


Article Figures & Data
Figures
- Figure 1
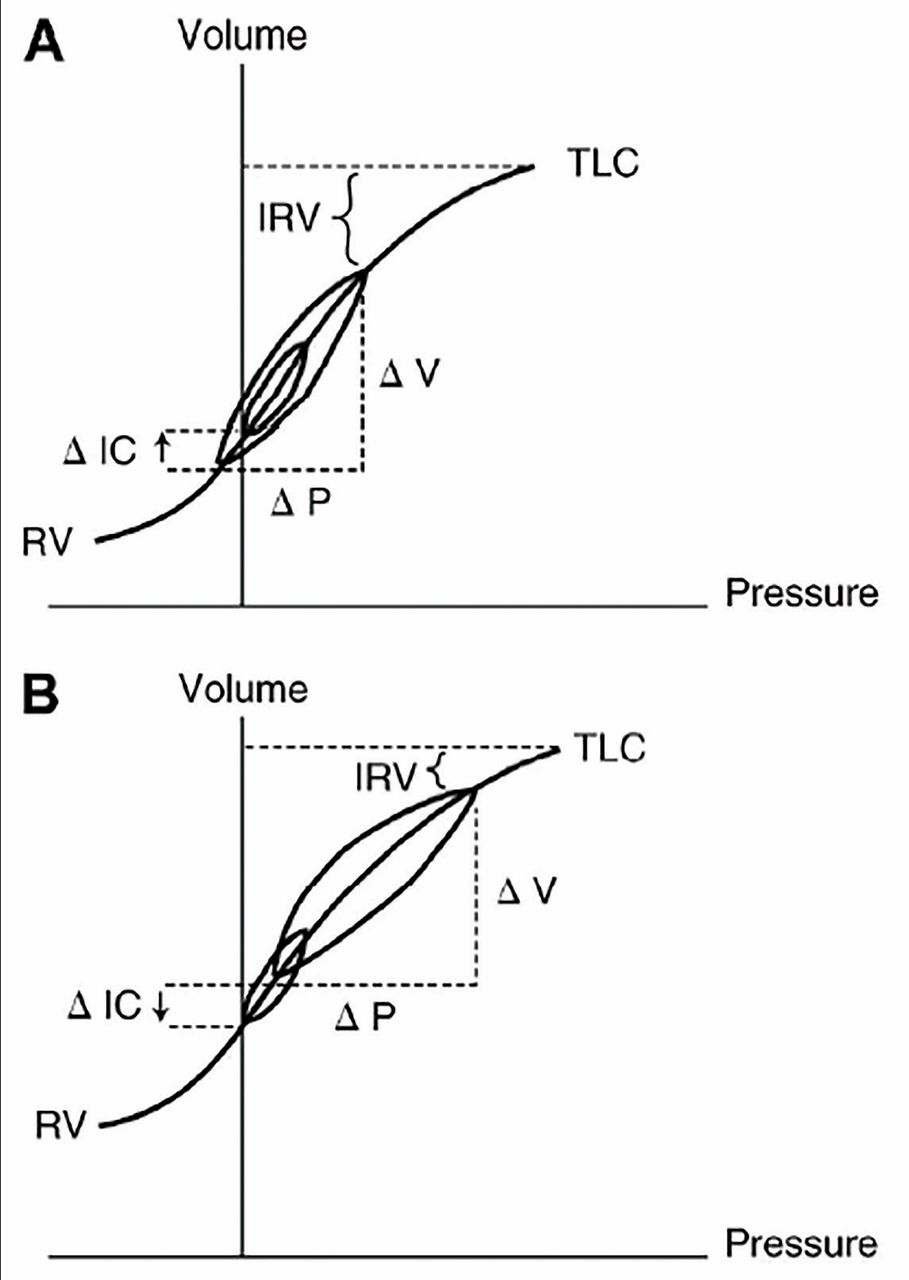
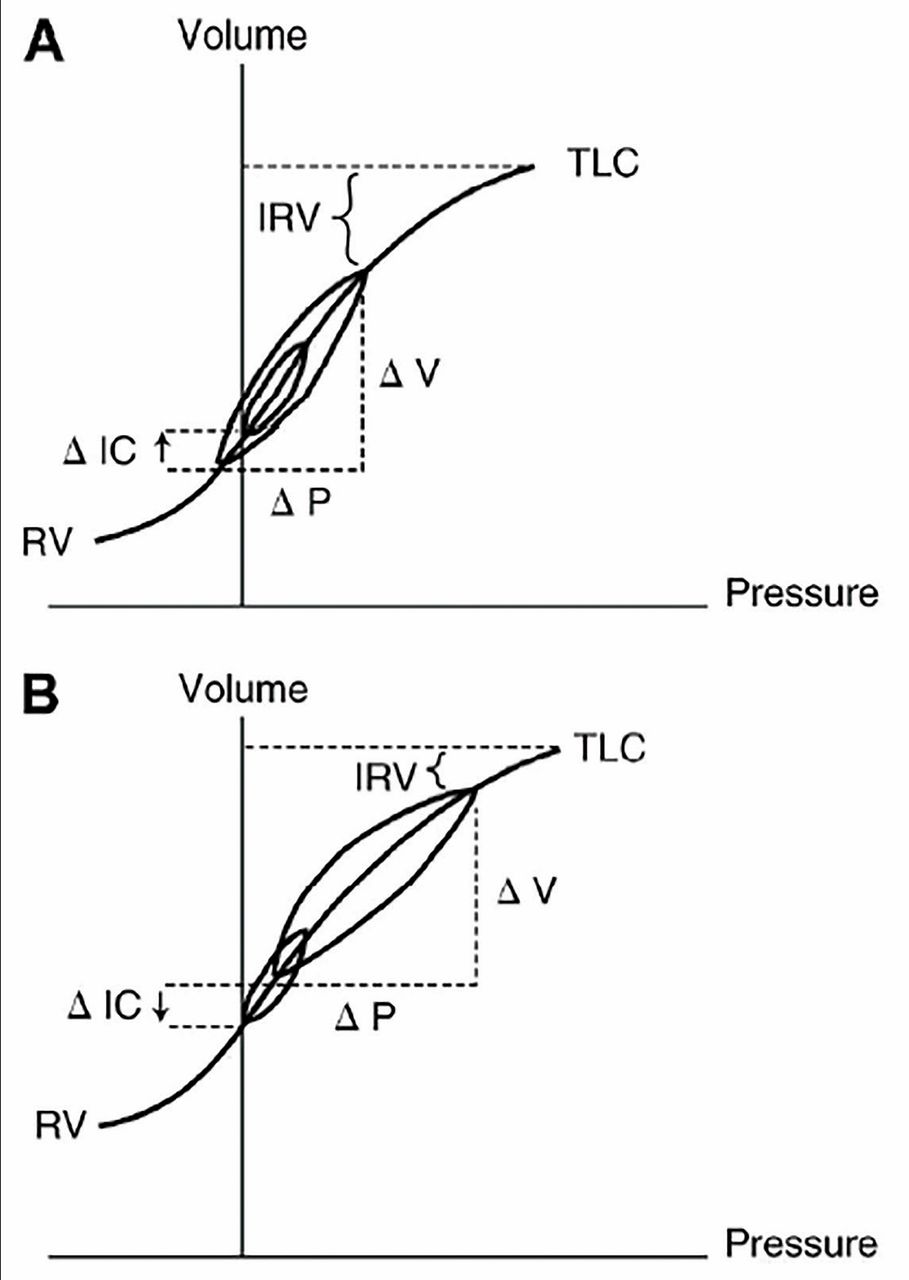
Pressure-volume loops while breathing at rest and during exercise in a healthy individual (A) and in a patient with chronic obstructive pulmonary disease (COPD) (B). Inspiratory capacity (maximum volume of breath that can be taken in after exhalation) increases in healthy people during exercise owing to a fall in lung volume at the end of exhalation. The volume loop during normal breathing is situated in the central linear portion of the pressure-volume relationship, which means that relatively small changes in pressure produce comparatively large changes in volume. In COPD, inspiratory capacity declines due to progressive air-trapping during exercise; thus, patients have to breathe at the upper and less compliant portion of the pressure-volume relationship. This means that increasingly higher pressures must be generated for any given breath, increasing the work of breathing.
IC = inspiratory capacity; IRV = inspiratory reserve volume; P = pressure; RV = residual volume; TLC = total lung capacity; V = volume
Used with the permission of the American Thoracic Society.
- Figure 2
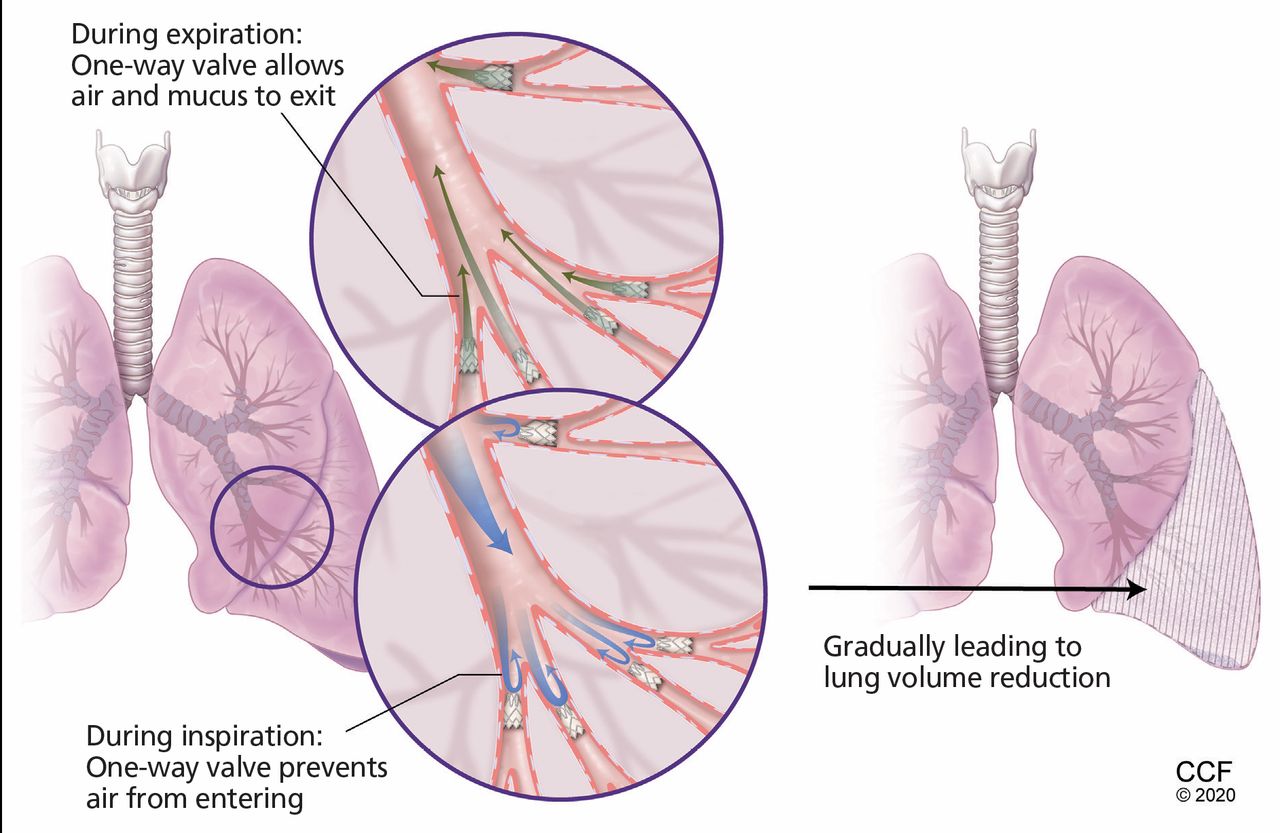
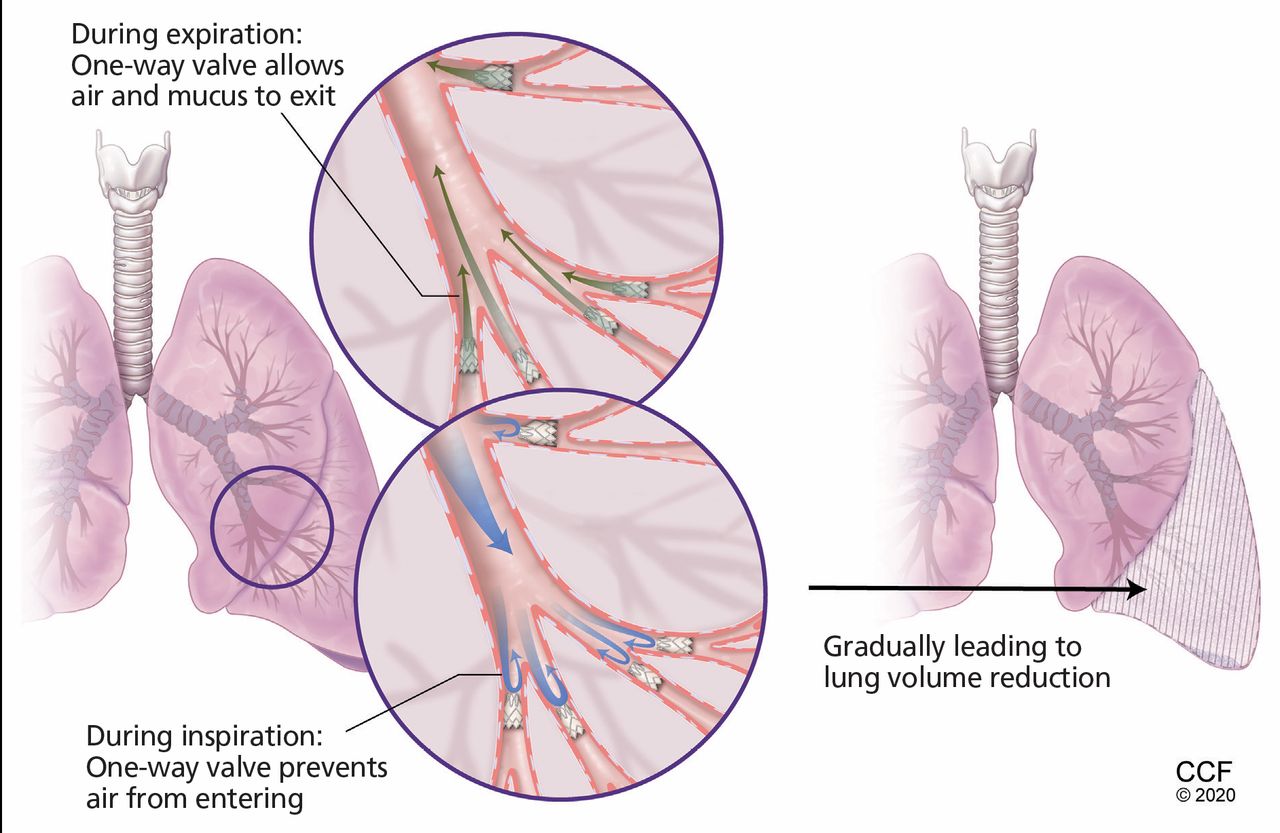
Valve therapy for bronchoscopic lung volume reduction involves implantation of 1-way valves to allow air flow and mucus clearance outward to central airways. The 1-way flow leads to selective de-aeration and collapse of treated areas, reducing hyperinflation and air trapping. Unlike lung volume reduction surgery, the procedure is performed unilaterally due to the inherent procedural risk of pneumothorax.
- Figure 3
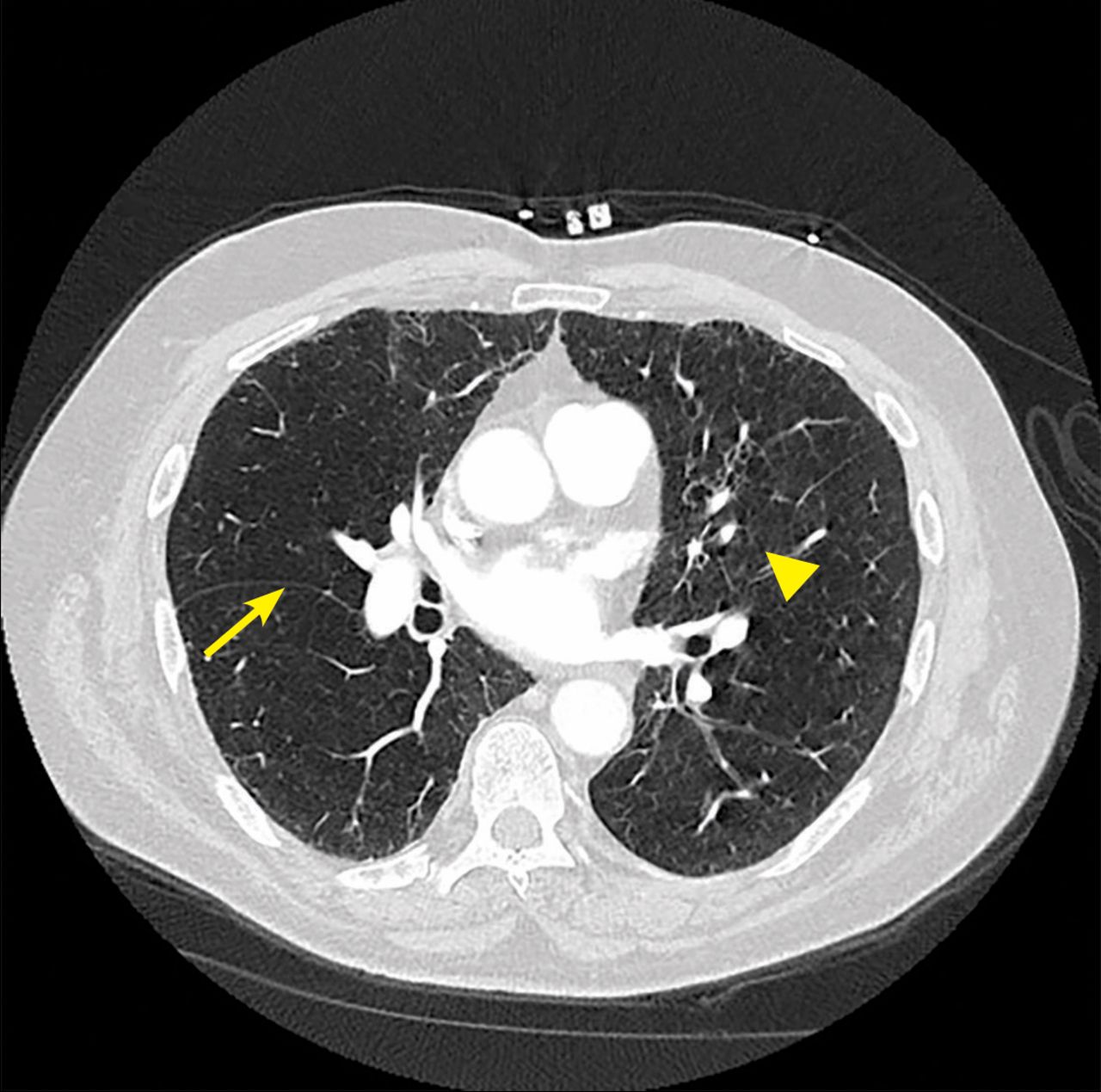
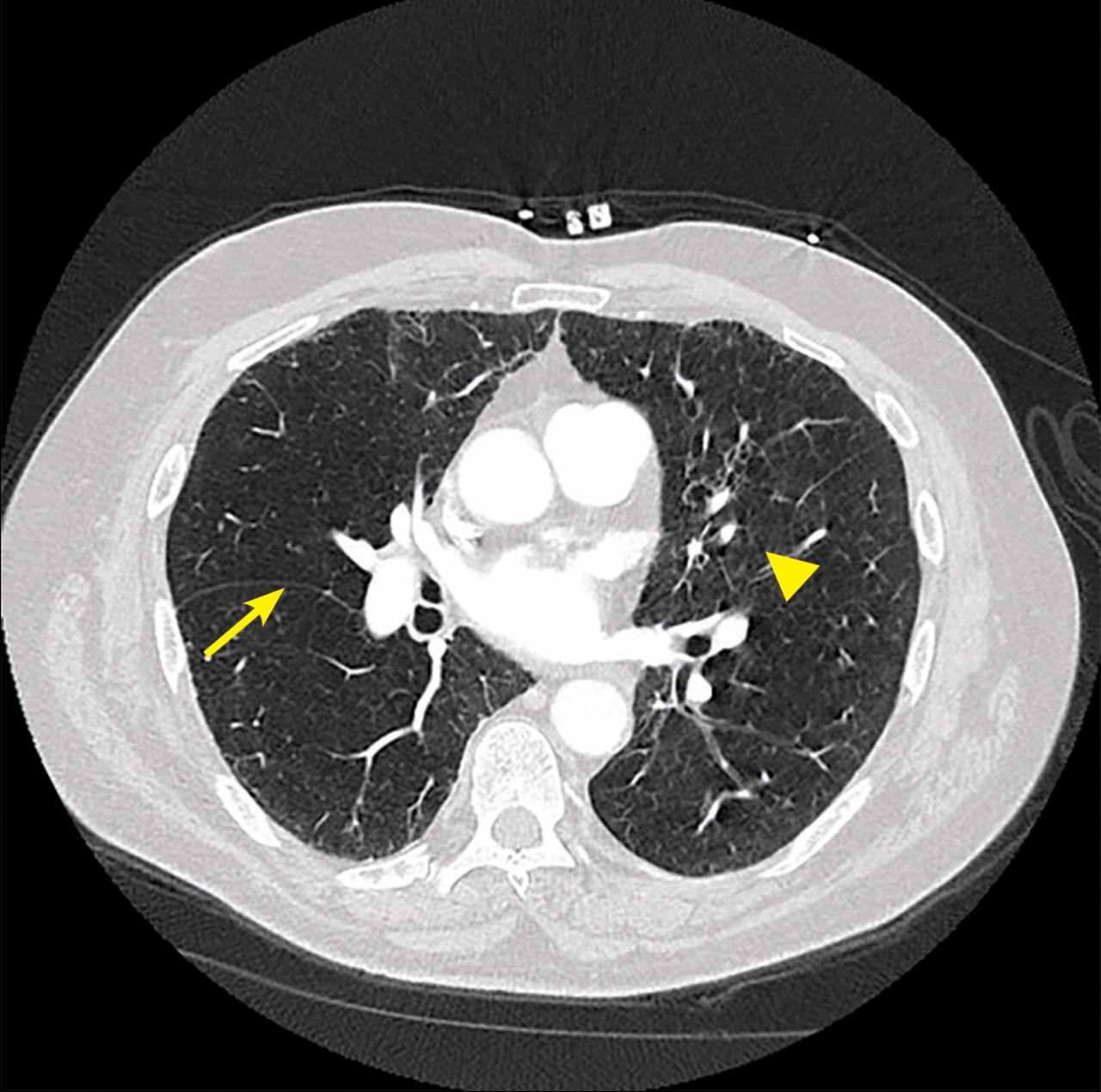
Specialized computed tomography software allows objective quantification of fissure integrity. The arrow indicates a complete fissure, and the arrowhead indicates incomplete fissure. Collateral ventilation is considered highly likely when the fissure is incomplete by > 20% across its span. This is a contraindication to valve therapy.
Tables
Valve therapy: Zephyr and Spiration Lung volume reduction coils: PneumRx10 Airway bypass stents (abandoned due to lack of efficacy and high complication rate)11 Bronchoscopic thermal vapor ablation (inducing scarring in the diseased airways leading to lung volume reduction)12 Biologic or polymeric lung volume reduction: fibrin-thombin mixtures, glue, polymeric foam sealant (the AeriSeal System)13-16 BELIEVER-HIFI19 2015 (N=50) STELVIO20 2015 (N=68) IMPACT21 2016 (N=93) TRANSFORM22 2017 (N=97) LIBERATE23 2018 (N=190) REACH24 2019 (N=107) EMPROVE25 2018 (N=172) Design Single-center 1:1; BLVR vs sham procedure over 3 months Single-center 1:1;BLVR vs standard care over 6 months Multicenter 1:1; BLVR vs standard care over 3 months Multicenter 2:1; BLVR vs standard of care over 3 months Multicenter 2:1; BLVR vs standard care over 12 months Multicenter 2:1; BLVR vs standard care over 3 months Multicenter 2:1; BLVR vs standard care over 12 months Emphysema type Heterogeneousa Heterogeneous, homogeneous Homogeneousb Heterogeneousc Heterogeneousd Heterogeneousd Heterogeneousc Valve system Zephyr Zephyr Zephyr Zephyr Zephyr Spiration Spiration Pulmonary function test criteria FEV1 < 50%
TLC > 100%
RV > 150%FEV1 < 60%
TLC > 100% RV > 150%FEV1 <
15-45%
TLC > 100%
RV > 200%FEV1 < 15-45%
TLC > 100%
RV > 180%FEV1 < 15-45%
TLC > 100%
RV > 150%
DLCO > 20%FEV1 < 45%
TLC > 100%
RV > 150%FEV1 < 45%
TLC > 100%
RV > 150%Collateral ventilation, fissure integrity assessment High-resolution CT Chartis system Chartis system Chartis system Chartis system High-resolution CT High-resolution CT Clinical outcome, change from baseline FEV1, % of predicted 8.7 20.9 13.7 20.7 17.1 13.5 12.1 6-min walk distance (m) 25 60 22.6 36.2 12.9 27.1 6.9 Reduction in RV (L) 0.26 0.86 0.42 0.66 0.49 0.52 0.36 Quality of life scoree 8.6 17.3 8.6 7.2 7.5 7.6 9.5 Pneumothorax occurrence, % 8.6 17.6 27.9 23 34.3 7.6 12.4 ↵a Defined as a National Emphysema Treatment Trial score of > 2 and a difference of > 1 emphysema score from ipsilateral lobes. Emphysema score ranges from 0-4; 0 represents absence of emphysema, and 1-4 represents quartiles of emphysematous lung involvement. For example, a score of 3 means 50% to 75% involvement with emphysema.
↵b Defined as a < 15% difference in destruction score by quantitative high-resolution computed tomography (CT).
↵c Defined as a > 10% difference in destruction score by quantitative high-resolution computed tomography.
↵d Defined as a > 15% difference in destruction score by quantitative high-resolution computed tomography.
↵e St. George Respiratory Questionnaire score.
DLCO = diffusing capacity for carbon monoxide; FEV1 = forced expiratory volume in 1 second; RV = residual volume; TLC = total lung capacity
Severe airflow obstruction:
FEV1 between 15% and 45% of predictedSevere air trapping and hyperinflation:
TLC > 100% and RV > 175% of predictedSevere emphysematous destruction in target lobe:
> 50% involvementAbsence of collateral ventilation between target lobe and neighboring lobe or lobes Adequate gas exchange:
diffusion capacity > 20% of predicted, PaCO2 < 50 mm Hg, PaO2 > 45 mm Hg at baselineNo history of frequent severe exacerbations:
> 2 hospitalizations over the past yearAbsence of clinically significant sputum production: “significant” production, > 4 tablespoons per day No significant comorbidities:
eg, cor pulmonale, ejection fraction < 45%, recent myocardial infarctionNo prior lung volume reduction surgery, lobectomy, lung transplant FEV1 = forced expiratory volume in 1 second; PaCO2 = partial arterial pressure of carbon dioxide; PaO2 = partial arterial pressure of oxygen; RV = residual volume;
TLC = total lung capacity
Adapted from reference 23.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.