


Article Figures & Data
Figures
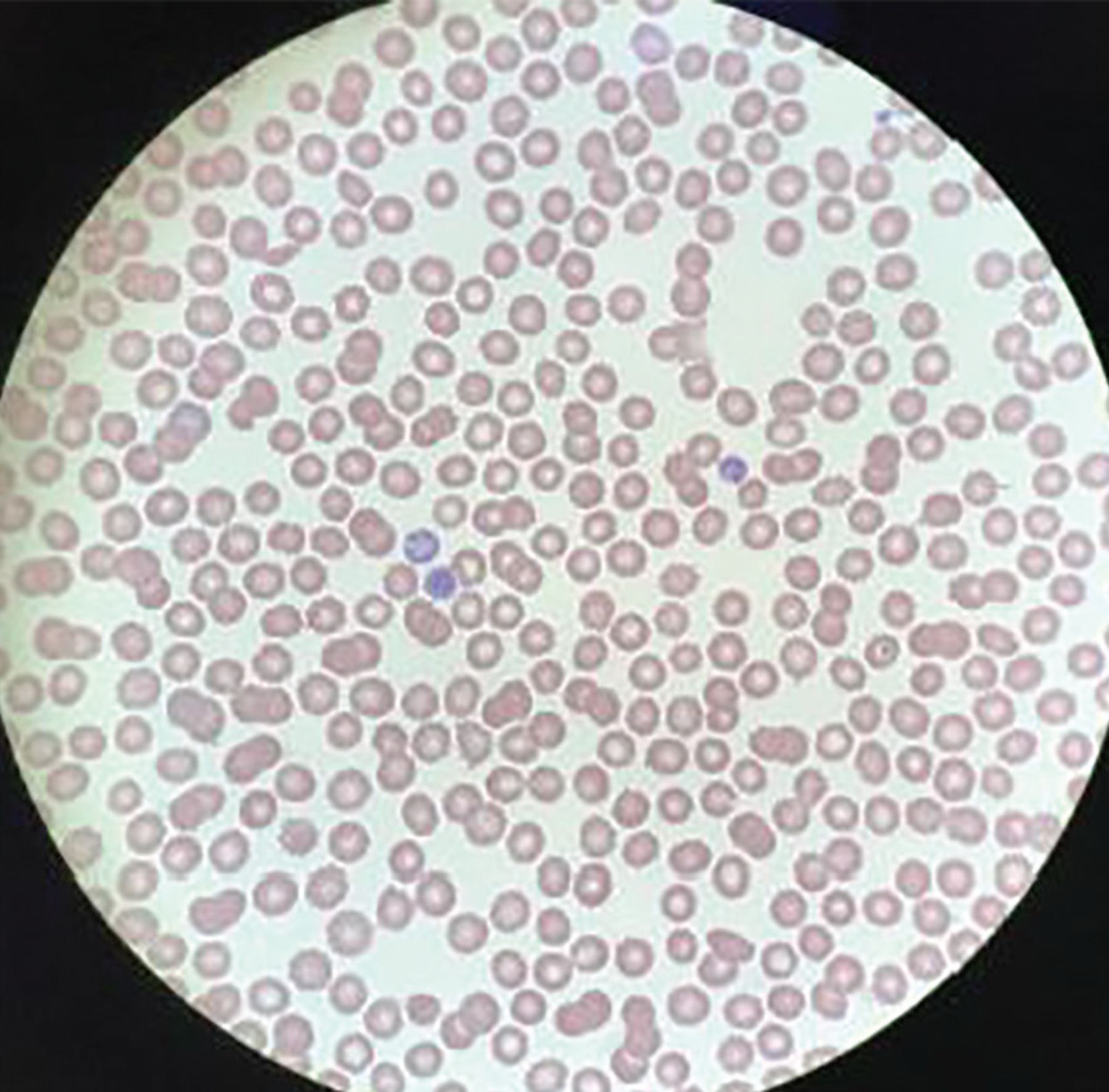
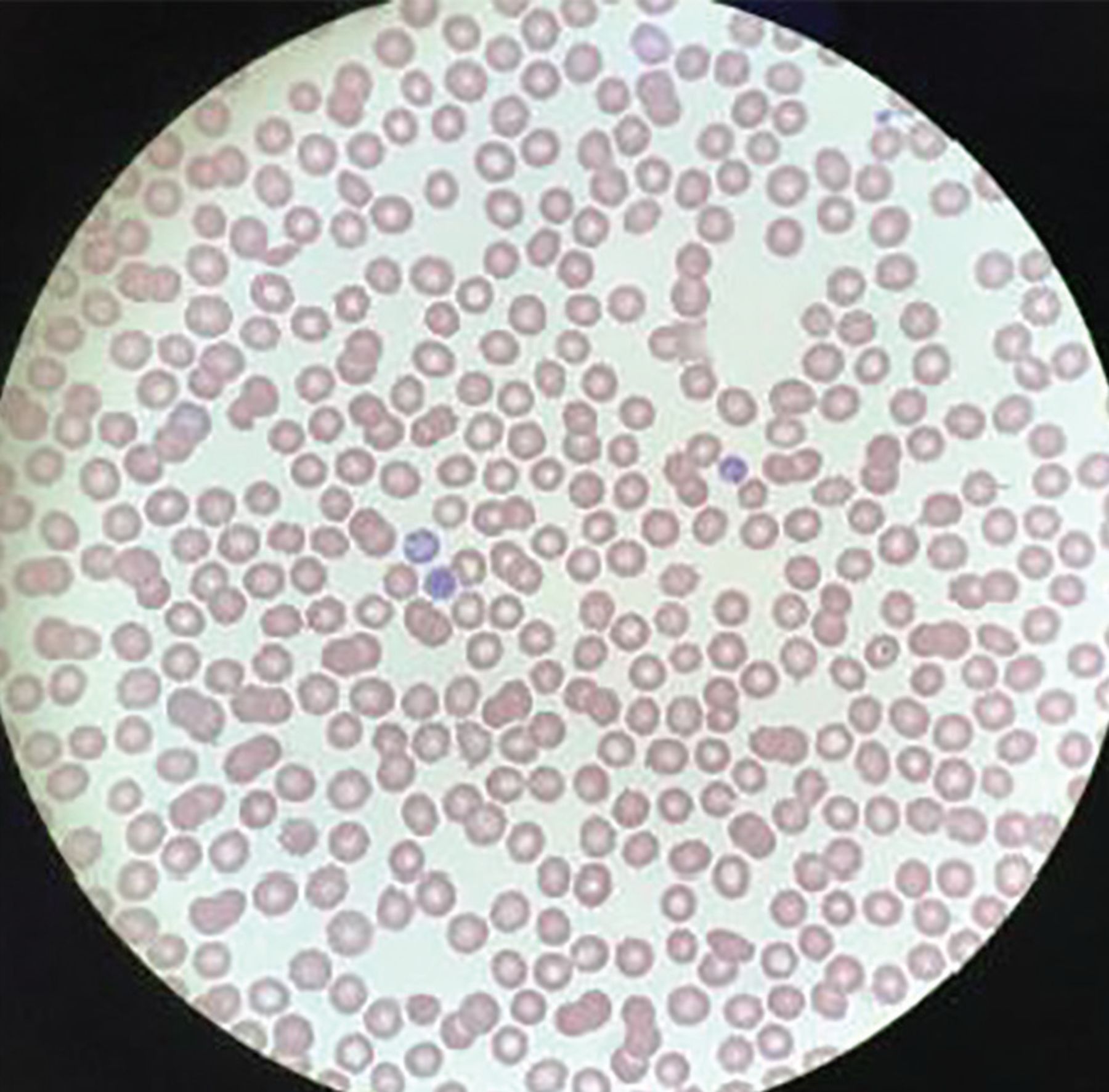
- Figure 1
On the patient’s peripheral blood smear, no platelets were visible.
Tables
Test Patient’s valuea Reference range White blood cell count 7.03 × 109/L 3.7–11.0 Red blood cell count 4.46 × 1012/L 3.90–5.20 Hemoglobin 14.4 g/dL 11.5–15.5 Hematocrit 41.2% 36%–46% Platelet count 3.0 × 109/L 150–400 Mean corpuscular volume 92.4 fL 80–100 Mean corpuscular hemoglobin 32.3 pG 26.0–34.0 Mean corpuscular hemoglobin 35.0 g/dL 30.5–36.0 concentration Mean platelet volume 11.7 fL 9.0–12.7 Red cell distribution width 11.9% 11.5%–15.0% coefficient of variance Reticulocytes 84 × 109/L 18–100 1.9% 0.4%–2.0% Neutrophils 4.59 × 109/L 1.45–7.50 65.3% 55%–70% Lymphocytes 1.77 × 109/L 1.00–4.00 25.2% 20%–40% Monocytes 0.57 × 109/L < 0.87 8.1% 2%–8% Eosinophils 0.09 × 109/L < 0.46 1.3% 1%–4% Basophils < 0.03 × 109/L < 0.11 0.1% 0.5%–1% Nucleated red blood cells < 0.01 × 109/L < 0.01 0% 0% ↵a Abnormal results are shown in bold.
Disease Thrombocytopenia Hemolysisa ADAMTS13 PT/PTT Fibrinogen D-dimer Thrombotic thrombocytopenic purpura Yes Yes Low Normal Normal Normal Hemolytic uremic syndrome Yes Yes Normal Normal Normal Normal Disseminated intravascular coagulation Yes Yes Normal Prolonged Low High Immune thrombocytopenic purpura Yes No Normal Normal Normal Normal ↵a Anemia, increased lactate dehydrogenase, decreased haptoglobin, increased reticulocyte count, increased unconjugated bilirubin.
ADAMTS13 = a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13; PT/PTT = prothrombin time and partial thromboplastin time
Test Patient’s valuea Reference range Sodium 141 mmol/L 136–144 Potassium 3.5 mmol/L 3.7–5.1 Chloride 105 mmol/L 97–105 Carbon dioxide 25 mmol/L 22–30 Blood urea nitrogen 8 mg/dL 7–21 Creatinine 0.97 mg/dL 0.58–0.96 Glucose 69 mg/dL 74–99 Total protein 6.9 g/dL 6.3–8.0 Calcium 9.4 mg/dL 8.5–10.2 Total bilirubin 4.1 g/dL 3.9–4.9 Conjugated bilirubin 0.3 mg/dL 0.2–1.3 Alkaline phosphatase 56 U/L 34–123 Alanine aminotransferase 22 U/L 7–38 Aspartate aminotransferase 19 U/L 13–35 Anion gap 11 mmol/L 9–18 ↵a Abnormal results are shown in bold.
Test Patient’s valuea Reference range Immunoglobulin G 1,120 g/L 717–1,411 Immunoglobulin A 279 g/L 78–391 Immunoglobulin M 123 g/L 53–334 Ferritin 159 ng/mL 14.7–205.1 Interleukin 6 < 2.2 pg/mL < 6.0 C-creative protein 0.1 mg/L < 0.9 Creatine kinase 122 U/L 42–196 Troponin T < 0.010 ng/mL 0.000–0.029 D-dimer 790 μg/mL < 500 Fibrinogen 440 mg/dL 200–400 International normalized ratio 1.3 0.9–1.3 Prothrombin time 10.3 s 9.7–13.0 Partial thromboplastin time 25.4 s 23.0–32.4 Haptoglobin 180 mg/dL 81–238 Lactate dehydrogenase 304 U/L 135–214 Coombs Negative Negative Hepatitis B surface antigen Negative Negative Hepatitis B surface antibody Positive Negative Hepatitis B core antibody, total Negative Negative Hepatitis C antibody 1A Negative Negative HIV1/2 antibodies Negative Negative Syphilis Nonreactive Nonreactive ↵a Abnormal results are shown in bold.
Case Presenting symptoms COVID symptoms present before or on admission? Hospital day of decrease in platelet count Initial platelet count (× 109/L) First ITP intervention Platelet count after first ITP intervention (× 109/L) Second ITP intervention (if applicable) Platelet count after second ITP intervention (×109/L) Hindilerdin et al22 Easy bruising, fatigue, fever, dry cough Yes Day 0 10 IVIG 1 g/kg × 2 days 25 Prednisolone 1 mg/kg/day × 10 days 100 Tsao et al23 Rash, purple lesions in mouth, bruising Yes Day 0 5 IVIG 1 g/kg once 320 N/A N/A Artru et al24 Dyspnea, fever, cough, asthenia Yes Day 4 1 IVIG 0.4 g/kg × 5 days Dexamethasone 40 mg/day × 4 days 30 Dexamethasone 40 mg/day × 4 days 75 Bennett et al25 Fever, dyspnea, diarrhea, cough Yes Day 0 < 3 IVIG 1g/kg × 2 days 105 N/A N/A Levesque et al26 Dyspnea, dry cough, fever Yes Day 20 23 IVIG 1 g/kg × 2 days Dexamethasone 40 mg × 4 days < 10 Romiplostim daily × 10 days Vincristine × 1 day Methylprednisolone 500 mg IV × 4 days 178 Murt et al27 Petechiae, easy bruising Yes Day 0 9 IVIG 2 g/kg × 2 days 54 N/A N/A Bomhof et al28 Patient 1 Oral mucosal petechiae, spontaneous skin hematomas Yes Day 0 < 3 Platelet transfusion IVIG 1 g/kg × 2 days 47 Dexamethasone 51 Patient 2 Petechiae, bleeding from hemorrhoids, epistaxis Yes Day 0 2 Platelet transfusion Dexamethasone 40 mg daily × 4 days 2 IVIG 32 Patient 3 Fever, coughing, dyspnea Yes Day 12 3 N/A N/A N/A N/A Granat et al (current case) None N/A 0 3 Platelet transfusion Dexamethasone 40 mg × 1 day 67 Prednisone 1 mg/kg × 4 days 268 ITP = immune thrombocytopenic purpura; IVIG = intravenous immunoglobulin; N/A = not available
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.