


ABSTRACT
Endoscopic ultrasonography (EUS) has been used since the mid-1980s. Initially a diagnostic tool, it has since evolved into a therapeutic, minimally invasive surgical tool with significant impact on the diagnosis and management of a range of benign and malignant conditions. The authors review current indications, safety, and efficacy of EUS for diseases of the upper and lower gastrointestinal tract, posterior mediastinum, pancreas, bile duct, gallbladder, retroperitoneum, liver, adrenal glands, and kidneys.
EUS is commonly used in the diagnosis and management of biliary and pancreatic diseases, including guidance of biliary drainage in bile duct or pancreatic duct obstruction.
EUS-guided fine-needle aspiration aids staging of malignancies of the upper and lower digestive tract.
EUS is now increasingly used to drain abdominal fluid collections of nonpancreatic etiology.
Endoscopic ultrasonography (EUS) has evolved from a diagnostic tool to a therapeutic procedure for a wide range of conditions of the upper and lower gastrointestinal tract, hepatobiliary system, pancreas, adrenal glands, kidneys, retroperitoneum, and lymph nodes around the gastrointestinal tract. It can help differentiate benign from malignant disease and in many cases is an alternative to surgery.
This review of current and evolving diagnostic and therapeutic indications for EUS will help physicians identify patients who may benefit from this procedure.
EUS VS OTHER IMAGING TESTS
EUS offers advantages over other imaging tests. It does not involve radiation as in computed tomography (CT) or positron emission tomography, and it is not subject to the contraindications of magnetic resonance imaging (MRI) such as metal implants or claustrophobia. EUS offers high-resolution real-time imaging and can be combined with Doppler to evaluate vasculature and perform diagnostic procedures, angiotherapy, fine-needle aspiration biopsy, and core biopsy for tissue diagnosis. In addition, EUS allows therapeutic interventions.1
PROCEDURAL REQUIREMENTS FOR THE PATIENT
EUS is an outpatient procedure that usually takes 30 to 60 minutes and can be done under moderate sedation or general anesthesia.
Periprocedural considerations
According to guidelines of the American Society for Gastrointestinal Endoscopy (ASGE),2 patients fast for 8 hours before the procedure.
For patients taking antithrombotics, guidelines recommend a platelet level greater than 50 × 109/L and an international normalized ratio below 1.5.
The endoscope
EUS is performed with a flexible wide endoscope with a small ultrasound probe and camera at the tip; other equipment in the scope depend on the indication and can include a fine-aspiration needle, a core biopsy needle, a celiac plexus blockade and neurolysis needle, and a metal or plastic stent. EUS can be performed using either a radial (360°) or a linear (approximately 120°) view. A narrow angle of view is required to allow endoscopic fine-needle aspiration.
Expanding indications
The indications for EUS are rapidly expanding. Uses identified by the American Cancer Society and the ASGE now include evaluation and staging of upper gastrointestinal malignancies, mediastinal adenopathy, pancreatic lesions and cancers, submucosal tumors, rectal cancer, and lung cancer staging.3 In particular, EUS has changed the approach to diagnosis and management of biliary and pancreatic diseases.
PANCREATIC DISORDERS
Pancreatic cancer
Pancreatic cancer has a poor prognosis since it is usually diagnosed at an advanced stage. According to the American Cancer Society, the 1-year relative survival rate is 20%, and the 5-year rate is 8% for all stages of pancreatic cancer. Current studies show that EUS has a sensitivity of 90% to 95% for detecting malignant pancreatic tumors measuring 2 cm to 3 cm, which is far superior to other imaging modalities.4 EUS is considered complementary to CT or MRI for diagnosis and staging of pancreatic adenocarcinoma. EUS is also used to rule out pancreatic cancer if results of CT or MRI are ambiguous.
EUS in combination with fine-needle aspiration biopsy improves diagnostic accuracy for pancreatic masses and helps in histologic confirmation.5 Immediate cytologic evaluation or rapid on-site cytologic evaluation helps improve the yield.
The sensitivity of EUS declines in the setting of severe underlying chronic pancreatitis or severe acute pancreatitis. The challenges of detecting pancreatic malignancy in the setting of chronic pancreatitis are being addressed with the advent of EUS elastography, which evaluates tissue stiffness and helps with characterization of the lesion.6
Acute pancreatitis
Gallstones are the most common cause of acute pancreatitis. EUS has higher sensitivity than ultrasonography, CT, and magnetic resonance cholangiopancreatography in detecting common bile duct stones and sludge in patients with acute pancreatitis or recurrent pancreatitis.7
The ASGE recommends EUS for the assessment of choledocholithiasis in patients at intermediate risk. If EUS confirms bile duct stones, therapeutic endoscopic retrograde cholangiopancreatography (ERCP) can be performed with the patient under the same sedation; and if a stone is not present, an additional diagnostic procedure can be avoided.2
EUS also helps determine other causes of acute pancreatitis such as pancreas divisum, small pancreatic tumors undetected on CT or MRI, autoimmune pancreatitis, and chronic pancreatitis, and it can be an important investigative test in patients with idiopathic pancreatitis.8
Pancreatic fluid collections
The revised Atlanta classification categorizes pancreatic fluid collections according to 4 types9:
Acute peripancreatic fluid collection, occurring in interstitial edematous pancreatitis
Pancreatic pseudocyst, occurring as a delayed complication (> 4 weeks) of interstitial edematous pancreatitis
Acute necrotic collection, occurring in necrotizing pancreatitis
Walled-off necrosis, which has a radiologically identifiable capsule (> 4 weeks).
Surgical and percutaneous approaches have traditionally been used to drain symptomatic pancreatic and peripancreatic fluid collections.10 However, disadvantages of these procedures include higher cost, longer hospital stay, possibly higher morbidity risk, and discomfort of external catheters requiring multiple exchanges.
In the past few years, EUS-guided transgastric or transduodenal drainage has been used more frequently with comparable success and lower morbidity and costs than surgical and percutaneous drainage. The procedure is feasible in more than 90% of patients, is minimally invasive, and results in shorter hospital stays than surgical drainage, and compared with CT or MRI, it more accurately differentiates pseudocyst from cystic neoplasms.11
Complications of endoscopic drainage of pancreatic fluid collections are minimal and include bleeding, perforation, and infection, all with rates of less than 5%.12
Chronic pancreatitis
Chronic pancreatitis is a complex disease with an ill-defined epidemiology but significant rates of morbidity and mortality. Smoking and alcohol consumption are main risk factors. Chronic abdominal pain is the most common presentation.
Diagnosis can be challenging in early, mild, or moderate disease. Studies13–16 have shown that the diagnostic accuracy of EUS is comparable to that of ERCP and pancreatic function testing. In addition, technologic advances in EUS such as contrast-enhanced harmonics and elastography offer improved diagnostic accuracy in patients with chronic pancreatitis.17,18 As a result, EUS is being increasingly used as a frontline test for this indication.
Pancreatic cystic neoplasms
The challenge in management of pancreatic cystic neoplasms lies in the timely and accurate diagnosis of premalignant mucinous cysts.
Differentiation of premalignant mucinous cysts from benign nonmucinous cysts by EUS with fine-needle fluid aspiration has become a valuable tool, providing high-quality imaging of the cyst and samples for fluid analysis, leading to increased diagnostic accuracy.
Periprocedural antibiotics are administered to minimize the risk of infection from fine-needle aspiration. Cyst fluid samples are sent to the laboratory for cytologic study and for analysis for carcinoembryonic antigen, glucose, amylase, and mucin.19,20 Premalignant mucinous cysts are managed according to the international consensus guidelines.21,22
GALLBLADDER AND BILIARY DISORDERS
Choledocholithiasis
Common bile duct stones can be present in 20% of patients with cholelithiasis. Noninvasive imaging with abdominal ultrasonography or CT has a diagnostic accuracy of only 50% for these stones. Magnetic resonance cholangiopancreatography is the most accurate noninvasive imaging test (diagnostic accuracy from 81% to 99%).23–26
ERCP and intraoperative cholangiography are accurate but invasive and can cause complications. Same-session EUS and ERCP (if stones are confirmed on EUS) for common bile duct stones are usually performed in patients with intermediate probability of stones according to the ASGE criteria or in patients with contraindications to magnetic resonance cholangiopancreatography.
Obstructive jaundice
Obstructive jaundice can result from benign and malignant diseases. Common benign causes are choledocholithiasis, postcholecystectomy bile duct injury, liver transplant, portal cavernoma cholangiopathy, primary sclerosing cholangitis, acquired immunodeficiency syndrome cholangiopathy, chronic pancreatitis, and immunoglobulin G4 cholangiopathy. Malignant causes include cholangiocarcinoma, gallbladder carcinoma, pancreatic malignancies, ampullary carcinoma, metastasis, metastatic lymph nodal compression on bile duct, and hepatocellular carcinoma. The proximity of the stomach and duodenum to the extrahepatic biliary system makes EUS useful for imaging the biliary anatomy. EUS-guided fine-needle aspiration from the bile duct wall and surrounding lymph nodes enables histologic diagnosis.
ERCP is the standard procedure for biliary drainage in benign or malignant biliary obstruction. However, it is not feasible in surgically altered anatomy as in Roux-en-Y anastomosis and duodenal bulb infiltration by tumor. In these cases, EUS-guided biliary drainage is being used with high success rates.27,28 EUS-guided cholangiopancreatography has been done in patients in whom ERCP could not be performed. This procedure requires a high level of technical expertise and can cause complications such as perforation and bile leak.
Cholecystitis
Cholecystectomy is the optimal treatment for acute calculous or acalculous cholecystitis. Patients deemed high-risk surgical candidates cannot undergo the procedure and traditionally undergo percutaneous placement of a cholecystostomy tube by interventional radiology for decompression of the gallbladder. EUS can be used to perform transgastric or transduodenal gallbladder drainage with a covered metal stent. Case series have shown outcomes comparable to those of percutaneous tube placement.29,30
GASTROINTESTINAL TRACT DISEASE
Upper tract conditions
EUS can be used to identify benign tumors of the upper gastrointestinal tract, includ ing submucosal esophagogastric tumors.31 EUS-guided fine-needle aspiration and biopsy can aid the cytohistologic diagnosis of esophagogastric solid subepithelial lesions.32
EUS is routinely used for diagnosis and staging of malignant esophageal tumors. The procedure may not be technically feasible if high-grade malignant esophageal stricture precludes passage of echoendoscope.
EUS-guided evaluation and biopsy are particularly useful to diagnose linitis plastica, a gastric cancer characterized by marked thickening of deeper layers of gastric wall. It is difficult to diagnose with superficial mucosal biopsies rendered with esophagogastroduodenoscopy.
Mediastinal adenopathy and non-small-cell lung cancer
Nearly 26% of lung cancer patients present with mediastinal lymph node involvement.33 CT, MRI, and positron emission tomography are the common modalities for diagnosing mediastinal lymph node enlargement. However, lack of tissue sampling results only in a presumptive diagnosis. Posterior and inferior mediastinal lesions are especially suitable for EUS-guided fine-needle aspiration and biopsy for histologic diagnosis, thus avoiding an invasive surgical intervention like mediastinoscopy. However, EUS is unable to visualize anterior upper mediastinal nodes.
Mediastinal staging in lung cancer is an area in which EUS has made most significant impact.34 It also allows for evaluation of distant metastases involving adrenal glands.
Submucosal lesions
EUS provides a detailed image of gastrointestinal wall layers and therefore has become the principal tool for assessment of submucosal masses in this area.
Gastrointestinal stromal tumors are the most common mesenchymal tumors, and the stomach is the most common site. EUS-guided fine-needle aspiration is considered the procedure of choice for preoperative diagnosis of these tumors, although it may provide inadequate material in one-third of cases. However, with the advent of newer biopsy needles, the histologic yield has improved significantly.
In addition to the diagnosis of gastrointestinal stromal tumors, EUS can distinguish between other benign lesions (leiomyoma, pancreatic rest, indolent neuroendocrine tumor, granular cell tumor, schwannoma, duplication cyst) and malignant lesions (primary or metastatic). EUS elastography is a promising technique that may also improve the distinction of benign from malignant lesions.
Retroperitoneal masses
For evaluation of idiopathic abdominal masses, EUS-guided fine-needle aspiration and biopsy provide a minimally invasive technique to obtain tissue samples for safe and accurate diagnosis, thus avoiding the need for exploratory laparotomy; it also helps guide subsequent therapy.35 These procedures are useful for evaluation of periintestinal and periesophageal lymph nodes and are more accurate than CT.36
Apart from providing adequate diagnostic tissue in lymphoproliferative tumors, EUS is highly useful in nonpancreatic retroperitoneal masses such as adrenal metastasis, leiomyosarcoma, paraganglioma, and lymphangioma. EUS-associated seeding of the needle tract has been reported but is rare.
Lower tract disease
Accurate preoperative staging of rectal cancer leads to targeted treatment strategies, increased cure rates, and reduction in short-term and long-term treatment failure. EUS and MRI have comparable accuracy in TNM staging of colorectal cancer, but MRI is perhaps more advantageous than EUS for nodal staging since it images the entire mesorectum.
CELIAC PLEXUS BLOCK AND NEUROLYSIS
Chronic abdominal pain is common and often disabling in patients with intra-abdominal malignancies and chronic pancreatitis. Pain relief from first-line medications including opiates may be inadequate or fraught with intolerances and adverse effects.37
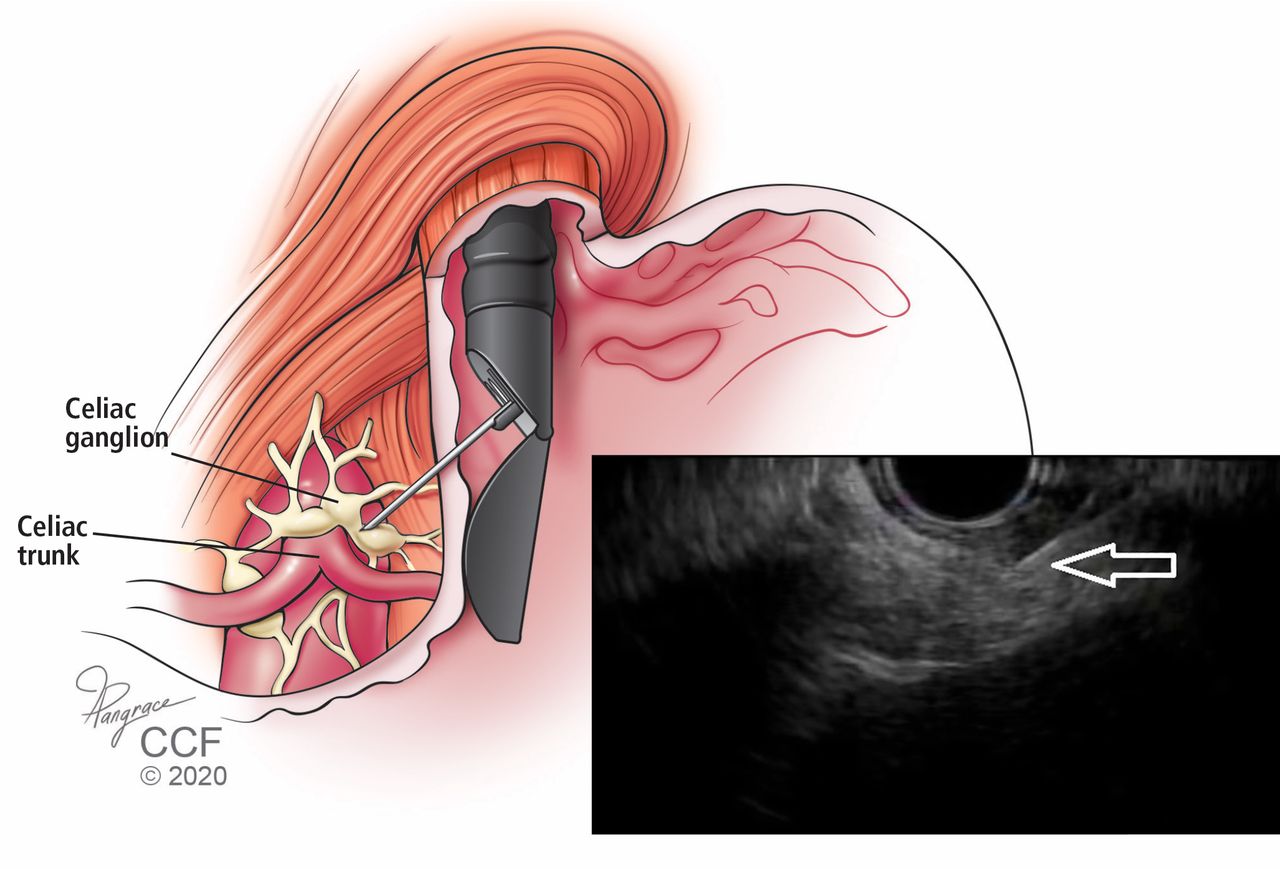
Celiac plexus block with CT-guided percutaneous and EUS-guided neurolysis has been shown to be safe and technically easy to perform (Figure 1). In a Cochrane review of 6 randomized controlled trials with a total of 358 pancreatic cancer patients,38 the authors found that celiac plexus block with either approach caused fewer adverse effects than opioid analgesia. More study is needed to confirm a statistically significant improvement in pain scores.

Control of chronic abdominal pain with first-line medications in patients with chronic pancreatitis or intra-abdominal malignancy may be inadequate or fraught with adverse effects. One alternative is endoscopic ultrasonography-guided fine-needle (EUS) celiac plexus block, performed under echoendoscopic guidance with passage of an injection needle. This procedure has been shown to be safe, is technically easy to perform, and is a safe alternative to percutaneous block guided by computed tomography. The arrow shows the EUS-guided placement of the needle.
RECENT DEVELOPMENTS, NEWER INDICATIONS
EUS-guided fine-needle injection
EUS-guided fine-needle injection is being evaluated for intratumoral chemotherapy in pancreatic and esophageal cancers. It has been used for tissue ablation by injection of ethanol in nonmalignant pancreatic cystic tumors and in radiofrequency ablation and brachytherapy in unresectable pancreatic cancers. Portal injection of chemotherapy has been shown to be safe and feasible. It may prove useful in the management of primary liver malignancies.
EUS-guided botulinum toxin injection for achalasia and for management of obesity has been done in few cases. Botox administration in the stomach promotes early satiety and weight loss through inhibition of acetylcholine-mediated peristalsis, ultimately delaying gastric emptying.39
EUS-guided gastrojejunostomy
Gastric outlet obstruction can result from malignancies involving stomach, duodenum, gallbladder, or pancreas. EUS-guided gastrojejunostomy has been reported to be a safe, durable, and successful treatment option.40–42 Compared with enteral (duodenal) stenting, which can be complicated by tumor ingrowth resulting in stent occlusion, EUS-guided gastrojejunostomy has been shown to provide longer-lasting symptom relief since it is performed remotely from the tumor location. It also offers shorter recovery time and is more cost-effective than surgical gastrojejunostomy.43,44
Contrast-enhanced harmonic EUS
Contrast-enhanced harmonic EUS has been developed to detect a microvascular pattern of lesions, which can help differentiate benign from malignant disease. An intravascular contrast agent is injected that contains microbubbles. On exposure to ultrasound, these microbubbles oscillate, and the transducer can make out the appearance of the peripheral microvasculature.45
Molecular marker analysis
DNA analysis of specimens obtained by EUS-guided fine-needle aspiration can aid diagnosis. Microdissection-based genotyping is now available at some centers. This has specific value in distinction of pancreatic cysts seen on CT. DNA quantification can help distinguish benign cysts from malignant ones.
EUS-directed transgastric ERCP in patients with gastric bypass
Duodenal and ampullary access with ERCP is difficult in patients who have undergone Roux-en-Y gastric bypass. Classically, enteroscopy-assisted ERCP is associated with a low success rate. Surgically assisted ERCP (laparoscopy or laparotomy) has a good success rate but is more invasive, has higher complication rates and longer length of stay in the hospital, with associated costs.
EUS-directed transgastric ERCP involves accessing the excluded stomach from the gastric pouch or Roux limb by creation of a fistula with placement of a removable lumen-apposing metal stent. Conventional ERCP can then be performed through the stent. A multicenter study comparing the EUS-directed procedure and laparoscopic ERCP found that the 2 procedures had similar success rates and adverse events.46 The EUS-directed procedure has the benefit of being an outpatient minimally invasive procedure with significantly shorter procedure time and cost.46,47
Drainage of other nonpancreatic abdominopelvic fluid collections
EUS is safe and effective in accessing and draining nonpancreatic abdominopelvic fluid collections from the stomach, duodenum, and colon. Multiple case series have reported safe and successful drainage of subphrenic abscesses, hepatic abscesses, bilomas, and pelvic and retroperitoneal abscesses. In addition, EUS has been increasingly utilized to drain postsurgical fluid collections, which can form anywhere in the abdominal cavity and can become symptomatic or infected. There is mounting recent evidence of successful EUS-guided drainage of such collections after common surgical procedures including Whipple surgery and Roux-en-Y gastric bypass.48
EUS-guided angiotherapy
EUS-guided angiotherapy is a relatively novel application that allows control of variceal bleeding by injecting coils and cyanoacrylate glue directly into the varices and confirming the thrombosis in real time with Doppler. It is purported that the combination of coil and glue might decrease the risk of glue embolization. However, further study is needed to establish the safety and superiority of this technique.34,49,50
DRAWBACKS AND COMPLICATIONS
Adverse events associated with sedation and standard endoscopic procedures are also applicable to EUS. However, since the echoendoscope has a larger diameter with a stiffer tip than the standard endoscope, it can be difficult to maneuver around the cricopharyngeus and duodenal bulb. It is also more time-consuming than standard routine endoscopy if fine-needle aspiration or intervention is planned. Despite this, complications, as reviewed below, are infrequent.
Perforation
Perforation is reported in the cervical esophagus and less often in the duodenum. The risk is usually similar to that with routine endoscopy (0.03%). A prospective study of 4,894 patients undergoing upper EUS found a cervical esophageal perforation rate of 0.06% (3 patients, with a curved linear array endoscope).51 A recent systematic review reported a perforation rate of 0.02% with EUS.52 The risks may be higher in patients with strictures, malignancy, older age, or history of difficult intubation, and with a less experienced operator.
Infection
The risk of bacteremia after EUS-guided fine-needle aspiration is lower than with diagnostic endoscopy, and prophylactic antibiotics are not recommended for aspiration of solid masses and lymph nodes.53,54 Some experts recommend prophylactic antibiotics as well as 48 hours of antibiotics after fine-needle aspiration of the perirectal space.55
EUS-guided aspiration of cystic lesions may carry an increased risk of febrile episodes and possibly sepsis. Therefore, prophylactic antibiotics followed by a short postprocedure course has been recommended.56
There have been isolated reports of streptococcal sepsis, mediastinitis, retroperitoneal abscess, perirectal abscess, and cholangitis.57
Pancreatitis
EUS-guided fine-needle aspiration of pancreatic lesions involves direct passage of the needle through pancreatic tissue. Reported rates of pancreatitis associated with this procedure range from 0% to 2%.58 A recent meta-analysis of 51 studies found a rate of of 0.44%.59
Hemorrhage
A recent meta-analysis of related adverse events reported a bleeding rate of 0.13%.59
Avoiding complications
Careful patient selection, familiarity with the equipment, and planning of the procedure are keys to avoiding complications. Early recognition of complications and prompt intervention can reduce morbidity and mortality risk.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.