


Article Figures & Data
Figures
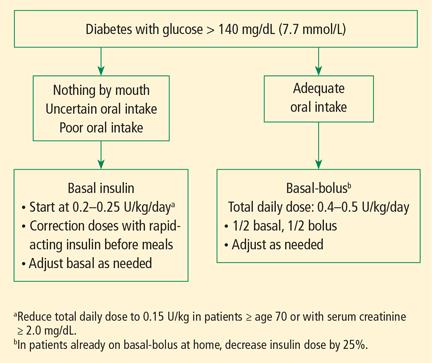
- FIGURE 1
Initial insulin treatment for patients with type 2 diabetes in the non-intensive care setting.

Tables
Organization Intensive care unit Non-intensive care unit American Diabetes Association/American Association of Endocrinologists13 Initiate insulin therapy for persistent hyperglycemia (glucose > 180 mg/dL [10 mmol/L]).
Treatment goal: For most patients, target a glucose level between 140 and 180 mg/dL.
More stringent goals (110–140 mg/dL) may be appropriate for select patients, if achievable without significant risk of hypoglycemia.No specific guidelines.
If treated with insulin, premeal glucose targets should generally be < 140 mg/dL, with random glucose levels < 180 mg/dL.American College of Physicians46 Recommends against intensive insulin therapy in patients with or without diabetes in surgical or medical intensive care.
Treatment goal: Target glucose level is between 140 and 200 mg/dL in patients with or without diabetes in surgical or medical intensive care.Critical Care Society29 Glucose level > 150 mg/dL should trigger insulin therapy.
Treatment goal: Maintain glucose level < 150 mg/dL for most adult patients in intensive care.
Maintain glucose level < 180 mg/dL while avoiding hypoglycemia.Endocrine Society26 Premeal glucose target < 140 mg/dL.
Random glucose < 180 mg/dL.
A lower target range may be appropriate in patients able to achieve and maintain glycemic control without hypoglycemia.
Glucose < 180–200 mg/dL is appropriate in patients with terminal illness or with limited life expectancy or at high risk for hypoglycemia.
Adjust antidiabetic therapy when glucose falls < 100 mg/dL to avoid hypoglycemia.Society of Thoracic Surgeons28 Guidelines specific to adult cardiac surgery.
Continuous insulin infusion preferred over subcutaneous or intermittent intravenous boluses.
Treatment goal: Recommend glucose < 180 mg/dL during surgery (≤ 110 mg/dL in fasting and premeal states).Joint British Diabetes Societies27 Target glucose levels in most patients are between 6 and 10 mmol/L (108–180 mg/dL) with an acceptable range of between 4 and 12 mmol/L (72–216 mg/dL). Insulin class Generic (brand) Onset Peak Duration Fast- or rapid-acting Aspart (Novolog) 10–15 min ~60 min 3–4 hrs Lispro (Humalog) 10–15 min ~60 min 3–4 hrs Glulisine (Apidra) 10–15 min ~60 min 3–4 hrs Short-acting Regular insulin (Humulin R, Novolin R/ReliOn R) 30–60 min 2–4 hrs 6–8 hrs Intermediate-acting NPH insulin (Humulin N, Novolin N/ReliOn N) 1–2 hrs 3–8 hrs 12–15 hrs Long-acting Glargine (Lantus) 2 hrs No real peak 22–24 hrs Glargine (Toujeo) 6 hrs No real peak 22–24 hrs Glargine (Basaglar)a 2 hrs No real peak 24 hrs Detemir (Levemir) 3–8 hrs No real peak 17–24 hrs Degludec (Tresiba) 1 hr No real peak 42 hrs Premixed 75% Insulin lispro protamine/25% insulin lispro (Humalog mix 75/25) 5–15 min Dual 10–16 hrs 50% Insulin lispro protamine/50% insulin lispro (Humalog mix 50/50) 5–15 min Dual 10–16 hrs 70% Insulin lispro protamine/30% insulin aspart (Novolog mix 70/30) 5–15 min Dual 10–16 hrs 70% NPH insulin/30% regular insulin (Humulin, Novolin/ReliOn) 30–60 min Dual 10–16 hrs ↵a Approved by the US Food and Drug Administration; scheduled to be marketed December 2016.
NPH = neutral protamine Hagedorn.
- TABLE 3
Comparison of medications for the management of hyperglycemia in the hospital setting
Medication Advantages Disadvantages Insulin Extensive experience with glycemic control
Protocols widely available
Easy to adjust in the event of hypoglycemia, changes in nutrition, diagnostic procedures, or reduced kidney functionHypoglycemia
Common source of hospital errors
Requires injectionGLP-1-based therapy Good glucose-lowering effect
Low risk for hypoglycemia
Nonglycemic beneficial effectsLimited data on safety and efficacy
Gastrointestinal side effects
InjectableMetformin Good glucose-lowering effect
Low risk for hypoglycemia
Inexpensive
Oral routeLimited experience
Risk of lactic acidosis in patients with impaired kidney function, heart failure, hypoxemia, alcoholism, cirrhosis, contrast exposure, surgery, and shock
Gastrointestinal side effectsSulfonylureas Good glucose-lowering effect
Inexpensive
Oral routeRisk for hypoglycemia especially in patients with reduced oral intake or impaired renal function. Thiazolidinediones Good glucose-lowering effect
Low risk of hypoglycemia
Oral routeSlow onset of action
Contraindicated in patients with heart failure and hepatic dysfunction
Fluid retentionBromocriptine-quick release Low risk of hypoglycemia
Oral routeNo studies in the hospital
Risk of hypotension, dizzinessColesevelam Low risk of hypoglycemia
Oral routeNo studies in the hospital
ConstipationDPP-4-inhibitors Modest glucose-lowering effect
Low risk of hypoglycemia
No major side effects reported in pilot trial
Oral routeLimited experience
Contraindicated in patients with history of pancreatitisSGLT-2-inhibitors Good glucose-lowering effect
Low risk of hypoglycemia
Oral routeLimited experience
Increase risk of urinary and genital tract infections
Risk of dehydration, hypotensionDPP-4 = dipeptidyl peptidase-4; GLP-1 = glucagon-like peptide-1; SGLT-2= sodium-glucose cotransporter-2.
Altered state of consciousness Suicidal ideation Prolonged instability of glucose levels Diabetic ketoacidosis Patient or family inability or refusal to participate in own care Insulin pump malfunction Lack of appropriate supplies for the insulin pump Other circumstances as identified by the healthcare provider Reprinted with permission from John Wiley and Sons (Lansang MC, Modic MB, Sauvey R, et al. Approach to the adult hospitalized patient on an insulin pump. J Hosp Med 2013; 8:721–727). © 2013 Society of Hospital Medicine.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- EMERGE: Evaluating the value of measuring random plasma glucose values for managing hyperglycemia in the inpatient setting
- ASSOCIATION OF HYPERGLYCEMIA WITH HOSPITAL MORTALITY IN COVID-19 PATIENTS WITHOUT DIABETES: A COHORT STUDY
- 15. Diabetes Care in the Hospital: Standards of Medical Care in Diabetes--2021
- 15. Diabetes Care in the Hospital: Standards of Medical Care in Diabetes--2020
- 15. Diabetes Care in the Hospital: Standards of Medical Care in Diabetes--2019
- 14. Diabetes Care in the Hospital: Standards of Medical Care in Diabetes--2018
- 14. Diabetes Care in the Hospital