


ABSTRACT
Survivors of allogeneic hematopoietic cell transplant (HCT) face the risk of many serious complications in the long term, which primary care physicians play an integral role in recognizing and treating. In this review, the authors summarize the most common complications that primary care physicians see after HCT recipients return to their care: chronic graft-vs-host disease; cardiovascular, metabolic, endocrine, rheumatologic, orthopedic, infectious, neurologic, and cognitive complications; secondary malignancies; psychiatric disorders; and impairments in quality of life and sexual health. Also discussed are health maintenance and screening recommendations for this patient population.
Patients who undergo allogeneic HCT have complex problems, their comorbidities may wax and wane, and their care requires careful coordination between the primary care physician, transplant physician, and primary oncologist.
Primary care physicians should monitor for complications, assisting with the management of the potential sequelae.
Primary care physicians are also important in managing underlying chronic conditions and in routine health screening and maintenance.
Allogeneic hematopoietic cell transplant (HCT) is a potentially curative therapy for many malignant and nonmalignant conditions. The procedure itself is managed by a multi-disciplinary hematology-oncology team, but optimal long-term care of transplant recipients, who can have potentially complex problems, relies on close collaboration with the primary care physician (PCP).
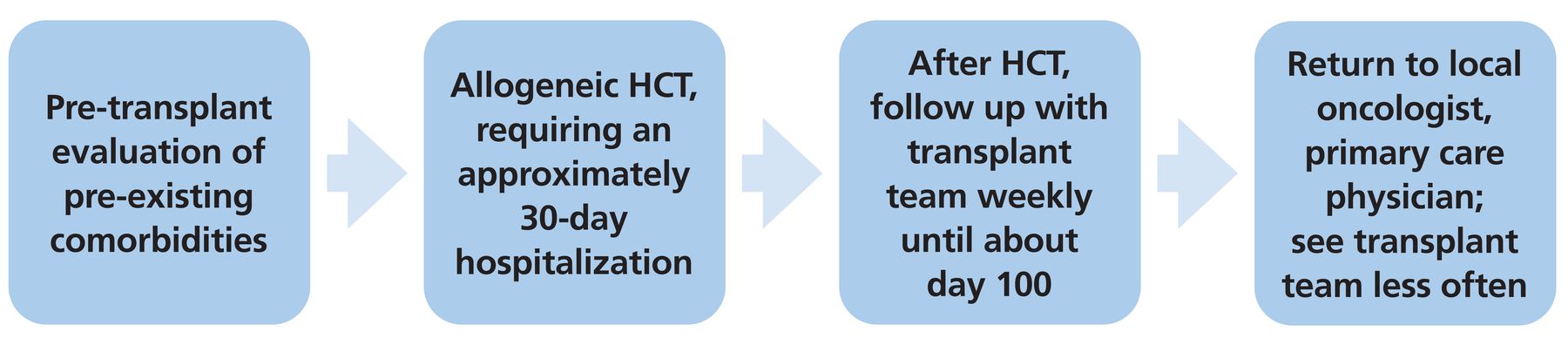
For the first 100 days or so after transplant, patients typically follow up with their transplant providers weekly. Afterward, most patients see their transplant team less frequently, and many return to their referring or primary oncologist and local PCP teams for long-term management (Figure 1), although the posttransplant course can vary from patient to patient and from center to center. In addition, many patients travel long distances to receive their transplant at an academic medical center, and as a result they may be more likely to resume routine care with their local oncologist or PCP before day 100.

Typical course of hematopoietic cell transplant (HCT).
Below, we summarize the most common complications that PCPs may see after HCT recipients return to their care. These include chronic graft-vs-host disease; cardiovascular, metabolic, endocrine, rheumatologic, orthopedic, infectious, neurologic, and cognitive complications; secondary malignancies; psychiatric disorders; and impairments in quality of life and sexual health. We also highlight health maintenance and screening recommendations.
PATIENTS ARE LIVING LONGER, FACING LONG-TERM COMPLICATIONS
Thanks to advances in HCT techniques and technology, including preventing and managing graft-vs-host disease and posttransplant infections, long-term survival rates have increased.1 An analysis of nearly 40,000 allogeneic HCT recipients found that the nonrelapse mortality rate in the first year after the procedure decreased from 24.4% in the 1990s to 9.5% in the years 2013 through 2016.2 But as more patients are living longer, many long-term complications and chronic conditions are becoming more prevalent.
The pathogenesis of post-HCT late effects is likely influenced by several factors. Transplant-specific factors include endothelial injury and DNA damage induced by chemotherapy and radiation; graft-vs-host disease; immunosuppressive treatment and subsequent gonadal and hormonal dysfunction; chronic inflammation; and the new development of cardiovascular risk factors. In addition, defective T-cell immunity may allow oncogenic viruses to reactivate and may also contribute to the development of subsequent malignancies. Patient risk factors such as age, genetic susceptibility, lifestyle, and health behaviors all contribute to the accelerated processes of late effects.
HEMATOPOIETIC CELL TRANSPLANT: A BRIEF OVERVIEW
There are 2 main types of HCT: autologous (in which the patient’s own stem cells are collected before chemotherapy for conditions such as multiple myeloma or lymphoma, and are given back afterward) and allogeneic (in which the patient receives stem cells from a donor). Although both types are associated with late adverse effects, allogeneic HCT recipients are a more complex patient population with a higher risk of late morbidity and mortality related to late effects. This review thus primarily focuses on the complications and care of allogeneic HCT recipients.
Historically, allogeneic HCT was performed to enable patients to receive high doses of myeloablative chemotherapy and radiotherapy to eradicate tumor cells. The transplant was done with the goal of re-establishing normal hematopoietic and immune function, as normal cells were damaged along with the tumor cells by the chemotherapy and radiotherapy. However, we now believe that the donor cells also provide an immune benefit and likely help cure malignant diseases by a graft-vs-tumor effect.2
The most common indications for allogeneic HCT are acute myeloid leukemia, acute lymphoblastic leukemia, lymphomas, myelodysplastic syndrome, and myeloproliferative disorders.2 Once a patient is deemed to be a candidate for allogeneic HCT—a decision that is outside the scope of this article—they are admitted to the hospital for approximately 30 days, during which they receive conditioning chemotherapy and then, on “day 0,” the infusion of allogeneic cells. They are then monitored for engraftment, potential infections, toxicities, and adequate nutrition.
CHRONIC GRAFT-VS-HOST DISEASE
Graft-vs-host disease, which can be acute or chronic, occurs after allogeneic HCT when nonidentical donor immune cells (the graft) attack those of the recipient (the host), causing inflammation, fibrosis, and potential end-organ damage. Chronic graft-vs-host disease occurs in 30% to 50% of allogeneic HCT recipients (the incidence varies with a number of factors and has been increasing over time),3 and apart from relapse, it is the leading cause of late morbidity and death in this group.3,4
The median time from transplant to the onset of chronic graft-vs-host disease is about 5 months, but it can occur at any time.5 The distinction between acute and chronic graft-vs-host disease was previously based on the timing of the onset of symptoms (before or after day 100). However, clinical and pathologic features are now more commonly used to distinguish between the two.6,7 A National Institutes of Health consensus group now recognizes the categories of “classic acute,” “classic chronic,” “de novo late acute,” “recurrent late acute,” “persistent late acute,” and “chronic overlap” graft-vs-host disease.6,7
The most commonly affected organs are the skin, liver, gastrointestinal tract, and lungs, but nearly any organ system can be affected and most patients have organ involvement at the time of diagnosis.8 Common signs and symptoms are listed in Table 1.9
Chronic graft-vs-host disease: Common findings, questions to ask the patient
Chronic graft-vs-host disease requires systemic immunosuppressive therapy for a long time (median of 2 to 3.5 years). Corticosteroids are the mainstay, typically in high doses, eg, prednisone 0.5 to 1 mg/kg/ day or the equivalent.
What PCPs can do: Conduct a thorough physical examination, ask targeted questions about the most common presenting signs of chronic graft-vs-host disease, and order routine laboratory tests such as a comprehensive metabolic panel (Table 1). If there is any suspicion of chronic graft-vs-host disease, the PCP should promptly communicate with the patient’s transplant physician. Early recognition of the signs and symptoms is necessary for prompt treatment and has the potential to halt progression to more severe and morbid phenotypes.
While the transplant physician should manage the treatment of chronic graft-vs-host disease, the PCP should help manage the complications of long-term corticosteroid therapy (Table 2).10 These complications can be recognized by performing routine physical examinations, by monitoring weight, blood glucose levels, electrolytes, and blood pressure, and by inquiring about bone, muscle, gastrointestinal, and psychiatric symptoms.
Screening for common adverse effects of corticosteroids in patients with chronic graft-vs-host disease
CARDIOVASCULAR AND METABOLIC COMPLICATIONS
Allogeneic HCT recipients are at increased risk of long-term cardiovascular complications. Several studies found the risk of cardiovascular death to be 2.3-fold to 3.7-fold higher in HCT recipients than in the general population.11 Armenian et al reported that 10 years after HCT the cumulative incidence of hypertension was 37.7%, diabetes 18.1%, and hyperlipidemia 46.7%.12
Metabolic syndrome, defined by obesity or increased waist circumference, dyslipidemia, hypertension, and hyperglycemia or insulin resistance, develops in as many as 49% of HCT recipients.11 The risk of cardiovascular events and death is significantly higher in patients who meet the criteria for metabolic syndrome than in those who do not.
Additional risk factors for cardiovascular disease in HCT recipients include cumulative exposure to cardiotoxic chemotherapy (eg, anthracyclines), chest radiation before HCT, and decreased cardiac function before HCT.
What PCPs can do: Vigilantly screen for and treat hypertension, diabetes, and hyperlipidemia. Several transplant societies have specific guidelines (Table 3).11–13 Although many of the recommendations are similar to those for the general population, HCT recipients should be screened soon after transplant.
Cardiovascular and metabolic complications after hematopoietic cell transplant
ENDOCRINE COMPLICATIONS
Thyroid dysfunction
Subclinical and overt hypothyroidism are both complications of allogeneic HCT and may be common after radiation to the neck, mediastinum, or total body.
What PCPs can do: Monitor thyroid function annually in all HCT recipients irrespective of risk factors, and repeat testing as needed based on reported symptoms.14
Gonadal failure and infertility
Gonadal failure after allogeneic HCT is common and can be caused by radiation damage to the hypothalamus-pituitary axis, damage to the gonads from chemotherapy or radiation, or both.
In general, the ovaries are more sensitive to radiation and chemotherapy than the testes, and almost all female allogeneic HCT recipients over age 12 who receive myeloablative conditioning develop premature ovarian insufficiency.15,16 Hypogonadism can also lead to dyspareunia and resultant poorer quality of life. Estrogen replacement therapy is often used to treat symptoms of estrogen deficiency, including vasomotor and urogenital symptoms, and can prevent bone loss associated with menopause. Although it may increase the risk of venous thromboembolism, this is rare in patients under age 60.17 It may also increase the risk of endometrial cancer.
Most men have normal testosterone levels after HCT, although many eventually become infertile. Testosterone levels should be measured if the patient develops symptoms such as erectile dysfunction or decreased libido.18 Testosterone replacement therapy can be used to treat symptoms related to testosterone deficiency,17 although it increases the risk of prostate cancer.
What PCPs can do: Assess symptoms of hormone deficiency, discuss replacement therapy and its risks, and, in patients receiving hormone replacement therapy, offer routine screening for complications (eg, prostate-specific antigen testing).
Osteopenia and osteoporosis
Bone loss and subsequent fragility fractures can cause significant long-term morbidity for allogeneic HCT recipients. While fragility fractures may occur later, bone loss can start within the first 6 to 12 months after transplant.19 Around half of HCT recipients develop osteopenia within 4 to 6 years, and the incidence of osteoporosis is approximately 20% after 2 years.20 The 2 most common causes of bone loss after allogeneic HCT are hypogonadism and corticosteroid treatment for graft-vs-host disease.16
What PCPs can do: Because bone loss starts early after transplant, recommend dual-energy x-ray absorptiometry within the first year.
Bisphosphonates are the mainstay of treatment for patients with low bone density and should be considered in patients with established osteopenia or osteoporosis or patients at high risk of bone loss, such as those receiving long-term glucocorticoid therapy for chronic graft-vs-host disease.
Before starting patients on bisphosphonate therapy, vitamin D levels should be measured and patients should receive adequate vitamin D supplementation. Also, because of the risk of jaw osteonecrosis, patients should undergo a dental examination before starting bisphosphonate therapy.
While the optimal duration of treatment has yet to be elucidated, long-term use of bisphosphonates (ie, beyond 5 years) may lead to subtrochanteric fractures.18
Patients should also be advised to engage in regular weight-bearing activity, follow a healthy diet, and avoid tobacco and alcohol.16
INFECTIOUS COMPLICATIONS
Allogeneic HCT recipients are at risk of numerous infectious complications. The type of complication depends on the time from transplant and the engraftment status. Allogeneic HCT recipients lose their immunity posttransplant and must receive all their vaccinations again—ie, vaccinations given during childhood and those given during adulthood. Immunocompetency increases with time from transplant. Typically, patients can safely receive routine vaccinations again between 3 and 12 months posttransplant (Table 4).21–24 Because many patients are still on immunosuppressive therapy or treatment for chronic graft-vs-host disease, it is imperative that they receive routine vaccinations to prevent infection from communicable diseases.
Recommended vaccination schedule after allogeneic hematopoietic cell transplant
Most inactivated vaccines can be given between 3 and 6 months after transplant, whereas live vaccines such as varicella and measles-mumps-rubella must be delayed until 2 years after transplant. COVID-19 vaccinations can be safely given 3 months posttransplant,23 whereas the inactivated influenza vaccine should be given 6 months posttransplant. If there is an influenza outbreak, the influenza vaccine can be given at 4 months posttransplant and a second dose can be considered.22
What PCPs can do: While many patients receive their vaccinations from their transplant physicians, PCPs are also able to vaccinate these patients if necessary. There are many nuances to vaccinating this vulnerable population that are outside the scope of this review, but we suggest communicating with the transplant team or primary oncologist if questions arise.
NEUROLOGIC AND COGNITIVE COMPLICATIONS
Central nervous system complications are common after allogeneic HCT and vary widely in incidence (ranging from 3% to 44%), severity, and etiology.25 These complications can be infectious, metabolic, cerebrovascular, and cognitive.
Cerebrovascular disease
Data indicate a 0.6-fold to 5.6-fold increased risk of cerebrovascular disease in HCT recipients.26 Possible causes include an increased prevalence of risk factors including diabetes, hyperlipidemia, and hypertension; inflammatory changes from chronic graft-vs-host disease; and medication toxicities.26 PCPs must be cognizant of this risk and manage cardiovascular risk factors appropriately (see “Cardiovascular and metabolic complications,” above).
Neurocognitive dysfunction
Neurocognitive dysfunction is the complication most likely to be encountered by PCPs in the outpatient setting. A retrospective study from 2018 found that 35.7% of allogeneic HCT recipients displayed global cognitive dysfunction at 3 years posttransplant.27 Transplant-associated risk factors for cognitive dysfunction include high-dose chemotherapy, total body irradiation, and graft-vs-host disease,25 whereas patient-associated risk factors include older age, male sex, and lower pre-transplant education, income, and cognitive reserve.27 The most common symptoms were loss of verbal recall, loss of fluency, and deficits in executive functions.
What PCPs can do: Transplant physicians do not routinely monitor for neurocognitive dysfunction, so the PCP plays a key role in diagnosis. It is important that PCPs be aware of the risk, assess cognitive function at least annually, and relay concerns to the transplant physician.18
PSYCHIATRIC DISORDERS AND IMPAIRMENTS IN QUALITY OF LIFE
Depression, anxiety, posttraumatic stress disorder, and other impairments in quality of life are common but often underrecognized and undertreated after allogeneic HCT.
Depression and anxiety
A retrospective study found that 15% of allogeneic HCT survivors experienced symptoms of depression and 14% had anxiety.28 These symptoms may increase rather than abate as time passes, as patients must also learn to cope with changes in their domestic roles, employment, and financial situations. In the same study, 81% of survivors reported fatigue that led to a reduction in physical activity, worsened quality of life, and depression.28 Decreased exercise tolerance is also related to decreased quality of life and disability in HCT recipients.29 Chronic graft-vs-host disease and continued immunosuppression are also associated with worse quality of life and depression.28
The Patient Health Questionnaire 2 can be used to screen patients for depression and then, if warranted, the Patient Health Questionnaire 9 can be used to diagnose major depressive disorder.30
Posttraumatic stress disorder
Patients who undergo allogeneic HCT are also at risk for developing posttraumatic stress disorder (PTSD). Patients admitted for allogeneic HCT undergo prolonged and sometimes socially isolating hospitalizations, which can lead to healthcare-associated PTSD.31 Fenech et al32 reported that 39 (18.9%) of 206 HCT recipients had clinically significant symptoms of PTSD at 6 months posttransplant, and risk factors included baseline psychological distress, lack of social support, and reduced physical activity.32 The primary care PTSD criteria of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, known as PC-PTSD-5, can be used for screening.33
What PCPs can do: Assess for psychological symptoms at least annually, and communicate with the transplant physician and mental health professionals if there is concern for the aforementioned disorders.
SEXUAL HEALTH
HCT recipients are at risk of disturbances to their sexual health due to genital chronic graft-vs-host disease, hypogonadism, and other causes.
In women, genital chronic graft-vs-host disease can present as lichen sclerosus-like skin changes or vaginal scarring and stenosis and lead to symptoms such as dryness, burning, dyspareunia, bleeding, abnormal discharge, pruritus, and lower urinary tract symptoms.34 In men, genital chronic graft-vs-host disease may present as lichen sclerosus-like skin changes, phimosis, balanitis, posthitis, erectile dysfunction, burning, or dyspareunia.35
While genital chronic graft-vs-host disease can lead to sexual dysfunction in both men and women, it is also important to consider additional causes such as anxiety, depression, and hypogonadism, as discussed above.
What PCPs can do: Help recognize and diagnose impairments to sexual health. If there is concern for genital chronic graft-vs-host disease or other causes of sexual dysfunction, refer the patient to their transplant physician, gynecologist, or urologist.
SUBSEQUENT MALIGNANCIES
Subsequent malignancies account for 5% to 10% of late deaths in allogeneic HCT recipients and include solid malignancies, hematologic malignancies, and posttransplant lymphoproliferative disorders.36 The most common oncologic complication in HCT recipients is a subsequent solid malignancy. Secondary hematologic malignancies and posttransplant lymphoproliferative disorder occur much less frequently.
Solid malignancies
After allogeneic HCT, recipients are at higher risk of developing solid malignancies than the general population.36 The reported cumulative incidence of solid cancers after allogeneic HCT ranges from 1.2% to 1.6% at 5 years, 2.2% to 6.15% at 10 years, and 3.8% to 14.9% at 15 years.36
What PCPs can do: Screen for cancer (Table 5),18,36–42 and communicate with the transplant physician and primary oncologist if there are questions regarding screening in the setting of specific risk factors. Equally important is to tell transplant recipients to refrain from smoking and drinking alcohol and to routinely wear sunscreen to protect against malignancy.
Screening for solid tumors in allogeneic hematopoietic cell transplant recipients vs the general population
Hematologic malignancies
Hematologic malignancies are the most common indication for allogeneic HCT. Thus, relapsed disease can be challenging to distinguish from a subsequent hematologic malignancy such as acute myeloid leukemia or myelodysplastic syndrome, although reported rates of subsequent hematologic malignancies are generally low.43 Secondary hematologic malignancies are thought to result from oncogenic transformation of normal donor cells in the transplant recipient, as opposed to those after autologous HCT, in which malignancy likely arises from the cryopreserved autograft.44 Symptoms may be consistent with cytopenias and, if present, should be discussed with the oncologic team.
Posttransplant lymphoproliferative disorder
Posttransplant lymphoproliferative disorder is a group of lymphoid disorders, usually B cell in origin, that typically occur in the setting of prolonged immunosuppression after HCT. Extranodal masses are common, and other manifestations may include constitutional symptoms (eg, fevers, chills, weight loss, night sweats), lymphadenopathy, dysfunction of the involved organs, and compression of surrounding structures.44
What PCPs can do: Be aware of this rare yet serious complication and refer patients who may display any new symptoms to their transplant physicians.
IT TAKES A PARTNERSHIP
The care of HCT recipients is complex and requires a partnership between the transplant physician, primary oncologist, and PCP. Understanding and awareness of the various late-onset complications that can arise after allogeneic HCT are extremely valuable, as the PCP is often the first to detect, investigate, and manage them. It is of equal importance that the PCP communicate any concerns with the patient’s transplant physician, primary oncologist, or both.
Although transplant recipients are a special patient population, many of the late-onset complications that they face are within the scope of typical primary care practice. Members of the primary care team, including advanced practice practitioners, nurses, and medical assistants, are often the first to recognize late complications and, owing to their expertise, are also best suited to aid in their management.
There are several known challenges.45–47 A survey of PCPs found that more than half of the respondents reported a gap in knowledge regarding the unique screening and prevention guidelines for HCT survivors.48 Acknowledging this deficit, we hope that this review article serves as a resource for PCPs as they care for this vulnerable population.
In summary, the PCP plays an integral role in screening for and managing chronic coexisting conditions. While the recommendations above are primarily based on consensus, and are not exclusively based on evidence for each specific organ system, PCPs are in a position to help prevent many posttransplant complications. PCPs are uniquely qualified to alter the trajectory of patients after allogeneic HCT, and their importance should not be underestimated.
DISCLOSURES
Dr. Hamilton has disclosed the following: DSMB member with Angiocrine; advisor or review panel participant with Equilium, Incyte, NKarta, and Sanofi; consulting for Incyte; and teaching and speaking for Pfizer and Therakos. The other authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2023 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
Jump to section
- Article
- ABSTRACT
- PATIENTS ARE LIVING LONGER, FACING LONG-TERM COMPLICATIONS
- HEMATOPOIETIC CELL TRANSPLANT: A BRIEF OVERVIEW
- CHRONIC GRAFT-VS-HOST DISEASE
- CARDIOVASCULAR AND METABOLIC COMPLICATIONS
- ENDOCRINE COMPLICATIONS
- INFECTIOUS COMPLICATIONS
- NEUROLOGIC AND COGNITIVE COMPLICATIONS
- PSYCHIATRIC DISORDERS AND IMPAIRMENTS IN QUALITY OF LIFE
- SEXUAL HEALTH
- SUBSEQUENT MALIGNANCIES
- IT TAKES A PARTNERSHIP
- DISCLOSURES
- REFERENCES
- Figures & Data
- Info & Metrics