


Article Figures & Data
Figures
- Figure 1
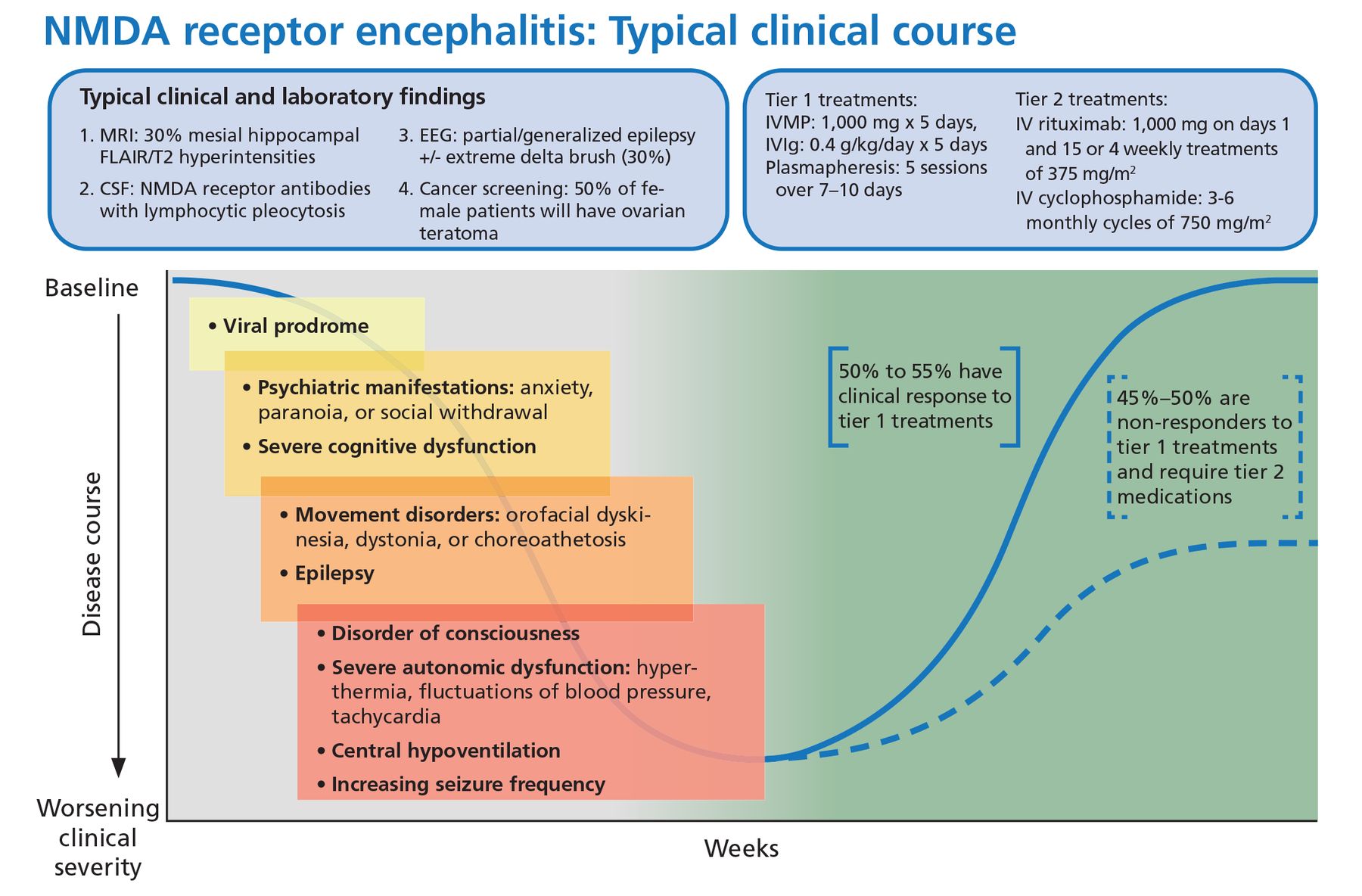
Typical clinical course associated with anti-NMDA receptor encephalitis.
CSF = cerebrospinal fluid; EEG = electroencephalography; FLAIR = fluid-attenuated inversion recovery; IV = intravenous; IVIg = intravenous immunoglobulin; IVMP = intravenous methylprednisolone; MRI = magnetic resonance imaging; NMDA = anti-N-methyl-D-aspartate receptor
Based on information in reference 15.
- Figure 2
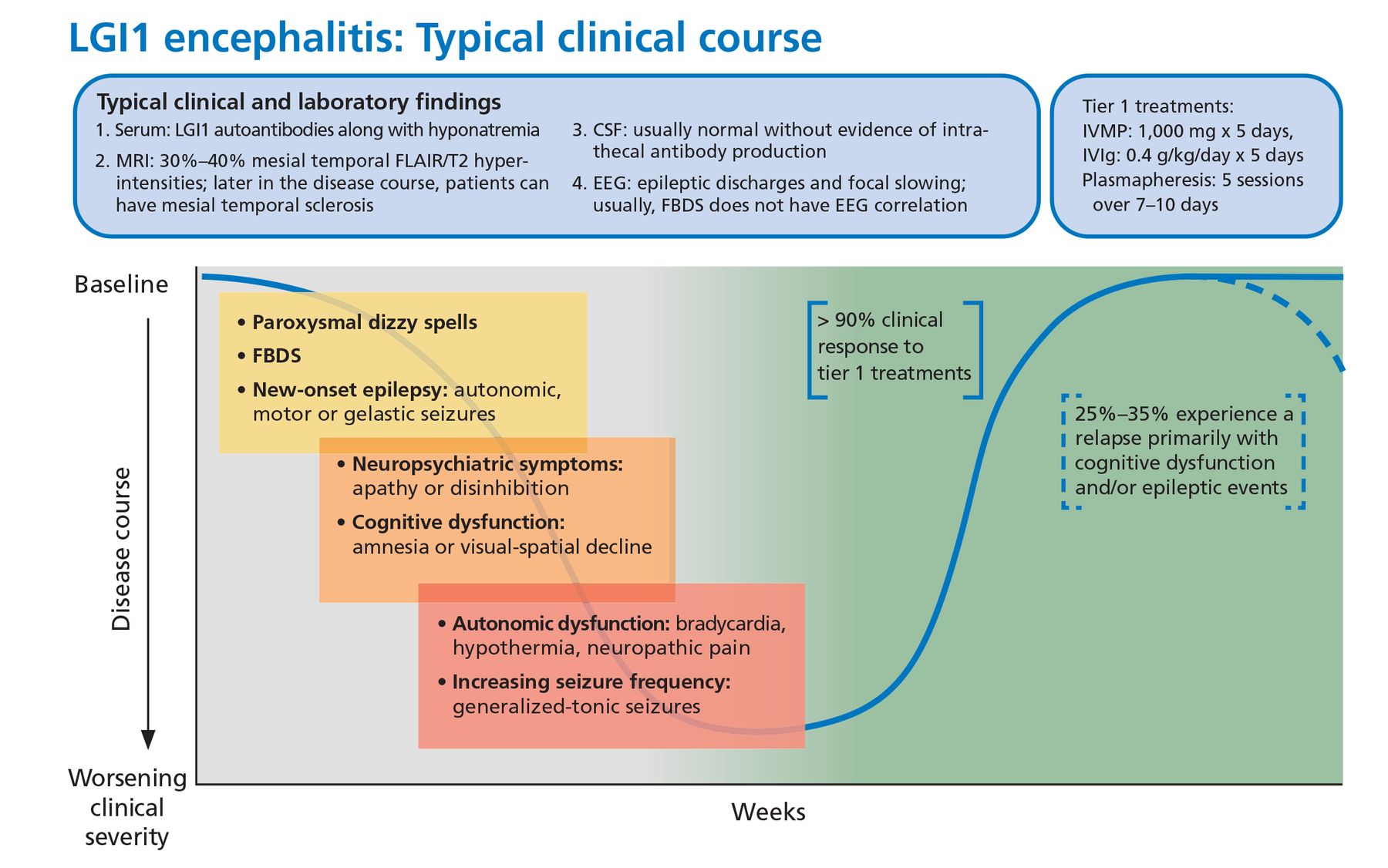
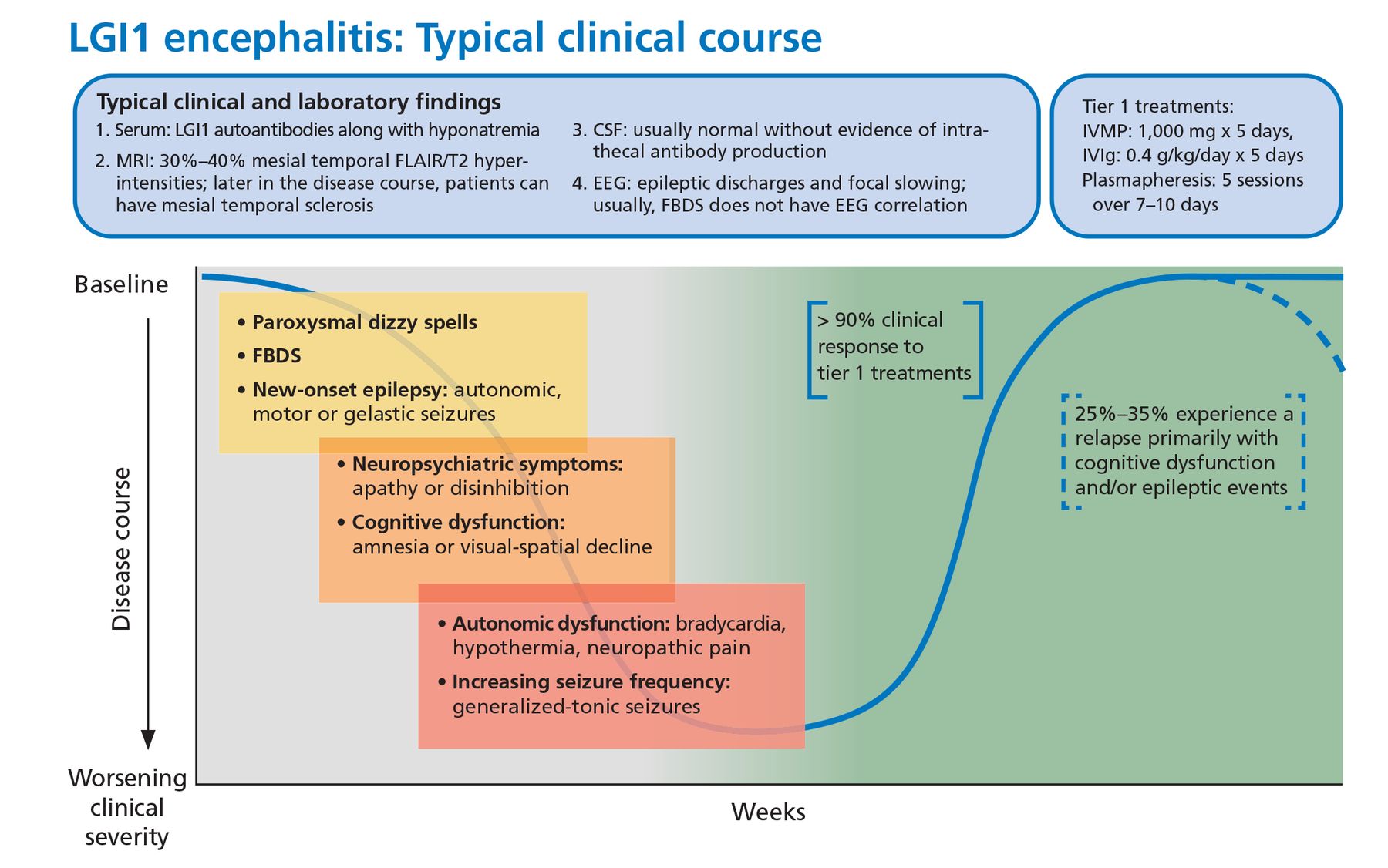
Typical clinical course associated with anti-LGI1 encephalitis.
CSF = cerebrospinal fluid; EEG = electroencephalography; FBDS = faciobrachial dystonic seizures; FLAIR = fluid-attenuated inversion recovery; IVIg = intravenous immunoglobulin; IVMP = intravenous methylprednisolone; LGI1 = leucine-rich glioma-inactivated 1; MRI = magnetic resonance imaging

Tables
ANTIBODY TARGET CENTRAL NERVOUS SYSTEM FEATURES PERIPHERAL NERVOUS SYSTEM FEATURES OTHER ASSOCIATED MALIGNANCY High-risk paraneoplastic autoantibodies ANNA-1 (Hu) Limbic encephalitis
Encephalomyelitis
Cerebellar ataxiaSensory neuropathy Gastrointestinal dysmotility SCLC Rare: neuroblastoma ANNA-2 (Ri) Encephalomyelitis
Cerebellar ataxia
RhombencephalitisJaw dystonia Laryngospasm SCLC Breast carcinoma ANNA-3 Limbic encephalitis
Encephalomyelitis
Cerebellar degenerationSensory and sensorimotor neuropathies SCLC Amphiphysin Stiff-person spectrum
disorderSCLC Breast or ovarian carcinoma CRMP-5 Limbic encephalitis
Cerebellar ataxia
Chorea
Myelopathy
Cranial neuropathies
(optic neuritis)Polyradiculoneuropathy SCLC Thymoma carcinoma GAD65 Stiff-person spectrum
disorder
Limbic encephalitis
Cerebellar ataxiaRare GFAP Meningoencephalitis
Myelitis
Optic neuritisOvarian teratoma Adenocarcinomas of various sites PCA-1 (Yo) Cerebellar ataxia Breast or ovarian carcinoma PCA-2 Limbic encephalitis
Cerebellar ataxiaPolyneuropathy SCLC PCA-Tr (DNER) Limbic encephalitis
Cerebellar ataxiaHodgkin lymphoma Ma 1 and Diencephalitis Ma1: Common, diverse Ma 2 (Ta) Limbic encephalitis
Brain stem encephalitis
Cerebellar degenerationMa2: Testicular seminoma ANNA = antineuronal nuclear antibody; CRMP-5 = collapsin response mediator protein 5; DNER = delta/notch-like epidermal growth factor-related receptor; GAD = glutamic acid decarboxylase; GFAP = glial fibrillary acidic protein; PCA = Purkinje cell cytoplasmic antibody; SCLC = small-cell lung cancer
- TABLE 2
Autoantibody biomarkers of autoimmune encephalitis: Cell-surface and synaptic antibodies
ANTIBODY CENTRAL NERVOUS SYSTEM FEATURES PERIPHERAL NERVOUS SYSTEM FEATURES OTHER FEATURES ASSOCIATED MALIGNANCY AMPAR Limbic encephalitis SCLC Breast carcinoma Thymoma Caspr2 Limbic encephalitis Peripheral nerve hyperexcitability Rare, but thymoma carcinoma reported DPPX Encephalopathy Myelopathy GI dysmotility Sleep disorder Rare, but lymphoma reported D2R Parkinsonism
EncephalitisGABA A receptor Encephalitis
Status epilepticusThymoma GABA B receptor Limbic encephalitis
Status epilepticus
Opsoclonus myoclonusSCLC GQ1b Bickerstaff brain stem encephalitis Guillain-Barré-like illness IgLON5 Sleep disorder
DementiaDysphagia Respiratory failure Rare LGI1 Limbic encephalitis
Faciobrachial dystonic seizuresThymoma NMDA-R Limbic encephalitis
Status epilepticus
Movement disorders
Psychosis
CatatoniaOvarian teratoma mGluR1
mGluR5
Glycine receptorCerebellar ataxia
Limbic encephalitis
Stiff-person spectrum disorderDysgeusia Hodgkin lymphoma
Hodgkin lymphoma
RareAMPAR = 2-amino-3-(5-methyl-3-oxo-1,2-oxazol-4-yl) propanoic acid receptor; Caspr2 = contactin-associated protein-like 2; D2R = dopamine 2 receptor; DPPX = dipeptidyl-peptidase-like protein 6; GABA = gamma-aminobutyric acid; GI = gastrointestinal; LGI1 = leucine-rich glioma-inactivated 1; mGluR = metabotropic glutamate receptor; NMDA-R = anti-N-methyl-D-aspartate receptor; SCLC = small cell lung cancer
FINDINGS COMMENTS Subacute clinical course 1–3 months of symptoms Viral-like prodrome Fever, malaise, headache, gastrointestinal symptoms, etc Neurocognitive deficits Agitation, apathy, catatonia, delusions, irritability, mania, psychosis, and paranoia Neurologic examination abnormalities Ataxia, brain stem abnormalities, myoclonus, tremor, or myelopathy New-onset focal seizure disorder or status epilepticus Often not responsive to antiepileptic medications New focal electroencephalogram abnormalities Focal epileptic or slow-wave activity particularly arising from the temporal lobes Subacute movement disorder Dyskinesias, dystonia, or choreoathetosis Subacute sleep disturbance Central sleep apnea, central neurogenic hypoventilation, or narcolepsy Subacute autonomic dysfunction Hyperhidrosis, tachyarrhythmias, labile blood pressure, central hypoventilation, gastrointestinal dysmotility, urinary dysfunction Brain MRI abnormalities Bilateral T2-weighted FLAIR hyperintensities in the medial aspect of the temporal lobes, although multifocal changes involving the gray and white matter are also possible Inflammatory cerebrospinal fluid Mild to moderate pleocytosis (white blood cell count 5–100/μL) Previous or current oncologic disorder or risk factors for malignancy such as smoking Increased risk of a paraneoplastic disorder FLAIR = fluid-attenuated inversion recovery; MRI = magnetic resonance imaging
In this issue




{kind=link}
{kind=link}
Jump to section
- Article
- ABSTRACT
- GENERAL FEATURES OF AUTOIMMUNE ENCEPHALITIS
- HOW IS AUTOIMMUNE ENCEPHALITIS CLASSIFIED?
- WHEN SHOULD I CONSIDER THE DIAGNOSIS?
- WHAT ARE THE COMMON CELL-SURFACE/SYNAPTIC ANTIBODY SYNDROMES IN AUTOIMMUNE ENCEPHALITIS?
- WHAT TESTING SHOULD I CONSIDER FOR AE DIAGNOSIS?
- A COMPREHENSIVE EVALUATION FOR AUTOIMMUNE ENCEPHALITIS
- WHICH AUTOANTIBODY FINDINGS SHOULD BE INTERPRETED CAUTIOUSLY?
- WHAT IS THE INITIAL TREATMENT FOR AUTOIMMUNE ENCEPHALITIS?
- HOW DO I MONITOR RESPONSE TO TREATMENT IN AE?
- WHAT ONCOLOGIC EVALUATION IS APPROPRIATE FOR PATIENTS WITH AE?
- TAKE-HOME MESSAGE
- DISCLOSURES
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.