


Article Figures & Data
Figures
- Figure 1
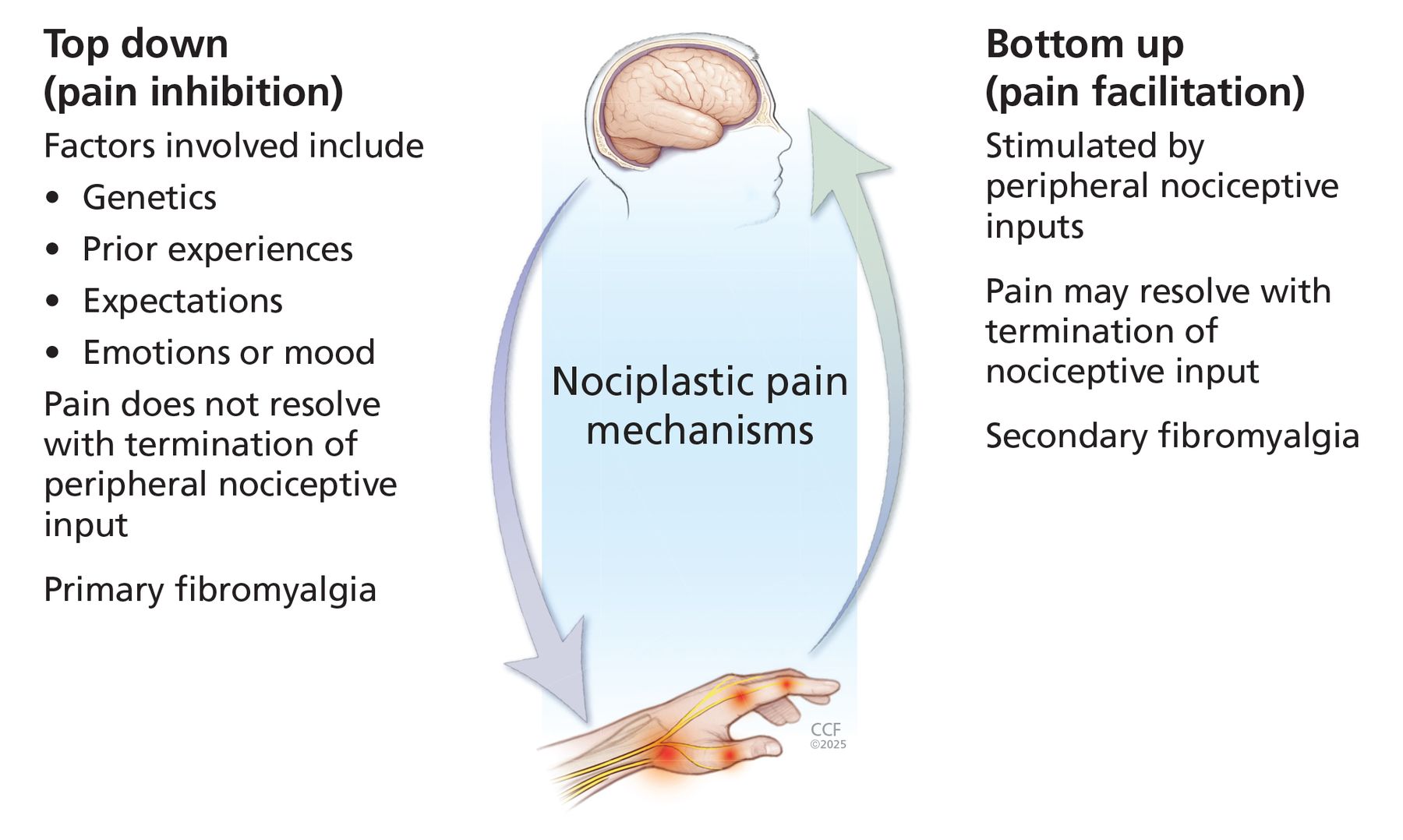
The mechanisms underlying nociplastic pain can be grouped into 2 broad categories: top-down (dysregulation in descending pathways involved primarily in pain inhibition) and bottom-up (dysregulation in ascending pathways primarily involved in pain facilitation).
Based on information from reference 7.
- Figure 2
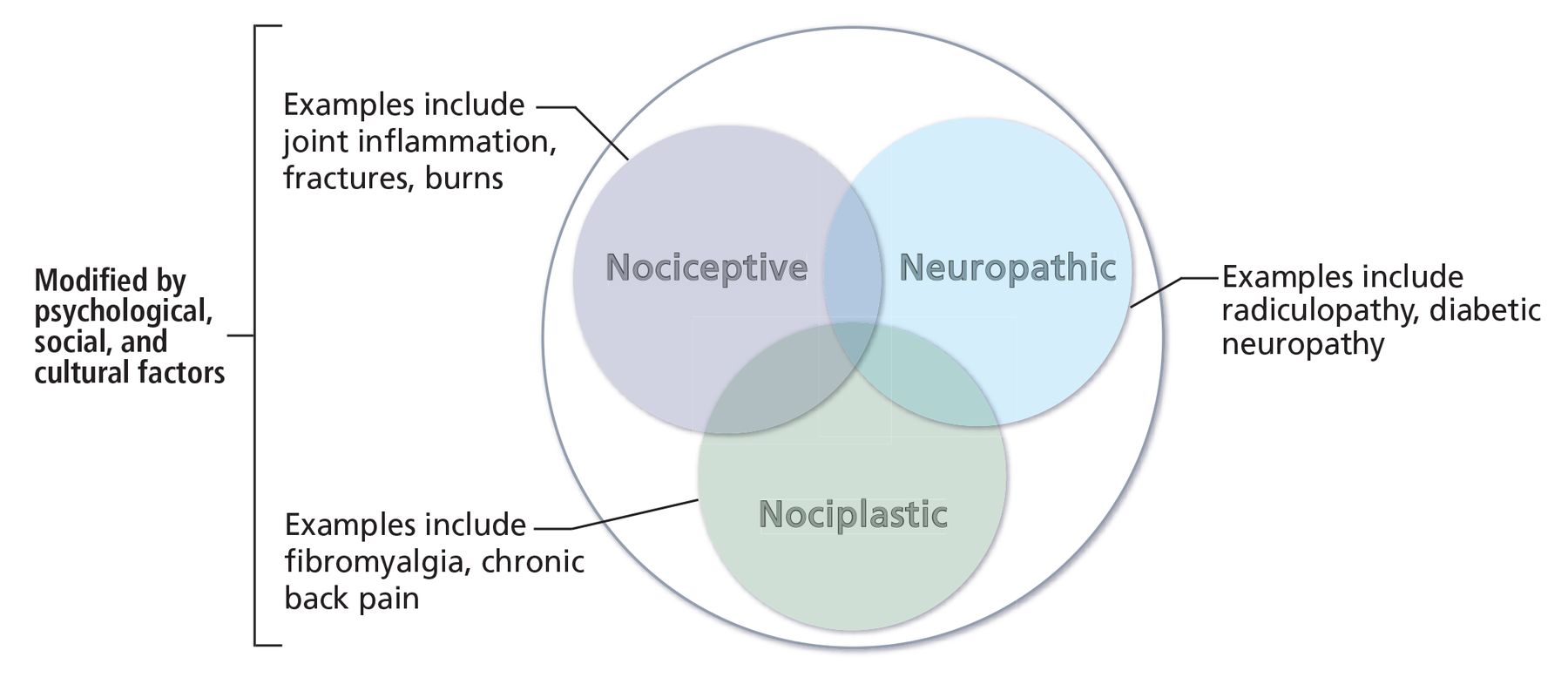
The pain continuum. There are 3 main categories of pain—nociceptive, neuropathic, and nociplastic—and these 3 types of pain can coexist.
Based on information from reference 7.


Tables
Pain type Defining characteristics Examples Treatment Nociceptive Pain due to tissue injury, inflammation, damage, or degeneration Osteoarthritis, rheumatoid arthritis, fracture, burns Topical analgesics, nonsteroidal anti-inflammatory drugs, acetaminophen, opioids, steroids Neuropathic Pain due to nerve injury or damage Radiculopathy, diabetic neuropathy, chemotherapy-induced neuropathy Topical or local therapy; systemic neuropathic medications such as gabapentin, pregabalin, and tricyclic antidepressants Nociplastic Pain arising from a sensitized nervous system (amplified processing of pain signals, decreased inhibition of pain, or both) Fibromyalgia, chronic back pain, chronic temporomandibular pain disorders Multimodal management approach Based on information from reference 6.
Barrier: Previsit bias
Mitigation: Eliminate any bias or negativity before the visit when the primary reason is “chronic pain” or “fibromyalgia” to improve clinician receptiveness and reduce frustration13
Avoid dismissive attitude toward the pain complaint10,11
Believe patient reports of the severity and adverse effects of painBarrier: Difficulty connecting with patients and winning their confidence and trust
Mitigation: Be empathetic and acknowledge that the pain is real; validating and legitimizing the pain can be emotional for patients and helps increase their trust and receptiveness11
Let patients narrate their symptoms and fully explain the impact of pain in their lives, which provides a crucial sense of being heard10
Debunk the myth that nociplastic pain is not a real condition and explain that the pain is not imagined or all in their head to make patients feel believed and heard12,13
Express to patients that we understand their pain and we will partner with them to help manage it as best we can
Share decision-making to reduce frustration toward clinicians and increase patient receptiveness, motivation, and adherence to therapeutic recommendationsBarrier: Unrealistic or unreasonable expectations
Mitigation: Patients may hope that a “magic pill” will fix the problem, and that can lead to frustration
Set realistic expectations upfront (eg, improve physical function), but be extremely empathetic14
Reassure patients that adequate pain control can be achieved, although the fix is not easy
Enable patients to take charge of their pain management, but provide assurance that they will always be supportedBarrier: Overexpectation to completely eliminate the problem
Mitigation: Focus on legitimizing and validating pain while also determining any acute causes of a pain flare
Accept that adequate pain management may not be curative, but even limited pain relief may enable patients to revive skills, renew social interactions, and improve quality of life
Modest gain in pain relief can significantly increase patient confidence in overcoming the pain and is a vital clinical accomplishment11
Focus on both the biological and psychosocial determinants of chronic pain (ie, mind–body dualism)13Barrier: Poor understanding of nociplastic pain and contributory factors
Mitigation: Explain pain physiology to patients, which may improve health status (less worry about pain and long-term improvement in physical functioning, vitality, mental health) and increase endogenous pain inhibition in patients with fibromyalgia15Barrier: Appointment time constraints
Mitigation: Schedule a separate appointment focused only on pain management; defer rest of care to another visit
Schedule a few extended appointments at first to allow time to really listen to patientsBarrier: Diagnosis challenge and lack of knowledge and training
Mitigation: Diagnosis is difficult due to inconsistent symptom recognition and diagnosis validity and lack of robust guidelines; even when guidelines are available, level of awareness may vary11
Learning about nociplastic pain and management principles is crucialBarrier: Referrals and resources
Mitigation: Multidisciplinary approach can be helpful, but avoid unnecessary referrals that can lead to frustration
Create achievable short- and long-term pain management goalsAutoimmune inflammatory arthritis Osteoarthritis or mechanical arthritis Nociplastic pain or fibromyalgia Autoimmune inflammation of the joints or tissue
Presence of red, hot, swollen joints with palpable joint fluid and warmth
Symptoms most pronounced in the morning and starts improving after 30 to 60 minutes of moving
Rest aggravates pain and stiffness
Responds to low-to-moderate dose of steroid; symptoms return after medication cessationRelated to tissue injury or degeneration
Can have transient morning pain and stiffness lasting less than 15 to 30 minutes
Pain worsens with activity and joint use throughout the day
Symptoms more prominent in the evenings, especially when joints were used more throughout the day
Rest makes the pain better except for transient pain and stiffness when getting up after a period of rest (ie, gelling phenomenon)Heightened pain sensitivity at the brain and spinal cord level
Pain is usually widespread with associated diffuse tenderness
Related fatigue, poor sleep, brain fog, or irritable bowel symptoms
Worsens with poor sleep and stressBased on information from reference 7.
Chronic primary headache and orofacial pain
Chronic migraine
Chronic tension-type headache
Trigeminal autonomic cephalalgias
Chronic temporomandibular pain disorders without anatomic abnormality or explanation
Chronic burning mouth
Chronic primary orofacial painChronic visceral pain syndrome
Chronic primary bladder pain syndrome or interstitial cystitis
Chronic pelvic pain syndrome
Irritable bowel syndrome
Chronic chest pain
Chronic abdominal painChronic primary musculoskeletal pain
Primary cervical, thoracic, lower back, and limb pain; extent of pain and suffering is greater than expected based on the underlying pathology9
Complex regional pain syndromeDifficulty localizing pain Chronic fatigue Memory problems (ie, brain fog) Anxiety or depression Poor sleep quality Irritable bowel symptoms Chronic headache Chronic pelvic pain Hypersensitivity to nonpainful stimuli (light sensitivity, sound sensitivity, allodynia or hyperalgesia) Report of more comorbid illnesses Intolerance to multiple medications without true allergy Frequent use of healthcare services Based on information from reference 9.
Type and components Description Cognitive behavioral therapy A technique to cope with pain and convert unpleasant stimuli to pleasant stimuli
Focuses on reducing pain and distress by modifying physical sensations, catastrophic thinking, and maladaptive behaviors29Distraction Involves engaging in thoughts or activities (eg, finding joy, relaxation techniques, diaphragmatic or belly breathing, social activities) that distract from pain
One of the most used and highly endorsed strategies for controlling pain30Activity pacing A 2-part strategy that involves spending just enough time on an activity to get the most out of it without pushing so far that patients experience more pain; over time, patients may be able to do more
1. Conserve energy for activities patients value (eg, playing with their kids or undertaking a pleasurable recreational activity)
2. Set graduated activity quotas to help increase ability to do activities (tolerance) and reduce disabilityCognitive restructuring Helps reframe negative thoughts into more positive adaptive thoughts Other Includes relaxation, guided imagery, and meditation that can be helpful with pain management
Telehealth can be an excellent resource, particularly for patients with inadequate access to mental health professionals31Mind–body therapy Mindfulness A nonelaborative, nonjudgmental awareness of the present-moment experience32
Involves breathing methods, guided imagery, and other techniques to relax the body and mind and to help reduce stress
Uses cognitive reappraisal to help separate the sensation of pain from the alarm reaction, which reduces the pain experience33
A recent study on veterans with chronic pain showed telehealth-based mindfulness intervention improved pain-related function and biopsychosocial outcomes compared with standard care34Tai chi A mind–body activity that combines meditation with slow, gentle, graceful movements, as well as deep breathing and relaxation, to move vital energy (or qi) throughout the body
A complex multicomponent intervention that integrates physical, psychosocial, emotional, spiritual, and behavioral elements35
Evidence shows clinically important improvements in symptoms, disability, and quality of life in patients with chronic widespread pain36Yoga Evidence supports a role in reducing nociplastic pain32 Psychodynamic therapy An in-depth form of talk therapy that focuses on unconscious processes based on previous unresolved conflicts or dysfunctional relationships that can shape present behavior
Goal is to create self-awareness and understand how the past influences present behavior and then rectify it
Focuses more on the patient’s relationship with the external world rather than the patient–therapist relationshipHypnosis and hypnotherapy Explores the subconscious mind and causes an altered state of consciousness to prevent normally perceived experiences, such as pain, from reaching the conscious mind Drug class and medication Predominant symptoms and dose Potential side effects Selective serotonin-norepinephrine reuptake inhibitors Pain and depression Duloxetine Start at 30 mg in morning; can increase to 60 mg daily in a few weeks as tolerated14 Nausea, headache, diarrhea; do not stop suddenly—taper off gradually Milnacipran Start at 12.5 mg in the morning, increase by 12.5 mg every few weeks to 50–100 mg once or twice daily as tolerated14 As above Tricyclic antidepressants Pain, sleep, fatigue, and overall quality of life Amitriptyline Start at 5–10 mg 1 to 3 hours before bedtime; increase by 5 mg no more frequently than every 2 weeks; use lowest dose possible (20–30 mg)46 Dry mouth, dry eyes, blurred vision, flushing, constipation, urinary retention, dizziness, drowsiness, cardiac arrythmia Nortriptyline Start at 10 mg at bedtime; up to 75 mg maximum46 Like amitriptyline but preferred due to fewer anticholinergic side effects Alpha 2 delta ligands Prominent sleep disturbance Pregabalin Start at 25–50 mg at bedtime; increase by 25–50 mg every 2 to 4 weeks to 300–450 mg daily (in 1 or 2 divided doses) as tolerated14 Dizziness, drowsiness, peripheral edema, weight gain, blurred vision Gabapentin Start at 100 mg at bedtime; increase by 100 mg every 2 to 4 weeks to 1,200–2,400 mg daily (usually in 2 or 3 divided doses) as tolerated46 As above
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.