


Article Figures & Data
Figures
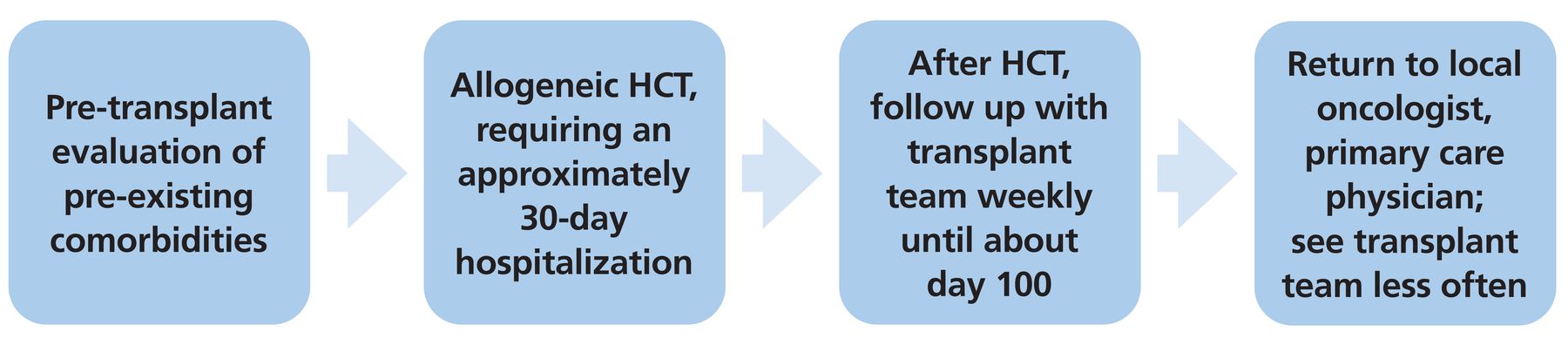
- Figure 1
Typical course of hematopoietic cell transplant (HCT).

Tables
Organs affected Common findings Questions to ask the patient Skin Poikiloderma: erythema
Sclerotic features: thickened skin
Lichen planus-like features: purple polygonal plaques
Lichen sclerosus-like features: wrinkled, atrophic plaques
Morphea-like features: small, red or purple patches with white center
Dryness
Pruritus
Hypopigmentation or hyperpigmentationHave you noticed any changes to your skin? Mouth Lichen planus-like changes: lacy white patches
Xerostomia (dry mouth)
Gingivitis: swelling, redness, bleeding, or pain of the gums
Mouth ulcers
Mucosal atrophy
Mucosal pseudomembranes
Mucoceles: painless mucus-filled cystsDo you have dryness or sensitivity of your mouth? Eyes Dry, gritty, painful eyes
Photophobia
Periorbital hyperpigmentationHave you noticed any changes in your eyes? Liver Jaundice
Total bilirubin, alkaline phosphatase, and alanine aminotransferase levels > 2 times the upper limit of normalGastrointestinal tract Anorexia
Nausea
Vomiting
Diarrhea
Weight loss
DysphagiaDo you have any nausea, appetite changes, changes in bowel habits or appetite, or difficulty swallowing? Lungs Cough
DyspneaDo you have a cough, wheezing, or shortness of breath? Muscles and joints Joint swelling
Joint stiffness
Muscle cramps
Arthralgias
ArthritisDo you have any joint or muscle swelling, stiffness, or pain? Genitalia In women: vaginal dryness, pruritus, dyspareunia, lower urinary tract symptoms
In men: burning, phimosisHave you noticed any urinary or sexual symptoms? Based on information in reference 9.
- TABLE 2
Screening for common adverse effects of corticosteroids in patients with chronic graft-vs-host disease
Adverse effects Screening Metabolic and endocrine Hyperglycemia
Adrenal insufficiency
Weight gainMeasure hemoglobin A1c every 3 months
Monitor complete metabolic panel and blood pressure
Weigh at every visitOrthopedic Osteoporosis
Avascular necrosis
MyopathyObtain dual-energy x-ray absorptiometry scan within first year after hematopoietic cell transplant
Obtain radiograph if symptoms are present
Ask about muscle pain and weaknessNeuropsychiatric Insomnia, mania, psychosis Ask about sleep and psychiatric symptoms Cardiovascular Hypertension
Fluid retentionCheck blood pressure at every visit
Weigh at every visitGastrointestinal Gastritis, peptic ulcer disease Ask about gastrointestinal symptoms Hematologic Leukocytosis Monitor complete blood cell count Dermatologic Acne, hirsutism Perform skin examination at every visit Based on information from reference 10.
Complications Recommendations General Moderate exercise 150 minutes per week
Tobacco cessation counseling
Maintain a healthy weight
Eat a healthy dietDiabetes mellitus Screen with hemoglobin A1c or fasting plasma glucose 3 months after transplant for patients at high risk (on corticosteroids)
Repeat every 6 months if elevatedDyslipidemia Check a fasting lipid panel 3 months after transplant
Repeat evaluation every 3 to 6 months for patients at high risk (on sirolimus, calcineurin inhibitors, or corticosteroids)Hypertension Check blood pressure at every visit at least annually for all patients, regardless of age or other risk factors Based on information in references 11–13.
Vaccine Time posttransplant to initiate vaccination 20-valent pneumococcal conjugate (PCV20) 3 months Tetanus-diphtheria ≥ 6 months Acellular pertussis ≥ 6 months Haemophilus influenzae type B 3 months Meningococcal disease ≥ 6 months Inactivated polio 6–12 months Hepatitis B ≥ 6 months Inactivated influenza ≥ 6 months Measles-mumps-rubella ≥ 24 months Varicella ≥ 24 months Human papillomavirus 6–12 months COVID-19 3 months Based on information in references 21–24.
- TABLE 5
Screening for solid tumors in allogeneic hematopoietic cell transplant recipients vs the general population
General population Allogeneic transplant recipients Risk factors Screening considerations Skin cancers Routine screening not recommended Acute or chronic graft-vs-host disease
Prolonged immunosuppression
Human papillomavirus infection
Total body irradiationAnnual skin self-examination Breast cancer Yearly mammogram beginning at age 45a Same as in general population Head and neck cancer Routine screening not recommended Chronic graft-vs-host disease with prolonged immunosuppression
Reduced-intensity conditioningOral evaluation at 6 months, 1 year, then annually Colorectal cancer Colonoscopy every 10 years beginning at age 45b Abdominal radiation For patients who received radiation: colonoscopy every 5 years beginning at age 35 or 10 years after radiation, whichever occurs last Esophageal cancer Routine screening not recommended Chronic graft-vs-host disease Upper endoscopy if persistent gastroesophageal reflux disease, symptoms of dysphagia Thyroid cancer Routine screening not recommended Neck radiation; chronic graft-vs-host disease Yearly thyroid examination Lung cancer Annual low-dose computed tomography for high-risk cigarette smokers beginning at age 50 c Busulfan and cyclophosphamide-based conditioning
Pretransplant smokingYearly chest imaging, smoking cessation Prostate cancer Discuss prostate-specific antigen screening at age 50 Same as in general population Cervical cancer Papanicolaou smear every 3 years beginning at age 25d Age > 34
Chronic graft-vs-host diseasePapanicolaou smear annually posttransplante ↵a Patients at high risk may require earlier or more frequent screening.
↵b Patients at high risk, including those with inflammatory bowel disease (Crohn disease or ulcerative colitis), family history of colorectal cancer, or a genetic syndrome, may require earlier or more frequent screening.
↵c Current smokers or those who quit within the past 15 years with a 20-pack-year history.
↵d Starting at age 30—cotesting with human papillomavirus every 5 years or Papanicolaou testing alone every 3 years. Discontinue at age 65 if certain criteria are met.
↵e Cotesting preferred, but cytology-only acceptable. If cytology-only is done, if 3 consecutive tests are negative, can increase the interval to every 3 years. If initial cotesting with human papillomavirus is done and negative, can increase interval to every 3 years. Continue past age 65.
Based on information in references 18 and 36–42.
In this issue




{kind=link}
Jump to section
- Article
- ABSTRACT
- PATIENTS ARE LIVING LONGER, FACING LONG-TERM COMPLICATIONS
- HEMATOPOIETIC CELL TRANSPLANT: A BRIEF OVERVIEW
- CHRONIC GRAFT-VS-HOST DISEASE
- CARDIOVASCULAR AND METABOLIC COMPLICATIONS
- ENDOCRINE COMPLICATIONS
- INFECTIOUS COMPLICATIONS
- NEUROLOGIC AND COGNITIVE COMPLICATIONS
- PSYCHIATRIC DISORDERS AND IMPAIRMENTS IN QUALITY OF LIFE
- SEXUAL HEALTH
- SUBSEQUENT MALIGNANCIES
- IT TAKES A PARTNERSHIP
- DISCLOSURES
- REFERENCES
- Figures & Data
- Info & Metrics