


Article Figures & Data
Figures
- Figure 1
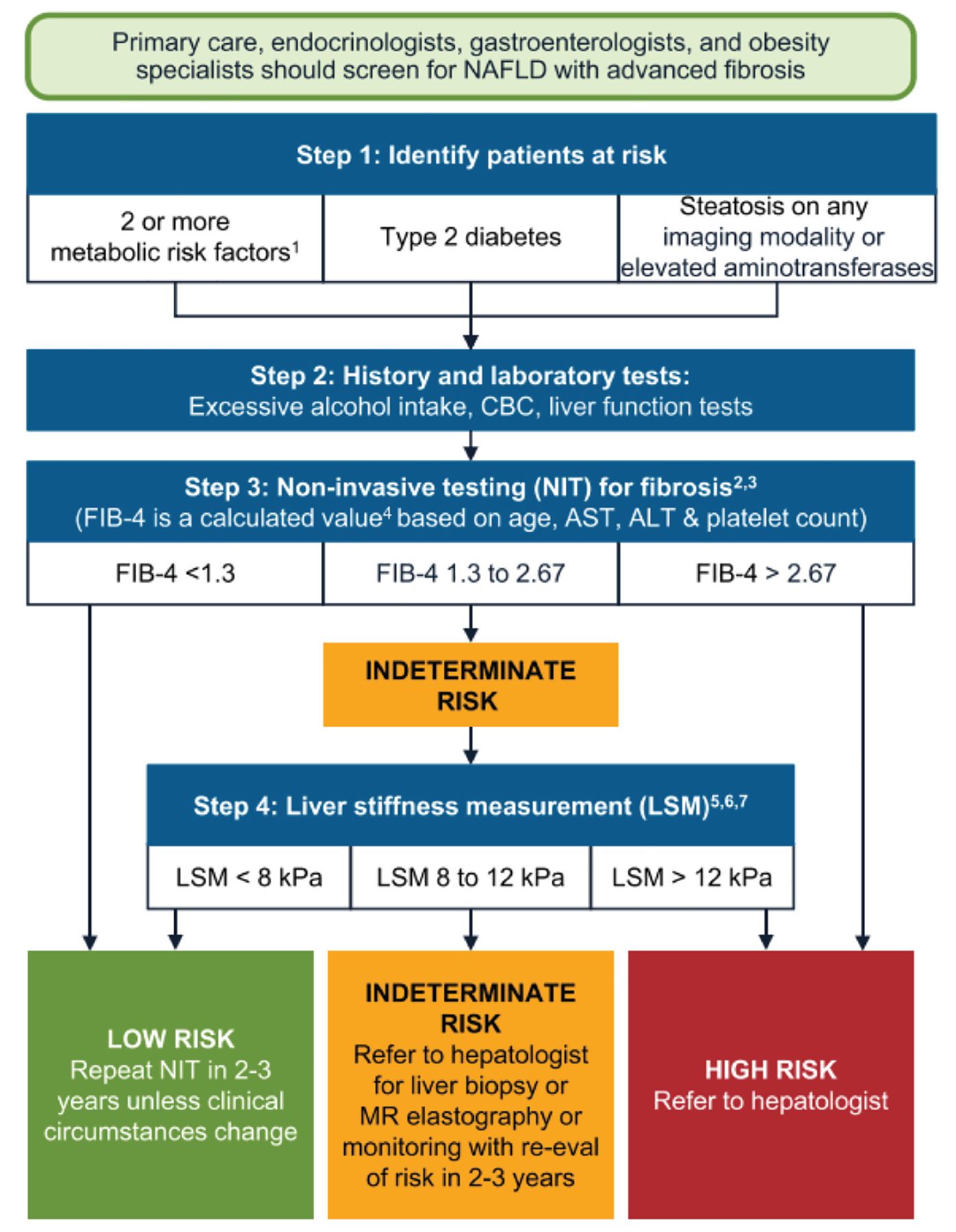
Screening patients for NAFLD with advanced fibrosis.
1Metabolic risk factors: central obesity, high triglycerides, low high-density lipoprotein cholesterol, hypertension, prediabetes, or insulin resistance.
2For patients 65+, use FIB-4 < 2.0 as the lower cutoff. Higher cutoff does not change.
3Other NITs derived from routine laboratories can be used instead of FIB-4.
4Many online FIB-4 calculators are available such as https://www.mdcalc.com/calc/2200/fibrosis-4-fib-4-index-liver-fibrosis.
5Ultrasonography acceptable if vibration-controlled transient elastography (VCTE, FibroScan) is unavailable. Consider referral to hepatologist for patients with hepatic steatosis on ultrasonography who are indeterminate or high risk based on FIB-4.
6LSM values are for VCTE (FibroScan). Other techniques such as bidimensional shear-wave elastography or point shear-wave elastography can also be used to measure LSM. Proprietary commercially available blood NITs may be considered for patients considered indeterminate or high risk based on FIB-4 or APRI (aspartate aminotransferase-to-platelet ratio index), or where LSM is unavailable.
7Eddowes et al (Gastroenterology 2019; 156[6]:1717–1730.) used 8.2 and 12.1 kPa as cutoffs for LSM using VCTE. Validation of simple (rounded) cutoffs reported by Papatheodoridi et al (J Hepatol 2021; 74[5]:1109–1116.).
ALT = alanine aminotransferase; AST = aspartate aminotransferase; CBC = complete blood cell count; MR = magnetic resonance; NAFLD = nonalcoholic fatty liver disease
Reprinted from Gastroenterology, 161(5), Kanwal F, Shubrook JH, Adams LA, et al, Clinical care pathway for the risk stratification and management of patients with nonalcoholic fatty liver disease, 1657–1669, 2021, with permission from Elsevier.
- Figure 2
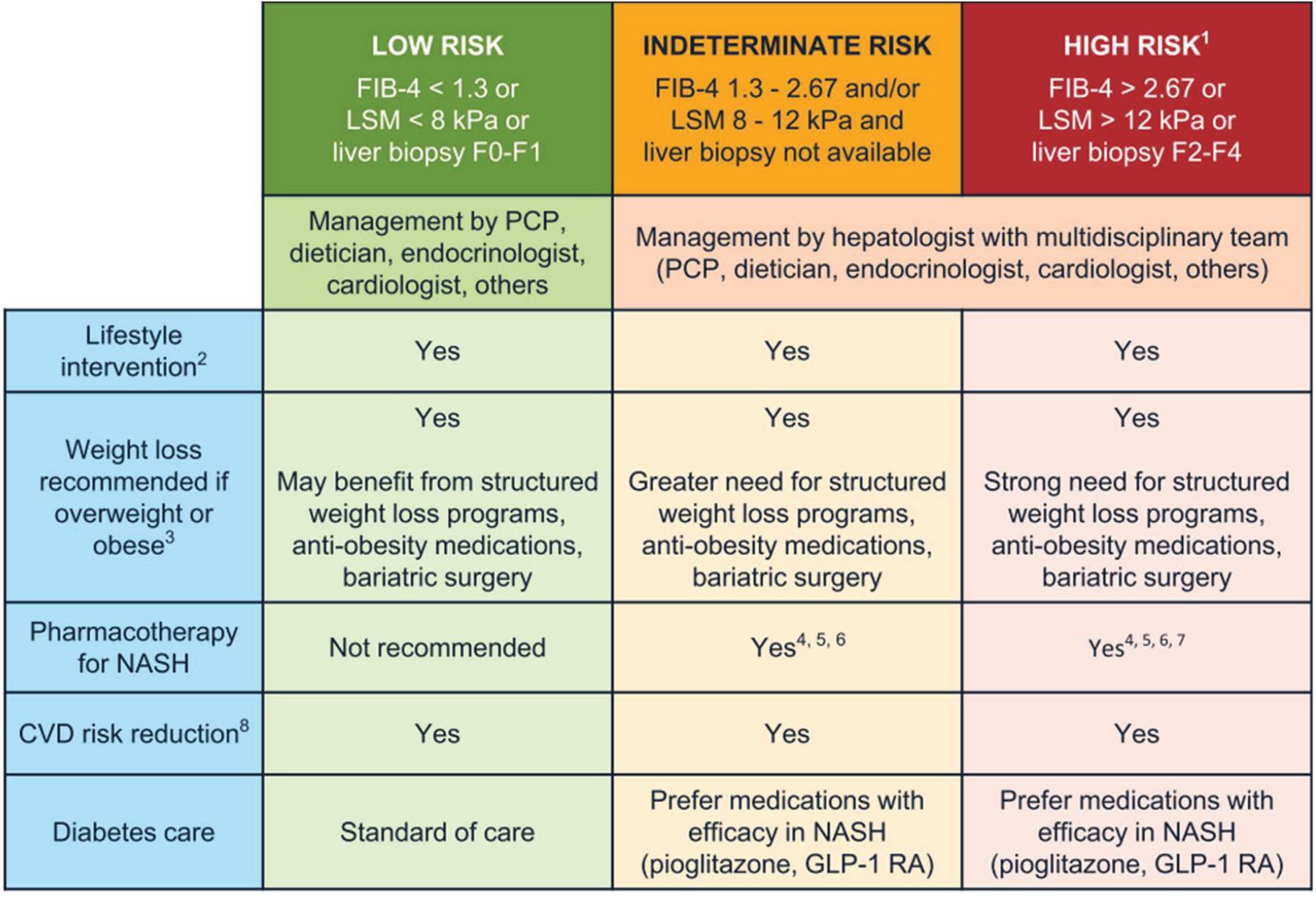
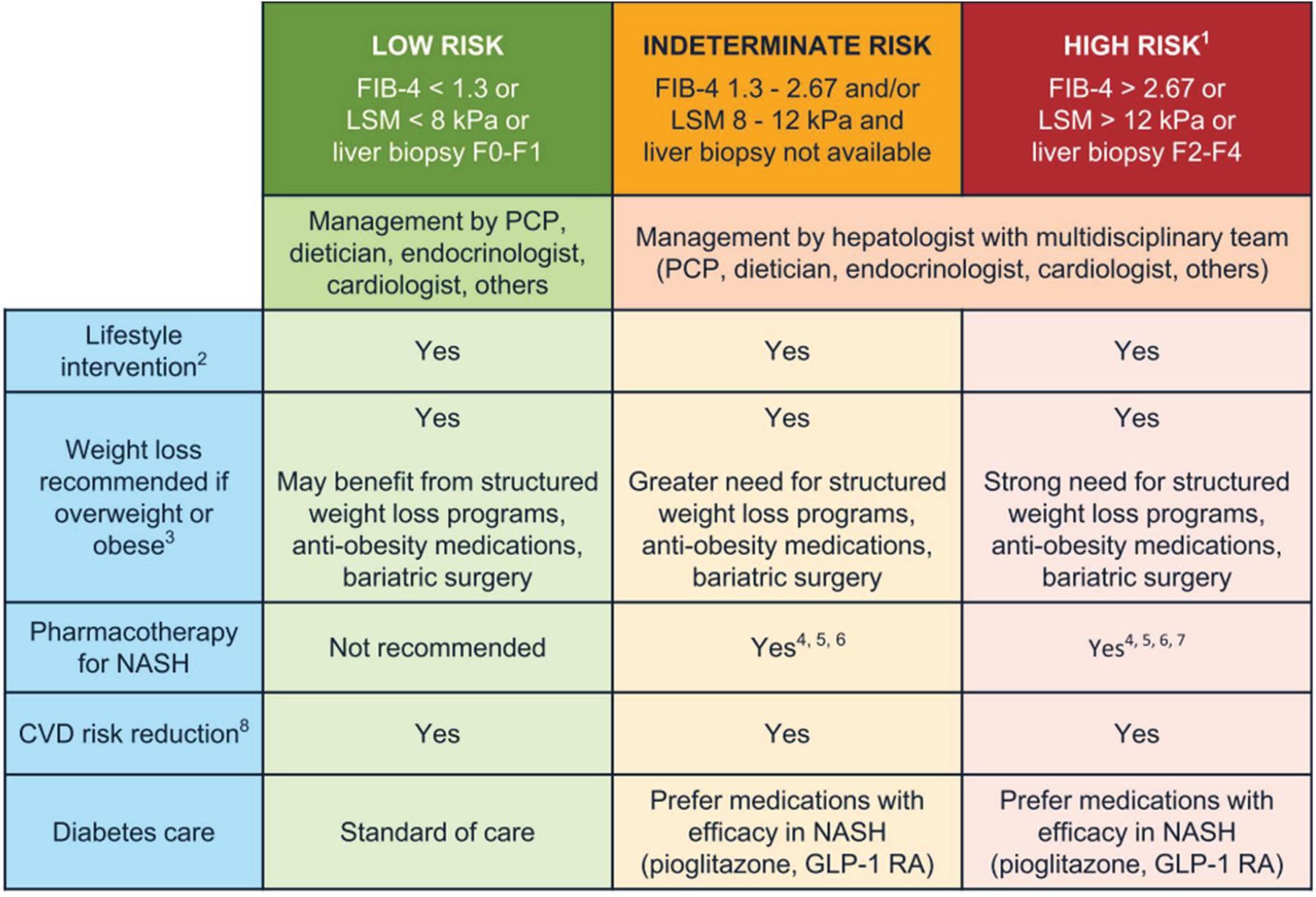
Management of NAFLD and NASH.
1Patients with stage F4 or cirrhosis (based on biopsy, LSM values based on vibration-controlled transient elastography [VCTE, FibroScan] or > 5.0 kPa on MRE) should undergo hepatocellular carcinoma surveillance. Varices screening is recommended if LSM > 20 kPa or platelet count of < 150,000/mm3.
2All patients require regular physical activity, healthy diet, avoid excess alcohol intake.
3Weight loss recommended for cardiometabolic benefit and reversal of steatosis. Greater weight loss is often associated with more benefit, such as reversal of steatohepatitis (usually with weight loss ≥ 7%) or fibrosis (usually with weight loss ≥ 10%).
4Individualize based on further workup and efforts to confirm the diagnosis of NASH. Liver biopsy provides helpful information and should be considered when there is a diagnostic doubt, such as in patients with indeterminate, unreliable, or conflicting noninvasive assessments or as part of phase 2 or 3 clinical trials.
5No pharmacologic agent is FDA-approved for the treatment of NASH. Patients with type 2 diabetes may benefit from some diabetes medications, such as pioglitazone (Sanyal et al, N Engl J Med 2010; 362:1675–1685; Bril et al, Diabetes Care 2019; 42:1481–1488; Aithal et al, Gastroenterology 2008; 135:1176–1184; Cusi et al, Ann Intern Med 2016; 165:305–315; Belfort et al, N Engl J Med 2006; 355:2297–2307) and some GLP-1 RAs (Armstrong et al, Lancet 2016; 387:679–690; Newsome et al, N Engl J Med 2021; 384:1113–1124) that have reported histologic improvement in randomized controlled trials in patients with NASH, either with or without diabetes. Among GLP-1 RAs, semaglutide has the strongest evidence of liver histologic benefit (Newsome et al, N Engl J Med 2021; 384:1113–1124).
6Vitamin E improves steatohepatitis in patients with NASH without diabetes (Sanyal et al, N Engl J Med 2010; 362:1675–1685), with less evidence in patients with type 2 diabetes (Bril et al, Diabetes Care 2019; 42:1481–1488).
7Pharmacotherapy in patients with NASH cirrhosis is very limited and should be avoided until more data become available.
8Statins can be used safely in patients with steatohepatitis and liver fibrosis. Avoid in patients with decompensated cirrhosis.
CVD = cardiovascular disease; FDA = US Food and Drug Administration; GLP-1 RAs = glucagon-like peptide-1 receptor agonists; LSM = liver stiffness measurement; MRE = Magnetic resonance elastography; NASH = nonalcoholic steatohepatitis; PCP = primary care provider
Reprinted from Gastroenterology, 161(5), Kanwal F, Shubrook JH, Adams LA, et al, Clinical care pathway for the risk stratification and management of patients with nonalcoholic fatty liver disease, 1657–1669, 2021, with permission from Elsevier.
Tables
NAFL Early NASH Fibrotic NASH Advanced fibrosis Cirrhosis Fibrosis stage No fibrosis F0–F1 (no or mild fibrosis) ≥ F2 (significant fibrosis) ≥ F3 (advanced fibrosis) F4 Histologic features ≥ 5% steatosis ≥ 5% steatosis and inflammation with hepatocyte injury (ballooning) ≥ 5% steatosis and inflammation with hepatocyte injury ≥ 5% steatosis and inflammation with hepatocyte injury Bridging fibrosis Weight loss needed for improvement, % of total ≥ 5% ≥ 7% ≥ 10% ≥ 10% Not applicablea ↵a Some cases of reversal of F4 cirrhosis were observed with significant weight loss, such as with bariatric surgery.10
NAFL = nonalcoholic fatty liver; NAFLD = nonalcoholic fatty liver disease; NASH = nonalcoholic steatohepatitis
Data from references 7–10.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.