


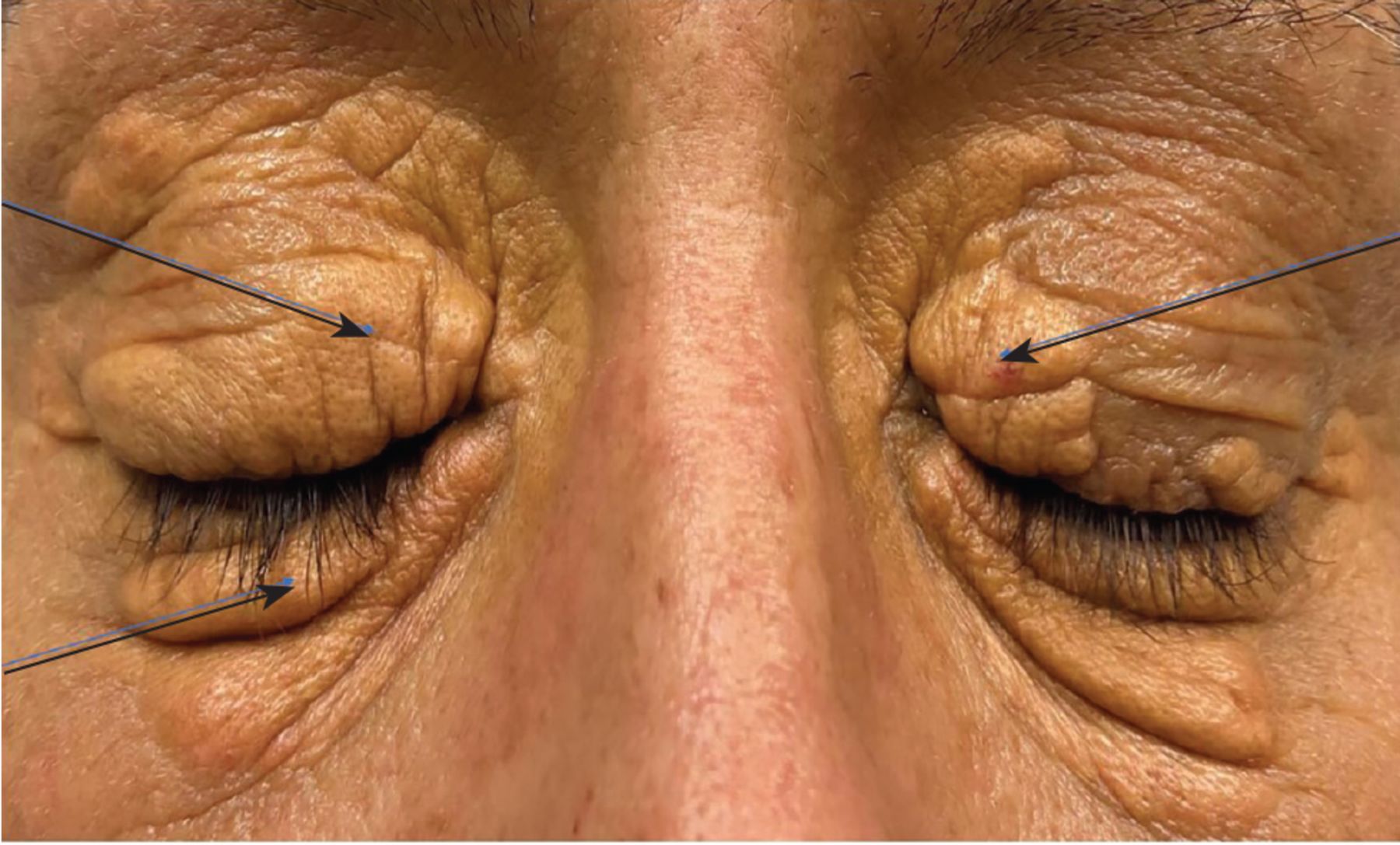
A 42-year-old woman with a known history of primary biliary cholangitis, a chronic progressive cholestatic autoimmune liver disease of uncertain etiology, presented with worsening of generalized pruritus and a gradually increasing number of yellow skin lesions. Physical examination demonstrated raised yellow coalescing plaques around both eyes (Figure 1), similar lesions on the palmar surfaces of the hands (Figure 2), cobblestone-like nodules on the dorsal joints of the hands (Figure 3), and pale pink lesions on the left buttock (Figure 4). She had mild jaundice and scleral icterus.

Coalescing plaques around both eyes (arrows). These plane xanthomas can be seen in the presence or absence of hyperlipidemia.

Xanthoma striatum palmare (arrows) on the palmar surfaces of hands is commonly seen in dysbetalipoproteinemia.

Cobblestone-like nodules (arrows) on the dorsal joints of hands can be seen in underlying hypercholesterolemia.

Pale pink lesions (arrows) on the left buttock representing eruptive xanthoma are seen in hypertriglyceridemia.
Laboratory testing showed the following:
Alanine aminotransferase 265 U/L (reference range 7–55)
Aspartate aminotransferase 191 U/L (8–48)
Alkaline phosphatase 1,109 U/L (40–129)
Total bilirubin 16.8 mg/dL (0.2–1.2)
Unconjugated bilirubin 14.6 mg/dL (0.2–1.2)
Total cholesterol > 585 mg/dL (< 200)
Triglycerides 179 mg/dL (< 150)
High-density lipoprotein cholesterol 31 mg/dL (> 60)
Low-density lipoprotein (LDL) cholesterol > 400 mg/dL (< 100).
Albumin, protein, and renal function panel results were within normal limits.
Based on the presentation and the results of laboratory testing, the lesions were diagnosed as cutaneous xanthomas.
WORKING THROUGH THE DIFFERENTIAL DIAGNOSIS
Cutaneous xanthomas arise from oxidized lipid deposits in the dermis.1 Xanthoma subtypes include plane (ie, xanthelasma), eruptive, tendinous, tuberous, and verruciform,2 and the morphology gives valuable hints about the underlying disease and whether it is atherogenic or nonatherogenic. For example, plane xanthoma can be seen with or without hyperlipidemia, eruptive xanthoma is seen in hypertriglyceridemia, and tuberous xanthoma in hypercholesterolemia. Tendinous xanthoma is seen in familial hyperlipidemia syndromes with elevated LDL cholesterol or familial defective apolipoprotein B-100. Verruciform xanthoma is not associated with dyslipidemia at all.2
Classically, these dyslipidemias contribute to worrisome cardiovascular complications such as myocardial infarction. However, it appears that the lipid accumulation seen in primary biliary cholangitis is a unique lipid subfraction known as lipoprotein X,3 an abnormal nonatherogenic LDL particle that is not associated with increased risk of cardiovascular disease.
Xanthoma striatum palmare
In our patient, the tendinous xanthomas on the dorsal joints of the hand and the eruptive xanthomas on the buttock would typically point the clinician toward underlying primary dyslipidemia. This is also supported by plane xanthelasmas around the eyes. However, our patient also exhibited xanthoma striatum palmare on the volar aspect of the hand, a rare finding that has been described in primary biliary cholangitis, a secondary dyslipidemia.4 This type of eruption is associated with dysbetalipoproteinemia. The diffuse display of 4 different xanthoma subtypes in a single patient is rare, with only 1 other case reported in the literature.4
Volar skin lesions
The differential diagnosis of a widespread pattern of skin lesions on the palms includes disseminated tophaceous gout, characterized by creamy white lesions consisting of monosodium urate buildup, and typically occurring in the ears, tendons, and bursas. Another condition in the differential for this generalized pattern includes pseudoxanthoma elasticum, which is characterized by elastic fibers in the dermis of flexural skin surfaces, as well as in arterial blood vessels. Lipoid proteinosis, a rare autosomal recessive disorder, also presents with this extensive distribution and appears as wart-like, cobblestone-like lesions mostly seen on mucocutaneous membranes. Our patient’s cobblestone lesions were not compatible with this and were on the dorsum of the hand.
TREATMENT OPTIONS
The definitive treatment for this patient is the same as for primary biliary cholangitis, ie, liver transplant.5 Cholestyramine is the guideline-recommended first-line drug for itching in primary biliary cholangitis,6 but it only relieves the pruritus and does not treat the condition. High-intensity statin therapy is not recommended in this patient, as studies have not indicated increased cardiovascular risk in patients with primary biliary cholangitis,6 but it may be beneficial if the benefits outweigh the risks.
Most evidence has shown that hypercholesterolemia in primary biliary cholangitis does not increase cardiovascular risk without a concomitant metabolic syndrome.7 This is due to the distinctive elevated level of cardioprotective lipoprotein X in primary biliary cholangitis.7
TAKE-HOME MESSAGE
Our patient’s case highlights the importance of differentiating atherogenic from nonatherogenic causes of dyslipidemia. By recognizing that the appearance of xanthomas may help differentiate between the two, we can remember to broaden our differential and appropriately tailor our therapies to treat dyslipidemia correctly.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
Footnotes
This research was supported (in whole or part) by HCA Healthcare and/ or an HCA Healthcare-affiliated entity. The views expressed in this publication represent those of the authors and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
- Copyright © 2022 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
{kind=link}
{kind=link}
{kind=link}