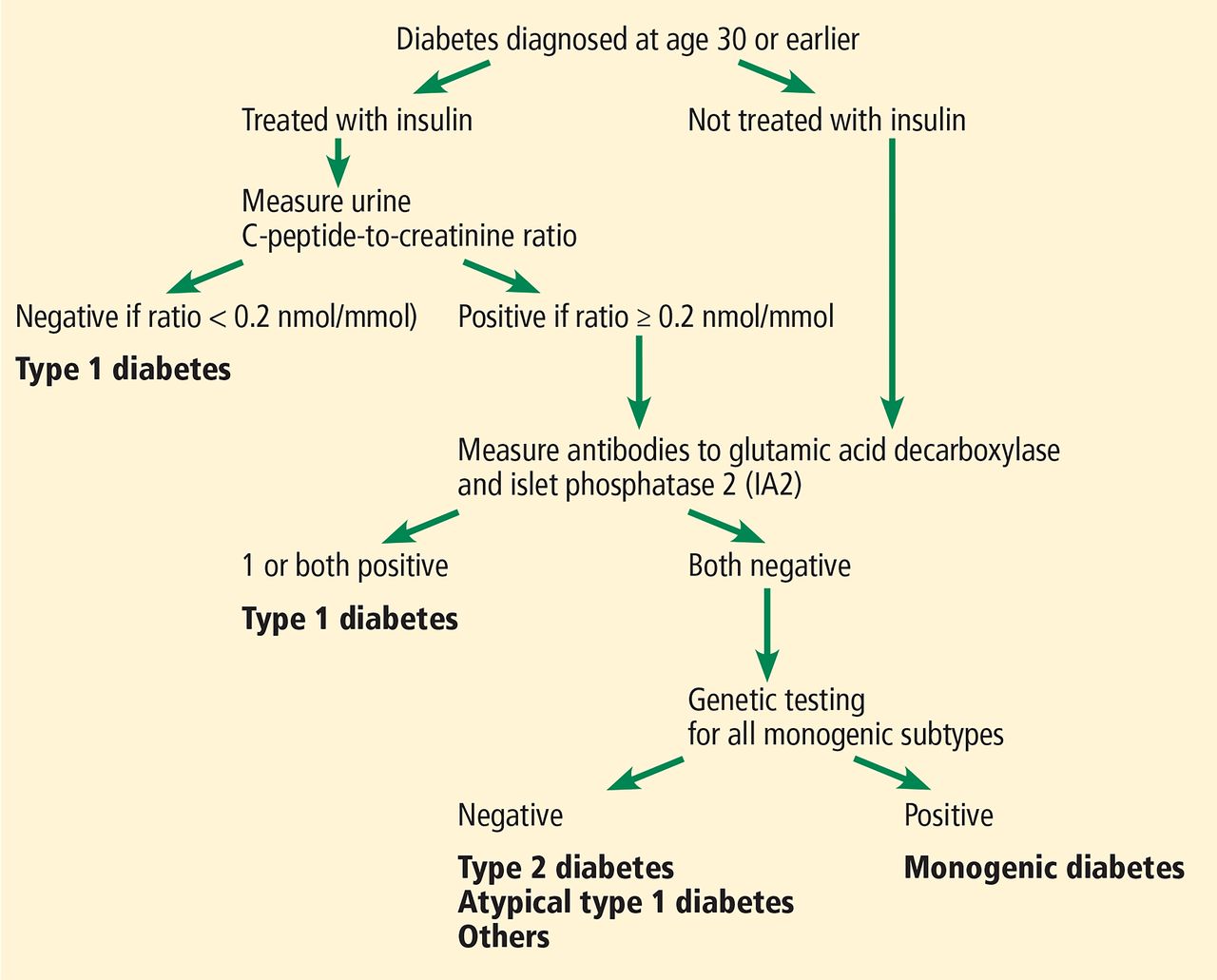
- Figure 1
The Using Pharmacogenetics to Improve Treatment in Early-Onset Diabetes (UNITED) biomarker screening pathway to investigate the etiology of diabetes diagnosed in patients age 30 or younger. Genetic testing is carried out in all patients who have endogenous insulin (urinary C-peptide-to-creatinine ratio ≥ 0.2 nmol/mmol) and do not have either glutamic acid decarboxylase or IA2 autoantibodies. Patients without endogenous insulin or with these antibodies are classified as having type 1 diabetes.
American Diabetes Association. Shields BM, Shepherd M, Hudson M, et al; UNITED study team. Population-based assessment of a biomarker-based screening pathway to aid diagnosis of monogenic diabetes in young-onset patients. Diabetes Care 2017; 40(8):1017–1025. Copyright and all rights reserved. Material from this publication has been used with the permission of American Diabetes Association.
Tables
Type Insulin level Auto-immune Genetic features Glucose-lowering treatments Type 2 diabetes mellitus8,10,14,36,37 High, but decreases over time No Multiple single nucleotide polymorphisms (SNPs), but no single SNP specifically associated with diabetes Multiple Level of hyperglycemia and comorbid conditions guide decisions MODY14–19,25 Variable No Autosomal-dominant and recessive Sulfonylureas for 2 genotypes (HNF4A, HNF1A); no medication for 1 genotype (GCK) Flatbush26–28 Variable No Unknown Insulin, followed by therapies for type 2 diabetes mellitus Lipo-dystrophy39–41 High No Yes, for genetic types Insulin, metformin, thiazolidinediones, metreleptin Type 1 diabetes mellitus11 Low Yes Yes, human leukocyte antigen (HLA) system- related Insulin LADA29–34 Low Yes Yes, HLA system- related and some novel genes Insulin Secondary diabetes Cushing disease, acromegaly Usually high secondary to counterregulatory hormones No No See type 2 diabetes mellitus above Medication-related Variable; high with glucocorticoids No No See type 2 diabetes mellitus above LADA = latent autoimmune diabetes in adults; MODY = maturity-onset diabetes of youth
Monotherapy is usually inadequate for glycemic control Medications that work by different mechanisms have additive effects for glucose control Insulin therapy can be broadly used as monotherapy or in combination with other agents Sodium-glucose cotransporter 2 (SGLT2) inhibitors have benefits in terms of renal failure, heart failure, and major adverse cardiovascular events (including death) Some glucagon-like peptide 1 receptor agonists (liraglutide,48 dulaglutide,49 and semaglutide,50 but not lixisenatide51 or exenatide [weekly formulation])52 reduce risk of major adverse cardiovascular events Comorbidities of diabetes affect the selection of glucose-lowering medications In renal compromise: Metformin poses risk of lactic acidosis; do not initiate if estimated glomerular filtration rate (eGFR) is < 45 mL/min/1.73 m2; but patients currently on metformin with eGFR ≥ 30 and < 45 mL/min/1.73m2 may continue cautiously, considering a 50% reduction and frequent monitoring of renal function; discontinue if eGFR is < 30 mL/min/1.73 m2 Adjust dose of dipeptidyl peptidase 4 (DPP4) inhibitors SGLT2 inhibitors have reduced efficacy In heart failure or risk of heart failure: Discontinue peroxisome proliferator-activated receptor (PPAR) gamma agonists Use DPP4 inhibitors (saxagliptin, alogliptin) with caution In hypoglycemia: Avoid sulfonylureas Adjust dose of insulin Based on information in references 45–52.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.