


ABSTRACT
Central sensitization, a pathophysiologic process in which the central nervous system undergoes changes that alter its processing of pain and other sensory stimuli, may be the mechanism underlying various conditions in which patients have unexplained pain and fatigue. Patients frequently misunderstand the cause of their symptoms and pursue unnecessary evaluations and treatments. Clinicians have a pivotal role in decreasing this misunderstanding by providing patient education, which can affect perception, management, functional status, and quality of life.
In central sensitization, the central nervous system undergoes structural, functional, and chemical changes that make it more sensitive to pain and other sensory stimuli.
Central sensitization provides an explanatory framework for various frequently encountered conditions.
Patient education about pain physiology and central sensitization can improve quality of life and functional status, and reduce anxiety and catastrophization.
Cognitive behavior therapy aims to reframe negative thoughts, emotions, and behaviors as positive ones.
When patients have chronic pain or other symptoms that seem out of proportion to anything we can tell is physically wrong with them, we should not assume they are faking it. The central nervous system can undergo changes—structural, functional, and chemical—that make it more sensitive to stimuli, a process called central sensitization.1
The concept has everyday relevance. In 2016, an estimated 20% of Americans had chronic pain that markedly worsened their life and raised their healthcare costs.2 In fact, chronic pain can adversely affect every aspect of a person’s life—physical, emotional, social, and financial.
Many patients with chronic pain pursue lengthy rounds of medical appointments and tests and seek relief through prescription medications, including opioids. Opioid-associated deaths have reached epidemic numbers. In the United States alone, opioid overdoses are estimated to cause 115 deaths every day,3 and in 2020, overdoses of all types of drugs killed more than 93,000 people, an increase of more than 28% from the previous year.4 Although it is impossible to know for certain, we hypothesize that many of these deaths were associated with chronic pain.5
However, it is possible—and imperative— to help shift a patient’s attention away from potentially harmful treatments and toward effective nonpharmacologic methods of pain management. Educating patients about the physiology of their pain has consistently been shown to enhance their ability to understand and manage their symptoms.6–9 We believe that educating patients and families about central sensitization empowers them to better appreciate what is going on in their bodies and helps them identify the best ways to manage their symptoms.
This article aims to enhance clinicians’ knowledge about central sensitization and to help them teach patients and families about its role in chronic symptoms—leading, we hope, to more realistic patient expectations and better outcomes.
THE ROLE OF CENTRAL SENSITIZATION IN CHRONIC PAIN AND OTHER SYMPTOMS
The term central sensitization was coined by Woolf and King10 in 1989 after studies in rats showed that neurons in the spinal cord become hyperexcitable over time after injury. Subsequent studies showed that central sensitization can be maintained with or without continued peripheral input, and that chemical, structural, and functional changes in the central nervous system may ultimately lead to a persistent, heightened state of neural reactivity.11,12
In this pathophysiologic state, the central nervous system is hyperexcited even in the absence of sensory stimuli, and sensory messages are amplified, whether internal or external to the body. This amplification often leads to chronic, widespread, and migratory pain, chronic fatigue, sensory hyperresponsiveness, and many other symptoms. The pain usually is in disparate or incongruent bodily regions, and medical evaluations reveal nothing helpful as to the cause.1,13 The pathophysiologic changes associated with central sensitization are summarized in Table 1.1
Structural, functional, and neurochemical changes associated with central sensitization
The ‘trifecta’ of central sensitization
Overall, these changes create the “trifecta” of central sensitization:
Hyperalgesia, in which a painful stimulus becomes associated with even more pain.
Allodynia, in which a previously nonpainful stimulus now causes pain. Many patients with central sensitization say that a hug or a pat on the back hurts them, clothing irritates their skin, or a heavy blanket exerts painful pressure.
Global sensory hyperresponsiveness, in which the patient is extremely affected by external and internal stimuli. For example, patients with central sensitization may be very sensitive to bright lights, loud noises, smells, foods, and medications, as well as to internal stimuli such as their heartbeat or peristalsis in their gastrointestinal tract.12,14
By asking patients if and how they experience these phenomena, and providing real-life examples, clinicians will be able to identify core features of central sensitization.
Mechanisms of acute vs chronic pain
But how does this all occur?
The enhanced response is in part due to neuroplasticity, ie, the ability of the central nervous system to adapt over time.
In the past, pain processing was thought of as a nebulous, passive relay between noxious stimuli and the parts of the brain responsible for interpreting pain (nociception). This model posited the existence of specific pain pathways, activated only by peripheral painful stimuli, and suggested that the intensity and duration of pain depended solely on these inputs.14 Acute pain therefore was an adaptive, protective function that occurred when a potentially harmful stimulus activated a peripheral nerve, which transported that message to the spinal cord, which carried it to the brain. It alerted an organism to threats and helped it escape from danger and recover from injury.15
Now we know that the process is more complicated. When a peripheral nerve receives a stimulus, the message is reviewed neurochemically. Some neurochemicals amplify the message, whereas others inhibit it. Notably, the inhibiting and amplifying effects originate in the brain, and the modulating messages are sent back down through dedicated neural pathways.16 Usually, the system is well balanced, so that if the brain perceives a stimulus as potentially harmful, the organism will respond to protect itself, whereas nonthreatening stimuli are minimized and do not come to the level of conscious awareness.
The spinal-gate control theory, proposed in 1965 by Melzack and Wall,17 introduced the concept of pain modulation and explained how acute pain differs from chronic pain. In chronic pain, neuroplasticity has primed the nerves to be more sensitive to stimulation, and pain signaling is not just a protective response to noxious stimuli. Rather, pain signals are a consequence of maladaptive changes within the nervous system (neuropathy) and are not necessarily a response to acute nociceptive concerns.
Various neuroplastic factors (including central sensitization, peripheral sensitization, and descending neuromodulation) and risk factors (including genetic variants, medical and psychological comorbidities, medications, and psychosocial factors) may explain why acute pain becomes chronic in some people.18 Although chronic pain previously was believed to arise from nociception or neuropathy, a third category of pain, termed nociplastic pain, has been proposed to describe the increased sensitivity caused by the altered function of sensory pathways.19 With central sensitization, the central nervous system can “change, distort or amplify pain, increasing its degree, duration, and spatial extent in a manner that no longer directly reflects the specific qualities of peripheral noxious stimuli, but rather the particular functional states of circuits in the [central nervous system].”13
Thus, patients with central sensitization may perceive pain from normally nonpainful stimuli (allodynia) and experience greater pain from painful stimuli (hyperalgesia). Affected neurons can have spontaneous autonomous activity, lower thresholds for activation or pain, and wider receptive fields (the pain becomes more diffuse and less definable).20
A patient with central sensitization genuinely feels sensations differently and more intensely than someone without central sensitization. For example, a patient experiencing chronic pain in a well-defined site may observe with time that the pain becomes more diffuse, less defined, and associated with other seemingly unrelated symptoms such as fatigue, headaches, unrefreshing sleep, mood changes, and gastrointestinal concerns. The patient may also relate heightened sensitivities and, as a result, may fear that something new or sinister is happening.
Central sensitization syndrome
What is the role of central sensitization in non−pain-related symptoms? The consensus is that changes that lead to pain origination and amplification similarly lead to many other symptoms.1 Although pain is a primary focus when discussing central sensitization, this condition is complex, with multiple nonpainful symptoms.
The unifying term central sensitization syndrome was proposed by Yunus21 to include overlapping symptoms such as pain, fatigue, sleep disorders, paresthesias, cognitive difficulties, and overlapping conditions such as irritable bowel syndrome, restless leg syndrome, interstitial cystitis, temporomandibular joint disorder, and others. The concept of various coexisting conditions and symptoms all being based on central sensitization has been recognized by the National Institutes of Health with the term chronic overlapping pain conditions.22
These conditions have gained greater attention recently, particularly because they share many features with post-COVID-19 syndrome, including chronic pain and fatigue, postural orthostasis, mood and sleep disturbances, and gastrointestinal symptoms.23 Although additional research is needed to identify the underlying pathophysiologic changes in post-COVID-19 syndrome, we believe that many of the underlying features of central sensitization will be directly applicable.
Other factors that affect an individual’s experience of central sensitization are being explored. These can be protective or pathologic, depending on the circumstances, and they include the autonomic nervous system, endocrine and immune systems, and mechanisms by which the brain responds to neural stimuli. For example, glial cells and neuroinflammation are now known to be key components of the pain experience and are targets of ongoing research.24 Studies have investigated the impact of sleep dysregulation on the development of central sensitization (by means of glial cell activation and neuroinflammatory changes) and the need for sleep hygiene as part of central sensitization-focused therapy.25,26
EDUCATING PATIENTS ABOUT PAIN PHYSIOLOGY
Educating patients about pain physiology and providing them with management strategies helps them reduce the intensity of their symptoms.
Although the field of pain research has seen tremendous advances in recent years, many symptoms and conditions still evade concrete diagnoses and lack effective treatments. As a result, many patients are dissatisfied with their medical care, and they often continue to search for a cure.
Nijs et al8 described how patients who are confused about their pain and believe that they have not received an appropriate diagnosis often assume that their pain indicates that something terrible is happening in their body. Fear of the unknown and excessive efforts to identify the cause can lead patients to have maladaptive perceptions of their symptoms. With this mindset, patients are less able to manage their symptoms, leading to poorer function and an overall lower quality of life. Therefore, successful management of symptoms crucially begins with changing the thought process by educating patients about basic neuroanatomy, physiology, and the role of central sensitization in the nociplastic pain experience.
Sharing information about central sensitization in a way that can be readily understood will increase hope and motivation for those experiencing chronic pain and other long-term symptoms.8 A randomized controlled trial showed that patients who received education about pain physiology worried less about their symptoms and reported better physical function, better mood, more energy, less pain, and overall improved general health perceptions than patients who received generic self-management education.9 Another study showed that neuroscience education in addition to standard nonpharmacologic treatments was associated with reduced pain severity and disability and improved mental and physical function.27
Tailoring learning methods helps build trust
By teaching patients and their families about central sensitization and the differences between acute peripheral pain and centralized nociplastic pain, clinicians can establish trust and empower patients by helping them understand what is happening in their bodies. And trust and empowerment help patients change how they approach and experience pain.
No single educational method is suitable for all patients. Principles of adult learning should be considered, and participants should be offered various options. Face-to-face education combined with written materials offers an ideal learning experience with more sustained outcomes than written materials alone.8,9,28 In our practice we use didactic lectures, handouts and other materials, hands-on demonstrations, visual aids, videos, Internet resources, discussions, and storytelling. Topics include patient experience, diagnostic criteria, physiology of the central nervous system and autonomic nervous system, the cycle of pain, symptom-focused behavior, stress management, diaphragmatic breathing, and biofeedback.
The technical nature of this content can be overwhelming for the layperson, so after assessing the individual’s readiness to learn, the information should be conveyed in an understandable manner, using plain language. Additionally, researchers are constantly publishing new findings about central sensitization, which clinicians should be aware of and discuss with patients.
Education could occur across the continuum of care, outpatient and inpatient. Continuing patient education is appropriate even in long-term care settings because many residents are living longer with chronic pain and multiple comorbid conditions.
EVIDENCE-BASED NONPHARMACOLOGIC TREATMENT
Evidence-based strategies exist for improving physical function and quality of life. Although the functional status of patients with central sensitization may vary widely, self-management strategies such as stress management, diaphragmatic breathing, relaxation, mindfulness, graded exercise, and cognitive behavior therapy can be implemented. Depending on the patient’s level of impairment, the intervention may be focused and brief, or it may need to be in-depth, interdisciplinary, and rehabilitative.29
A helpful way to begin is by guiding patients through an activity that makes them think about how they got to where they currently are in their pain journey. This activity helps identify triggers that may perpetuate the pain cycle and contribute to other harmful actions, such as symptom-focused behaviors, symptom hypervigilance, activity avoidance, and decreased socialization.
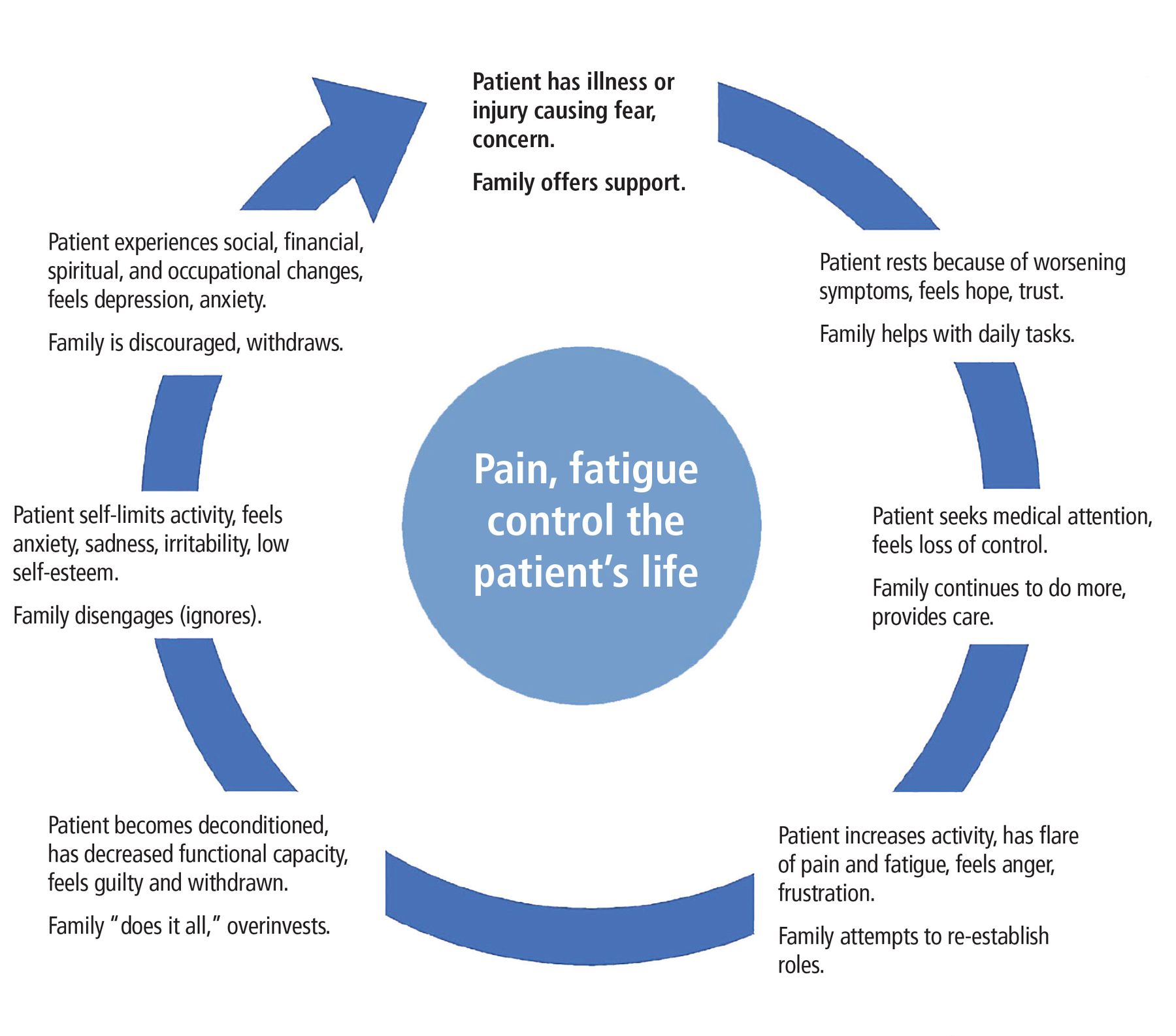
Although each person’s history is different, patients report similar behaviors, emotions, and family responses regarding their chronic symptoms. Figure 1 shows how a patient can get caught in a down ward spiral. Such patients often consider pain to be excessively threatening, have lower pain tolerance, and have hypervigilance with catastrophic thoughts. Family members go through their own cycle.

The cycle of pain and fatigue in central sensitization, showing patient behaviors and emotions and family response.
From Mayo Clinic Patient Education. Managing your Fibromyalgia (MC2593-100). Rochester, MN: Mayo Clinic, 2017, pp. 7 & 32; used with permission of Mayo Foundation for Medical Education and Research, all rights reserved.
Clinicians should seize the opportunity to give hope by educating and empowering patients to take an active rather than passive role in their recovery. Helping patients break free from the cycle of pain and symptom-focused behavior requires them to shift their perspective from an external to an internal locus of control. This change requires education and consistency on the part of the patient. Acceptance of pain and a willingness to engage in self-management have been shown to improve functional outcomes.30,31
To help patients gradually work self-management skills and strategies into their daily lives, it is essential to set goals. For each new strategy, clinicians can help patients write down specific, realistic, and measurable goals. Patients should then write down the specific steps needed to achieve the goals, as they are then more likely to do the work and follow through. Motivational communication skills such as engaging, focusing, and planning can help patients begin the next step of their journey.32
Cognitive behavior therapy and related techniques
Cognitive behavior therapy involves identifying harmful thoughts, emotions, and behaviors and restructuring them into more beneficial ones (Table 2). Patients should know that they can replace maladaptive strategies with more appropriate ones that will help lessen their symptoms.
Central sensitization: Turning negatives into positives
This cognitive restructuring or reframing is done with a trained clinician for a limited time. This approach has been highly successful in helping patients with chronic symptoms improve their overall quality of life and reduce their symptom burden.33–37
Various forms of cognitive behavior therapy are available for specific symptoms such as anxiety, depression, pain, or insomnia. Acceptance and commitment therapy was developed in the mid-1990s as an action-oriented approach that focuses less on controlling or changing negative thoughts and behaviors and concentrates more on helping an individual accept a negative obstacle such as pain or central sensitization and to move past it, despite what they are experiencing.34,36,38 Acceptance in this context is not about resigning oneself to chronic pain. Rather, it is about adapting and learning to respond to symptoms in a healthier manner. Another treatment that can be considered is emotional awareness and expression therapy.39
These approaches can help the patient shift the focus away from symptoms and help build new memory pathways through neuroplasticity.
Stress management
Stress management has a key role in helping patients manage their anxiety and reduce catastrophizing, and it also directly affects physical symptoms by dampening the autonomic stress response.37 Stress-management techniques such as diaphragmatic breathing, relaxation, biofeedback, and mindfulness-based stress reduction can help decrease sympathetic (fight-or-flight) activity.
Mindfulness-based stress reduction promotes neuroplasticity and reduces sympathetic drive. Mindfulness is a skill in which people focus on the present moment, including emotions and physical state, and use meditation, yoga, and focused breathing to lessen symptoms related to central sensitization.40
According to Keefer and Mandal,34 this approach promotes downregulation of pain pathways and also helps improve the emotional experience of pain. Adler-Neal and Zeidan40 reported that cognitive behavior therapy and mindfulness-based stress reduction helped decrease functional connectivity in areas of the brain associated with anticipation, emotional evaluation, and sensory discrimination, resulting in less pain and catastrophizing. Chiesa and Serretti41 showed that the practice of mindfulness reduced pain-related depressive symptoms and stress levels while improving quality of life and increasing pain acceptance.
Graded exercise
Studies have examined the benefits of exercise (flexibility, aerobic, and strengthening) for patients with chronic pain. Ambrose and Golightly42 concluded that exercise not only decreased pain but improved overall physical function, sleep quality, and cognitive function.
Unfortunately, after being told to exercise, many patients get into a cycle of overdoing it on a “better” day, only to have more severe symptoms later. This exercise-induced exacerbation can cause patients to associate pain with exercise, termed a pain memory.43
To prevent this cycle, exercise should be graded: the patient should exercise at a low, tolerable level and then gradually increase the duration and intensity. Nijs et al43 recommend an approach based on goals such as duration, number of repetitions, and distance rather than on pain levels. Table 3 shows an example plan with graded exercise recommendations.44
Examples of graded exercise recommendations for self-management
Initially, some patients with central sensitization find that even small amounts of exercise, movement, or activity provoke symptoms, and this can be extremely frustrating and discouraging. The important point to communicate to patients is that graded exercise, movement, and activity strengthen the body in a sustainable manner over time. Graded exercise helps create new memory pathways in the brain, which will decrease the perception of pain and fear of movement.43
Tips on implementing a treatment strategy
To lessen symptoms and enhance quality of life, patients must be ready to transition from a diagnostic mindset to a rehabilitative one. Thus, before starting any treatment, they should understand their symptoms, previous diagnostic results, the need to avoid unnecessary or repetitive diagnostic evaluations (especially those with low value or diagnostic utility), the process of central sensitization, and the importance of using strategies that target both the central (nociplastic) and peripheral mechanisms of symptoms.1,13,29,45
Pharmacologic treatments can include nonsteroidal anti-inflammatory drugs and topical agents aimed at specific peripheral pain generators, if present, as well as neuromodulators (eg, pregabalin, gabapentin, amitriptyline, nortriptyline, duloxetine, milnacipran) that aim to mitigate several of the neurochemical and functional pathophysiologic changes present in central sensitization.1,13,29 Many patients with central sensitization also have focal sources of pain: for example, a patient with fibromyalgia could also have knee osteoarthritis. Thus, treatment needs to strike a balance between therapies aimed at the central sensitization symptoms and the focal symptoms.
Nonpharmacologic strategies, as described above, are strongly recommended as part of a multimodal rehabilitative approach.1,13,29 By providing ongoing education about pain physiology (through clinical visits, handouts, articles, videos, trusted online resources) and describing the process of central sensitization as the anchoring framework, clinicians will be far better able to achieve patient acceptance and motivation. Additional nonpharmacologic treatments that are helpful in central sensitization include time management, moderation, physical and occupational therapy, massage therapy, acupuncture, graded exercise therapy, and sleep hygiene.29
Our preferred approach is to offer individualized strategies to patients and allow them to determine what will work for them. After the strategies are identified and agreed upon, it is vital to refer patients to the appropriate specialists and to encourage patients to implement these strategies to create new neural pathways. Furthermore, if patients struggle to implement these strategies, they can be encouraged to seek further clinical assistance or an interdisciplinary pain rehabilitation program.
No one-size-fits-all treatment strategy exists for patients with central sensitization. Rather, the lack of a “perfect” strategy highlights the need for bidirectional communication, ongoing patient education, and routine clinical visits.
Clinical visits should initially focus on reviewing the history and diagnostic evaluations, making the appropriate diagnosis, and then transitioning to education about pain physiology and central sensitization. Subsequent visits should focus on implementing a multimodal (pharmacologic and nonpharmacologic) approach, with ongoing visits to ensure treatment compliance and functional improvement.
Clinicians should also attempt to consolidate the care for patients with central sensitization-based conditions or other difficult-to-diagnose (“medically unexplained”) conditions rather than provide frequent referrals to subspecialists for additional investigation, as frequent referrals have limited utility and may lead to greater patient dissatisfaction, higher healthcare costs, and, potentially, patient harm.46
ACHIEVING THOROUGH AND EMPATHIC CARE OF PATIENTS WITH NOCIPLASTIC PAIN
The educational framework of central sensitization, which validates and explains the patient’s experience of pain and other symptoms, is a key factor in the thorough and empathic care of patients with nociplastic pain. Education about their condition is a vital step in the patient’s acceptance of and commitment to evidence-based tools to manage their symptoms. The literature supports teaching patients about the basics of central sensitization and nociplastic pain in conjunction with coaching them to implement nonpharmacologic management strategies that help decrease symptoms and improve overall quality of life. Teaching this content is within the scope of clinical practice and is an essential component of high-quality care.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
Acknowledgment
June Oshiro, PhD, ELS, Mayo Clinic, substantively edited the manuscript. The Scientific Publications staff at Mayo Clinic provided proofreading, administrative, and clerical support.
- Copyright © 2023 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Investigating the influence of experimentally induced central sensitisation on pain prediction error encoding in healthy individuals: a novel virtual reality protocol
- Mechanisms of chronic postsurgical pain
- Impact of chronic pain on numerous long COVID-like symptoms: A large-scale internet-based epidemiological study in Japan
- Can a specific biobehavioral based therapeutic education program lead to changes in pain perception and brain plasticity biomarkers in chronic pain patients? A study protocol for a randomized clinical trial
- Chronic centralized pain syndromes: A rheumatologists perspective