


A 40-year-old man who hunted large and small game and had frequent exposure to ticks was admitted to the hospital with persistent fevers, peaking at 102.6°F (39.2°C), and a transient episode of monocular vision loss.
About 9 months earlier, he developed night sweats, fatigue, and arthralgias, and over the next several months he noted ongoing fatigue, intermittent night sweats, and a 10-lb weight loss. He also had an episode of transient loss of vision in his left eye. When he sought medical care about 4 months earlier, tests for Borrelia burgdorferi immunoglobulin M (IgM) and Ehrlichia chaffeensis IgG were positive; he was started on doxycycline and experienced modest improvement.
See related editorial, page 316
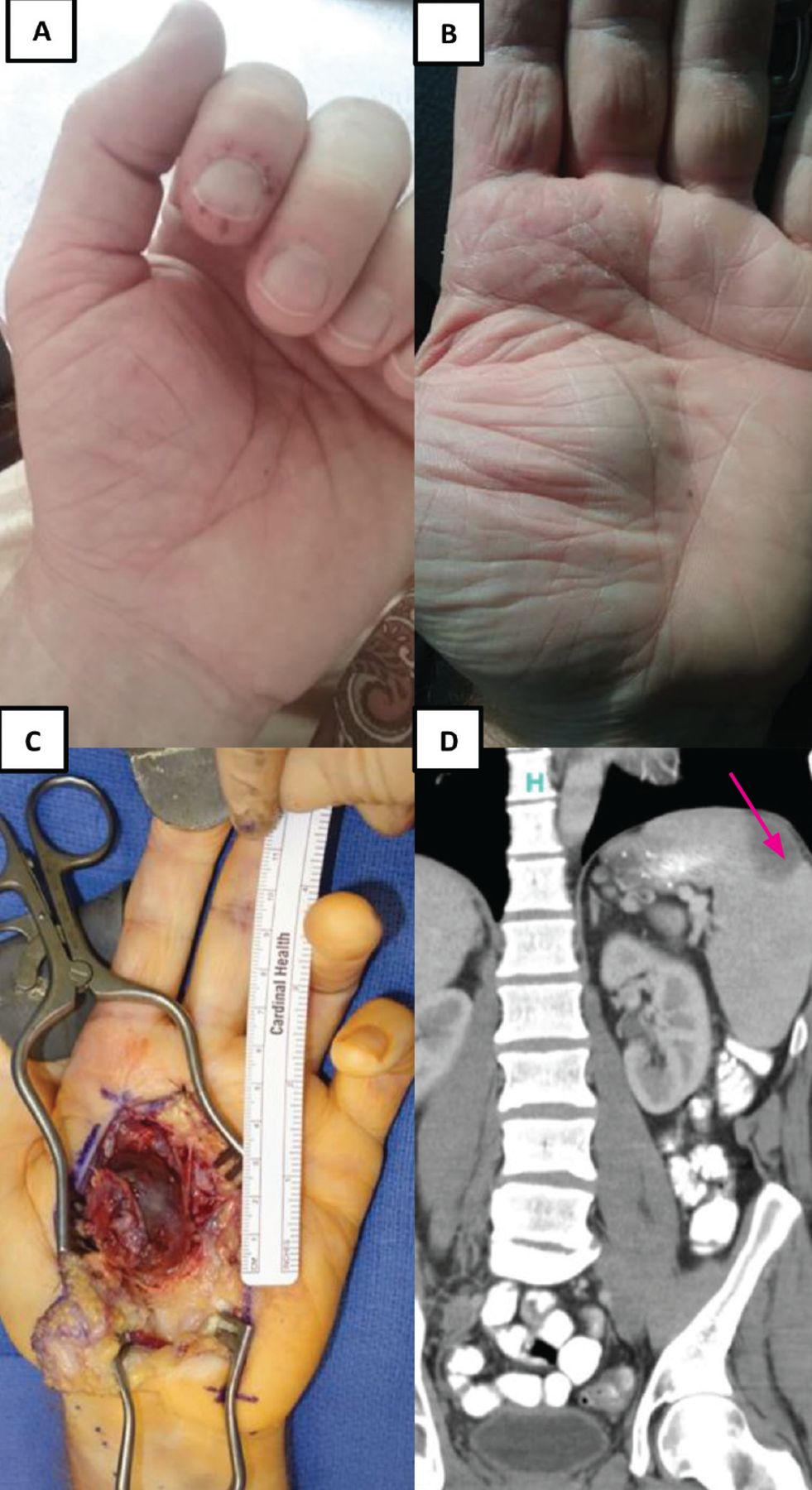
However, during the next month, he developed pain in his left index finger and right second toe, with periungual and digital petechiae (Figure 1A), and then developed a painful pulsatile palmar mass (Figure 1B). Magnetic resonance angiography at another medical facility revealed a superficial palmar arch aneurysm that was subsequently excised (Figure 1C). He also developed new left scapular pain, and computed tomography showed evidence of a wedge-shaped splenic infarct (Figure 1D).
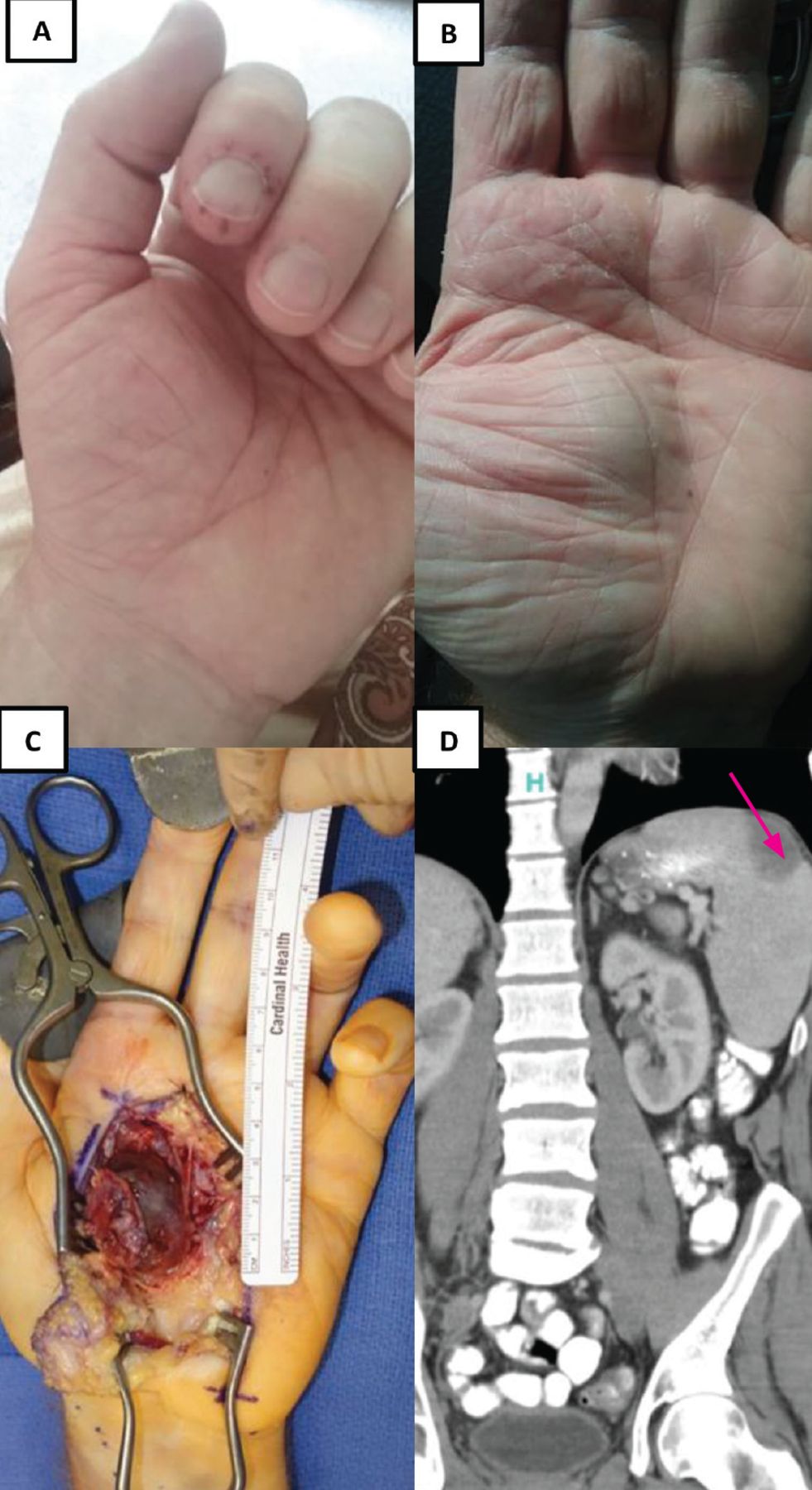
Findings before presentation: (A) painful periungual petechial rash on the left index finger; (B) pulsatile palmar mass; (C) intraoperative image of the aneurysm arising from the superficial palmar arch; and (D) abdominal computed tomography showing a wedge-shaped splenic infarct (arrow).
On admission to our hospital, he did not appear ill. Cardiac examination revealed a grade III/IV blowing diastolic murmur at the left lower sternal border. There were painful grouped petechiae and splinter hemorrhages affecting the left great toe (Figure 2). Results of laboratory testing were as follows:
White blood cell count 6.48 × 109/L (reference range 4.5–11.0)
Platelet count 280 × 109/L (150–350)
Hemoglobin level 11.0 g/dL (13.9–16.3)
Hematocrit 35% (41–53)
Erythrocyte sedimentation rate 33 mm/h (1–15)
C-reactive protein 5.6 mg/dL (< 0.5)
Rheumatoid factor 649 IU/mL (0–35).

Painful petechial rash affecting the left great toe, compatible with Osler nodes, and splinter hemorrhage of the toenail.
B burgdorferi antibody, Babesia microti IgG and IgM, and E chaffeensis polymerase chain reaction testing were negative.
Transthoracic echocardiography detected a vegetation on the left coronary cusp of the aortic valve. Blood cultures on the first and second hospital days were positive for Streptococcus mutans.
The patient’s evolving distal signs, aortic regurgitation murmur, results of echocardiography, and microbiologic data were confirmatory of subacute bacterial endocarditis, and an extended course of antimicrobial therapy was implemented.
EMBOLIC MANIFESTATIONS OF ENDOCARDITIS
Early in this patient’s course, the repeated exposure to ticks and the positive serology for Lyme disease and ehrlichiosis prompted treatment with doxycycline. However, the development of distal embolic phenomena, transient visual impairment, splenic infarct, and pulsatile palmar mass compelled reconsideration of the underlying infectious process.
Janeway lesions (painless hemorrhagic or erythematous lesions on the palms and soles developing as septic emboli) and Osler nodes (painful petechial eruptions on the finger pads and toes), understood to arise from immune complex deposition, are classic features of endocarditis.1,2 They are helpful clues to uncover the diagnosis. This patient’s sudden visual disturbances, albeit transient, and shoulder pain were instructive additive symptoms arising as immunologic and vascular occlusive insults to the retina and spleen, respectively.1,3
Elevated rheumatoid factor is present in one-third of patients with confirmed endocarditis, arising from sustained inflammation, thereby inducing polyclonal hypergammaglobulinemia.3,4 The painful palmar swelling arose from a mycotic aneurysm of the superficial palmar artery. Surgical pathology identified a dilated arterial wall with granulation tissue, acute and chronic inflammation, and prominent luminal thrombus. Interestingly, mycotic aneurysms may occur in 10% to 20% of patients in large endocarditis series, and were described by Sir William Osler as “mycotic endarteritis” in 1885.5 They may arise in the cerebral, splenic, coronary, pulmonary, and mesenteric arteries and in the abdominal aorta.1,2
THE PATIENT’S MANAGEMENT
In our patient, the evolving distal signs, along with the lack of specificity and potential for false-positive results of serologic bloodwork for Lyme disease and ehrlichiosis, necessitated a reformulation of the underlying disease process and the establishment of the diagnosis of bacterial endocarditis.6
On completion of a 4-week course of intravenous penicillin G, our patient achieved complete resolution of symptoms.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2021 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.