


An 85-year-old woman presented with a 9-month history of pruritus in the left breast and unremarkable medical history. On examination, a brownish erythematous patch was observed in the nipple-areola complex (Figure 1).

Brownish erythematous patch in the nipple-areola complex.
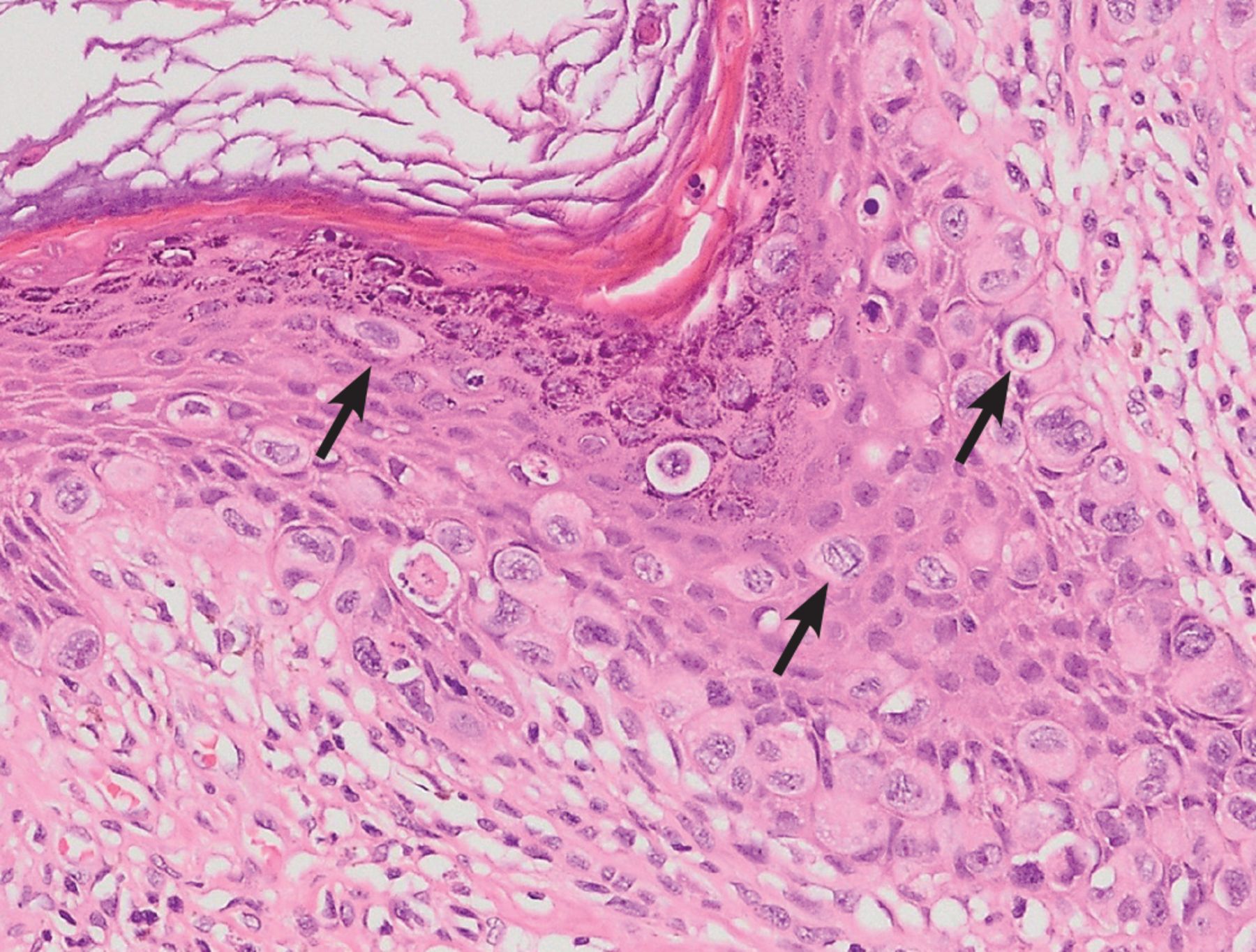
Skin-punch biopsy revealed single cells and small clusters of neoplastic cells throughout the epidermis and granular layer, with abundant pale cytoplasm, intraglandular extension, and chronic inflammation in the papillary dermis (Figure 2), resulting in the diagnosis of Paget disease of the breast.
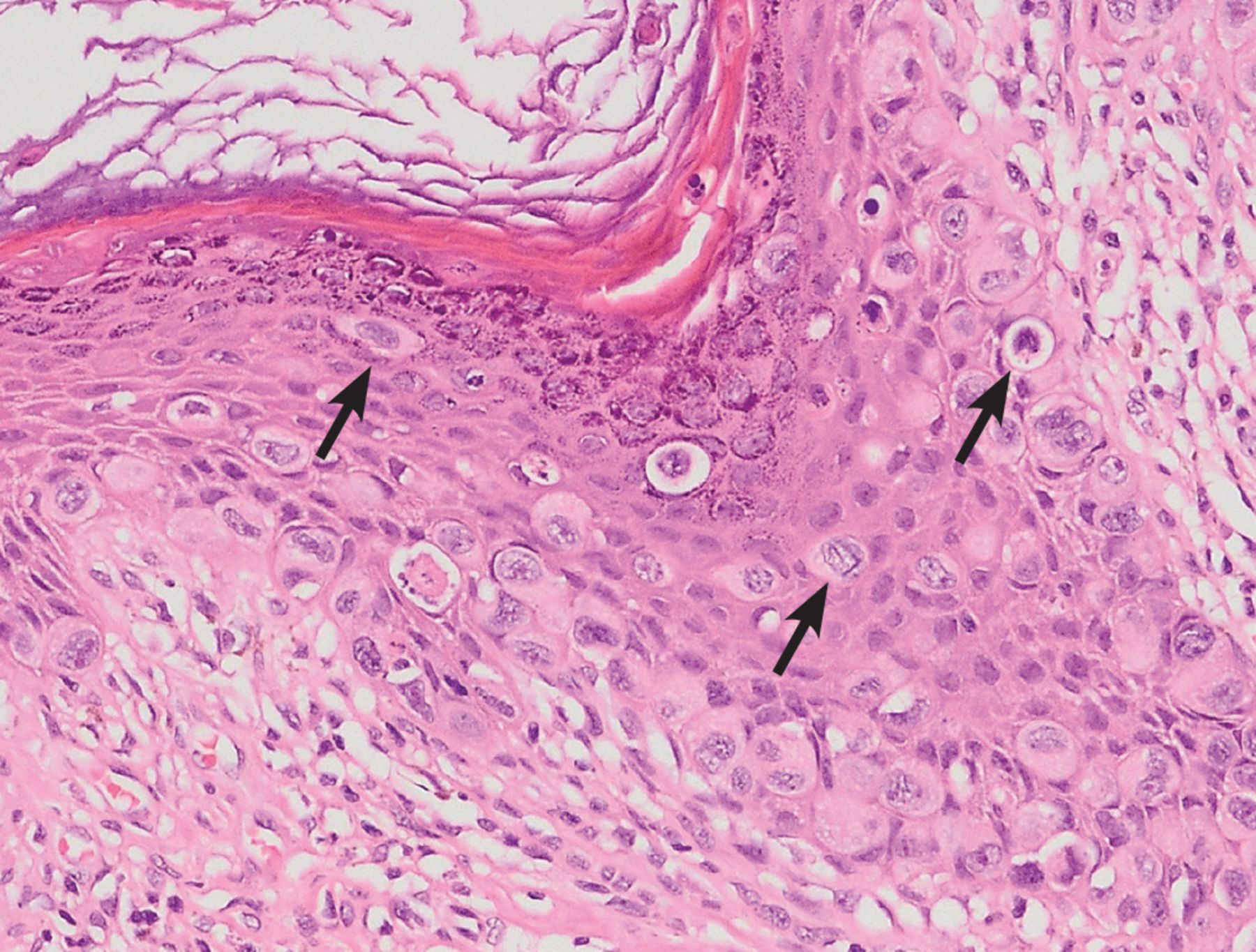
Skin biopsy showing single cells and small clusters of neoplastic cells (arrows) through the epidermis, with abundant pale cytoplasm (hematoxylin and eosin, × 400).
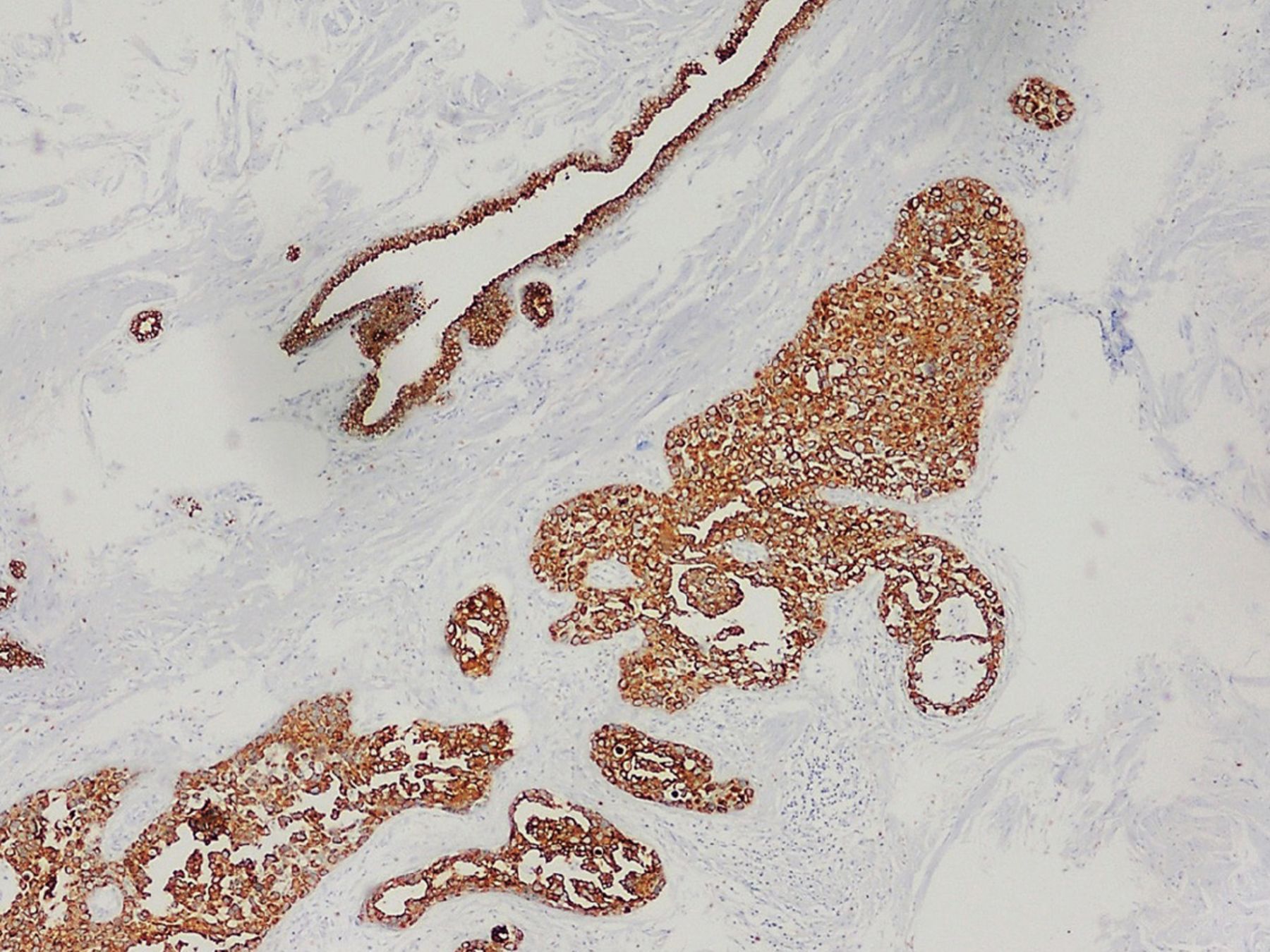
Mammography to rule out underlying tumor did not reveal pathologic features. Breast-conserving surgery was recommended, and the patient underwent a nipple-areola complex lumpectomy without axillary dissection, followed by adjuvant radiotherapy. Surgical specimen histologic findings were consistent with ductal carcinoma in situ of the breast, revealing sheets of neoplastic and cohesive cells in the ductal lumen. Results of immunohistochemistry showed strong staining with cytokeratin 7 (Figure 3) and human epidermal growth factor receptor 2 (HER-2).
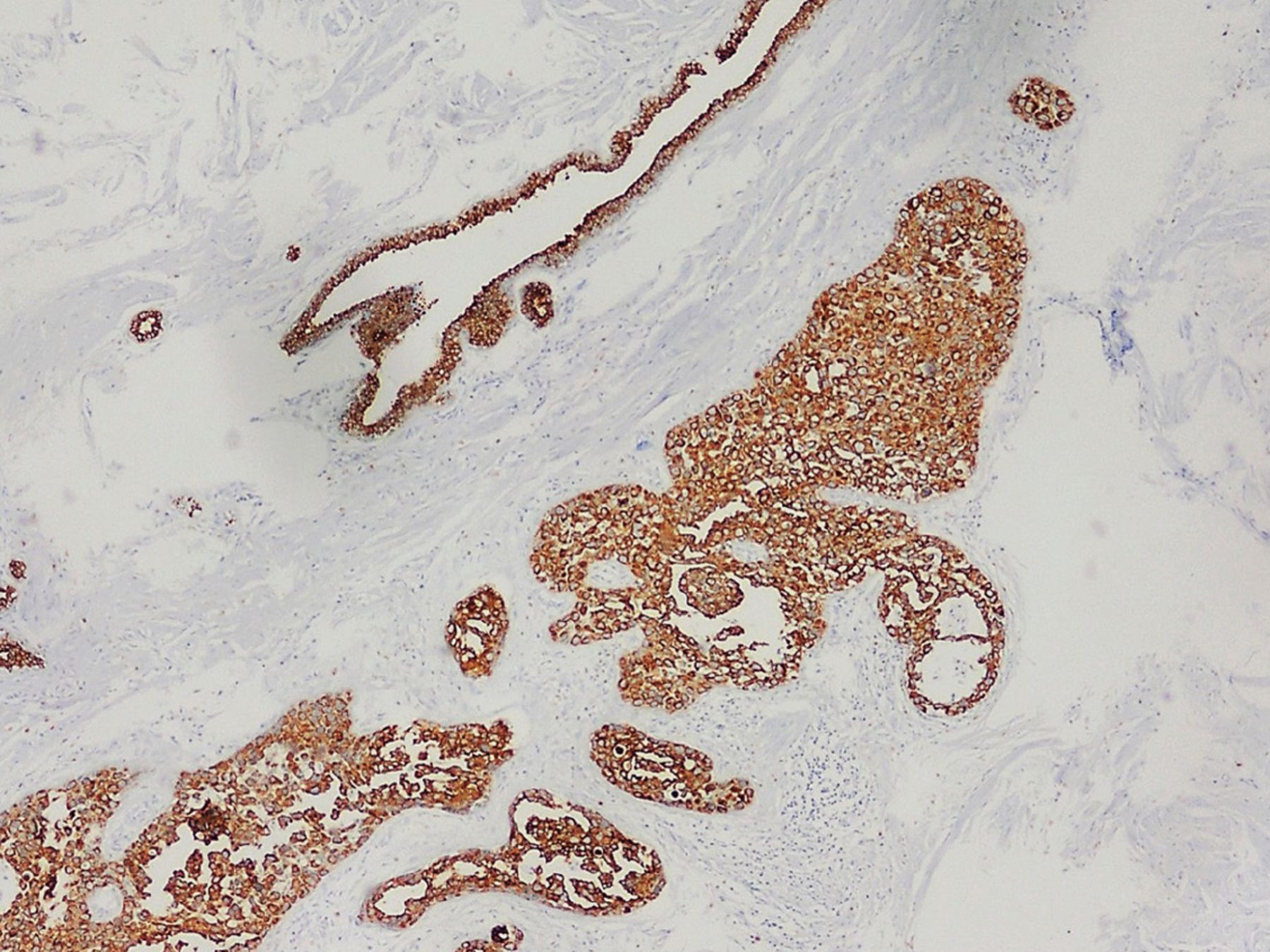
Strong staining of the surgical specimen with cytokeratin 7 in the surgical specimen confirmed the presence of cohesive neoplastic cells in the ductal lumen.
Paget disease of the breast usually presents as a brownish erythematous scaly plaque affecting the nipple-areola complex.1,2 This condition can be mistaken for other skin diseases including atopic dermatitis, allergic contact dermatitis, and Bowen disease.3 Extramammary Paget disease, commonly located in the anogenital area or perineal area and axilla, has also been described.1 However, while mammary Paget disease is often associated with underlying breast carcinoma,1–3 extramammary Paget disease with underlying malignancies occurs less frequently because Paget cells originate from ductal cancer cells that migrate from breast parenchyma along the basal membrane of the nipple.2 These tumor cells have glandular features that are large and pale with abundant clear cytoplasms and atypical nuclei with prominent nucleoli. Expression of cytokeratin 7, GATA binding protein 3 (a regulator of mammary luminal cell differentiation), and HER-2 are useful to confirm diagnosis.1,3
Mammography may fail to detect neoplasms in up to 50% of patients, and disease extent can be underestimated in up to 43%.1,4 Magnetic resonance imaging can help identify occult malignancy, axillary node involvement, and candidacy for breast conservation surgery.1,4,5
A high level of suspicion for nipple-areola abnormalities is required for prompt diagnosis of Paget disease. Radiologic evaluation, histopathologic study, and immunohistochemistry are essential tools in the assessment of this condition.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2022 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.