


Article Figures & Data
Figures
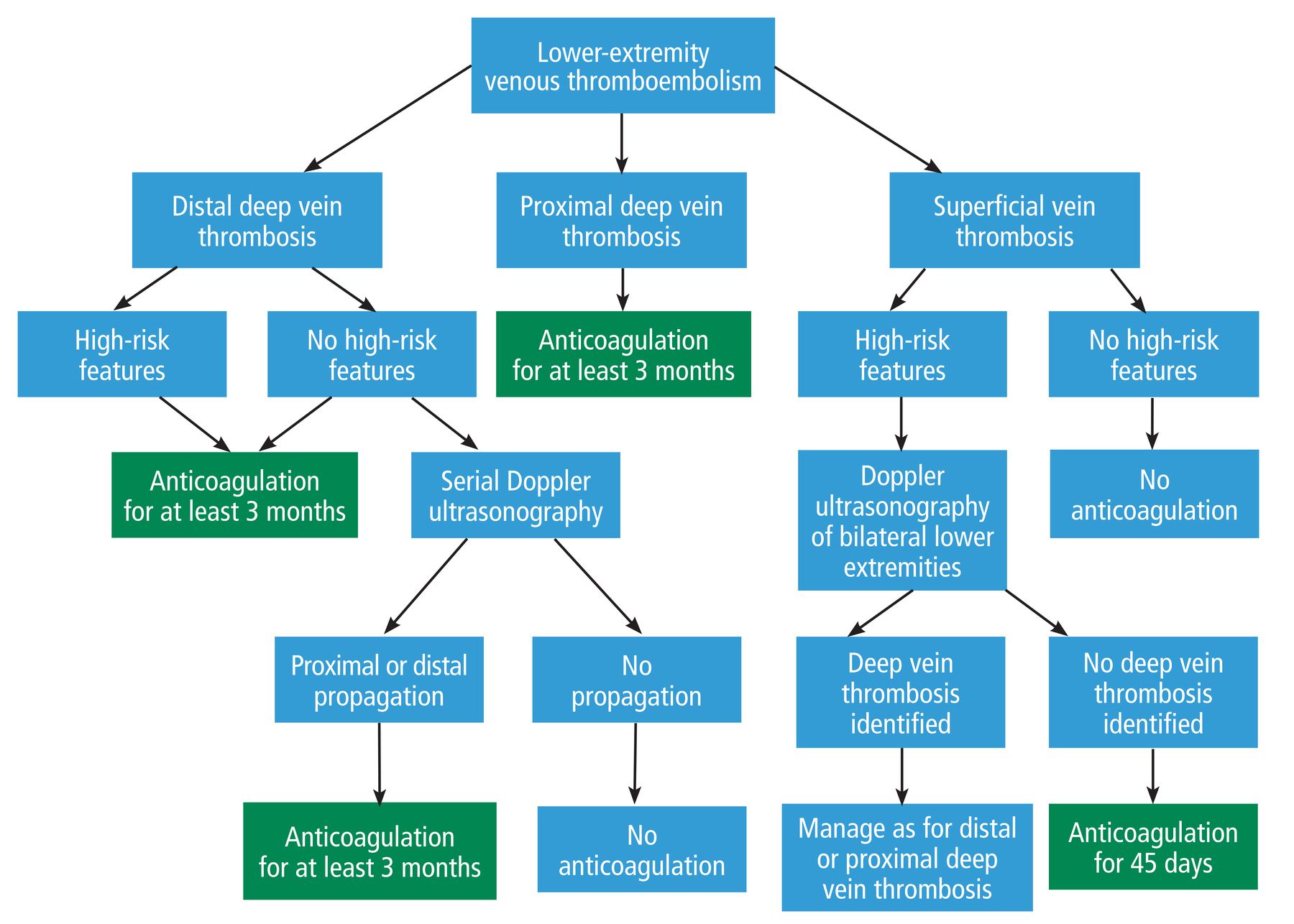
- Figure 1
Approach to lower-extremity venous thromboembolism.
Based on information in references 1,15, 24, and 26.

Tables
Severe symptoms (severe pain, throbbing pain when standing that improves with leg elevation, leg discoloration, swelling of the entire limb) Extensive thrombosis (> 5 cm in length, involving multiple veins, > 7 mm in diameter) Thrombosis close to the proximal veins No reversible provoking factor (ie, no transient or persistent risk factor up to 3 months before venous thromboembolic event) Active cancer (newly diagnosed cancer or cancer being treated with surgery, chemotherapy, radiotherapy, hormonal therapy, support therapy for terminal cancer, or combined treatments) History of venous thromboembolism Prolonged immobility (> 3 days) Patient currently has COVID-19 infection Based on information in references 1, 7–9.
Age greater than 75 Recent major bleeding, ie, requiring transfusion of 2 or more units of blood; retroperitoneal, spinal, or intracranial bleeding Severe liver dysfunction (baseline abnormal prothrombin time) Severe renal impairment (creatinine clearance rate < 30 mL/min) Severe thrombocytopenia (platelet count < 50 × 109/L) Cancer Acute hemorrhagic stroke or cerebral lesions at high risk of bleeding Severe uncontrolled hypertension Based on information in references 1, 8, 11, 13, and 14.
Extensive superficial vein thrombosis (> 5 cm) Involvement above the knee, particularly if 3 cm or less from the saphenofemoral junction Severe symptoms Involvement of the greater saphenous vein History of venous thromboembolism Active cancer Recent surgery Based on information in references 1, 15, and 16.
Vitamin K antagonists Direct oral anticoagulants Parenteral anticoagulation Warfarin Dabigatran Apixaban Rivaroxaban Edoxaban Low-molecular-weight heparins Fondaparinux Target Vitamin K Thrombin Factor Xa Factor Xa Factor Xa Antithrombin III Factor Xa Dosing Once daily Twice daily Twice daily Once daily Once daily Once or twice daily Once daily Monitoring needed Yes (INR) No No No No No No Comorbidity-specific recommendations Recommended for patients with antiphospholipid syndrome Recommended for patients with active cancer with no gastrointestinal or genitourinary involvement: rivaroxaban, apixaban, or edoxaban
Recommended for patients with cancer with gastrointestinal or genitourinary involvement: apixaban
For patients with recent acute coronary syndrome, avoid dabigatranRecommended for patients with active cancer and for pregnant patients Recommended for patients with high-risk superficial vein thrombosis Liver dysfunction considerations Can be used in patients with increased prothrombin time or INR Avoid in patients with increased prothrombin time or INR Can be used in patients with increased prothrombin time or INR Recommended for patients with high-risk superficial vein thrombosis; use with caution, monitor closely for signs of bleeding Renal dysfunction considerations Can be used in patients with creatinine clearance rate < 30 mL/min For patients with creatinine clearance 30–50 mL/min, preferred agents are rivaroxaban, apixaban, or edoxaban
Avoid all direct oral anticoagulants in patients with creatinine clearance rate < 30 mL/minUse doses adjusted for renal function as recommended in product labeling Avoid in patients with creatinine clearance rate < 30 mL/min INR = international normalized ratio
Based on information in references 11 and 21–24.
- TABLE 5
2021 American College of Chest Physicians guidelines on duration of anticoagulation for deep vein thrombosis, based on risk factors for venous thromboembolism
Risk factorsa Recommendation Major transient risk factors, occurring up to 3 months before the thrombotic event:
Surgery with general anesthesia for longer than 30 minutes
Confined to bed in hospital (only “bathroom privileges”) for at least 3 days with an acute illness
Cesarean delivery
The guidelines recommend against offering extended-phase anticoagulation (strong recommendation, moderate-certainty evidence) Minor transient risk factors, occurring up to 2 months before the thrombotic event:
Surgery with general anesthesia for less than 30 minutes
Admission to hospital for less than 3 days with an acute illness
Estrogen therapy
Pregnancy or puerperium
Confined to bed out of hospital for at least 3 days with an acute illness
Leg injury associated with reduced mobility for at least 3 days
The guidelines suggest against offering extended-phase anticoagulation (weak recommendation, moderate-certainty evidence)
In patients with venous thromboembolism diagnosed in the absence of a transient provoking factor, offer extended-phase anticoagulation with a DOAC (strong recommendation, moderate-certainty evidence)Persistent risk factors:
Active cancer (untreated, ongoing treatment or no potential curative treatment)
Inflammatory bowel disease
Antiphospholipid syndrome
In patients with antiphospholipid syndrome, vitamin K antagonists are suggested over DOACs as first-line treatment (weak recommendation with low-certainty evidence); a vitamin K antagonist can be offered for patients who can’t receive or who decline DOACs (weak recommendation, moderate-certainty evidence) Unprovoked thrombotic event (no transient or persistent risk factor identified) The guidelines recommend offering extended-phase anticoagulation with a DOAC (strong recommendation, moderate-certainty evidence); in patients who can’t receive a DOAC, extended-phase anticoagulation with a vitamin K antagonist is recommended (weak recommendation, moderate-certainty evidence) ↵a Previous venous thromboembolism is not mentioned clearly in the guidelines as affecting the duration of treatment.
DOAC = direct oral anticoagulant
Based on information in references 1 and 34.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.