


In 80-year-old woman presented with dyspnea on exertion, present for the last 2 years. She said she became short of breath after walking 1 block. Her medical history was significant only for 35 pack-years of smoking.
On examination, her lung fields were clear, with no audible murmurs, and she had no lower-extremity edema. Her oxygen saturation was 98% on room air.
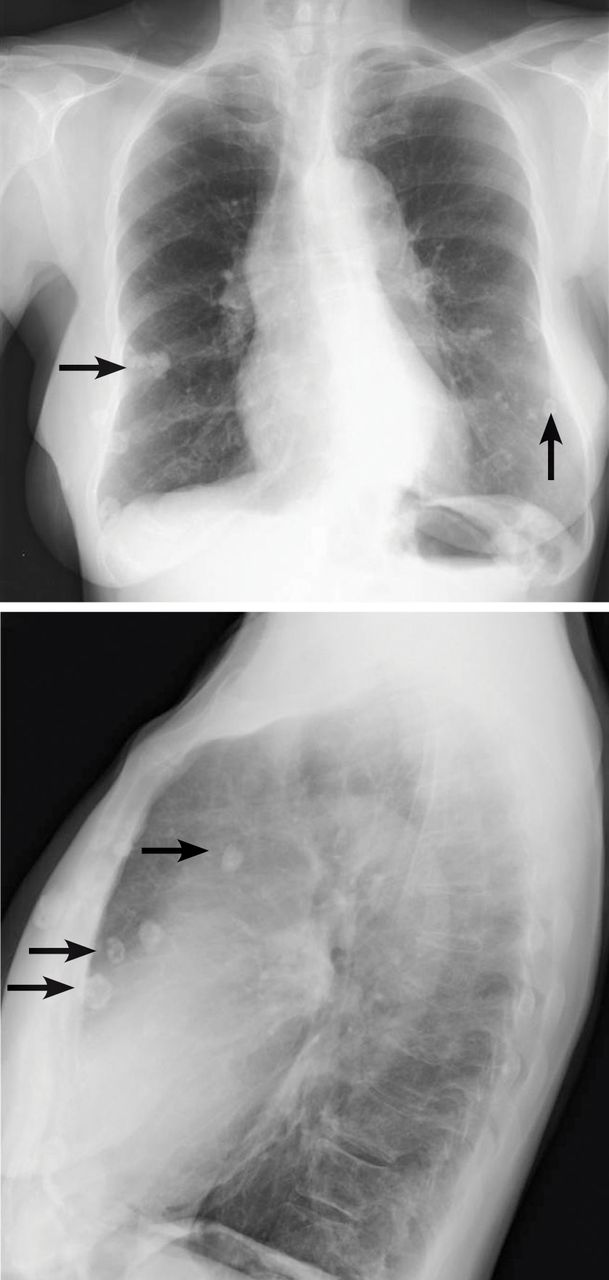
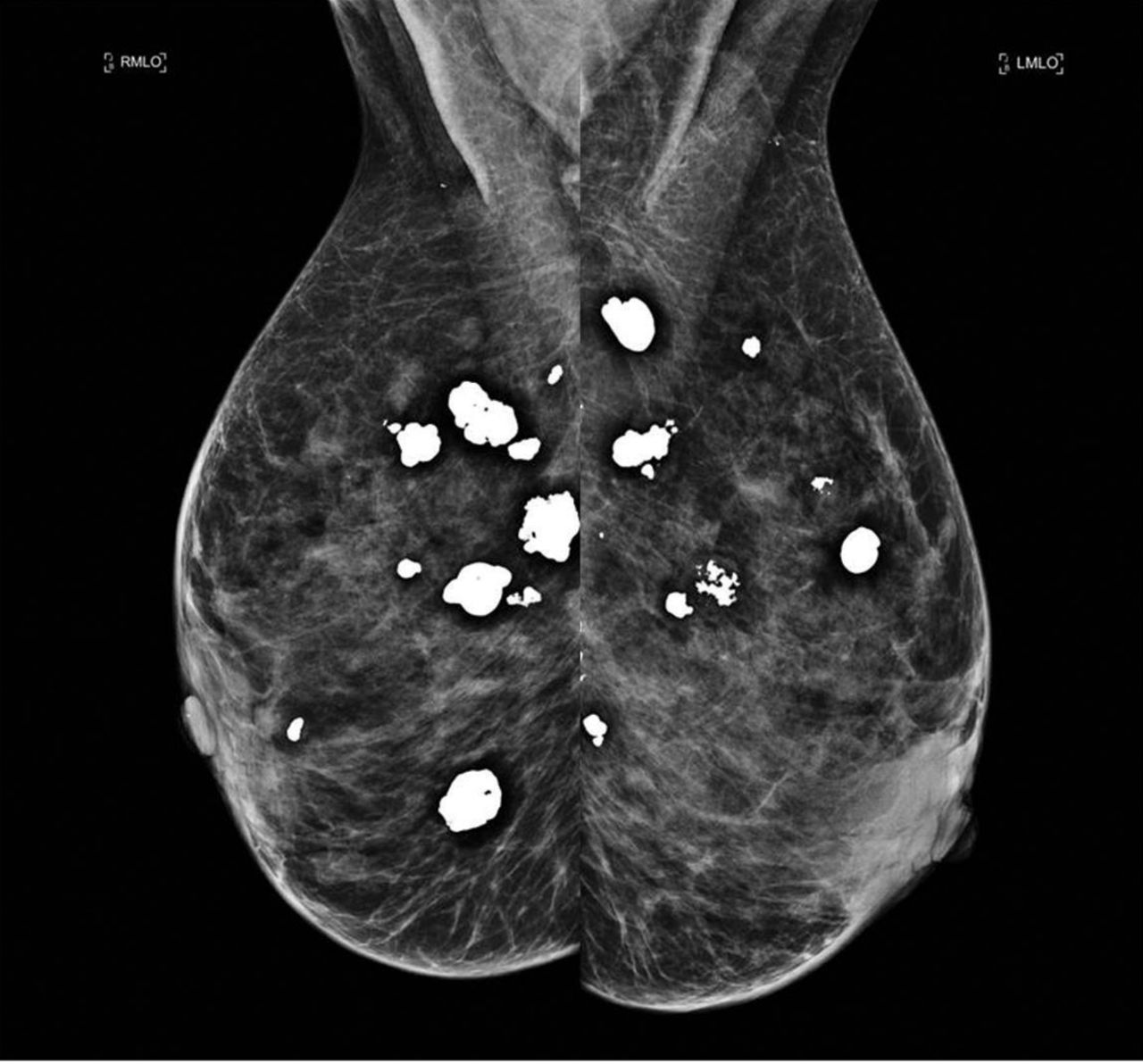
Chest radiography as part of the initial evaluation showed lesions on both sides that looked like pulmonary nodules. The locations of the lesions were similar on frontal and lateral views (Figure 1). No previous imaging was available for comparison. However, computed tomography (CT) showed numerous, rounded, coarse calcifications scattered throughout the breasts, likely representing degenerating fibroadenomas, consistent with the nodules on chest radiography. Mammography confirmed these findings (Figure 2).
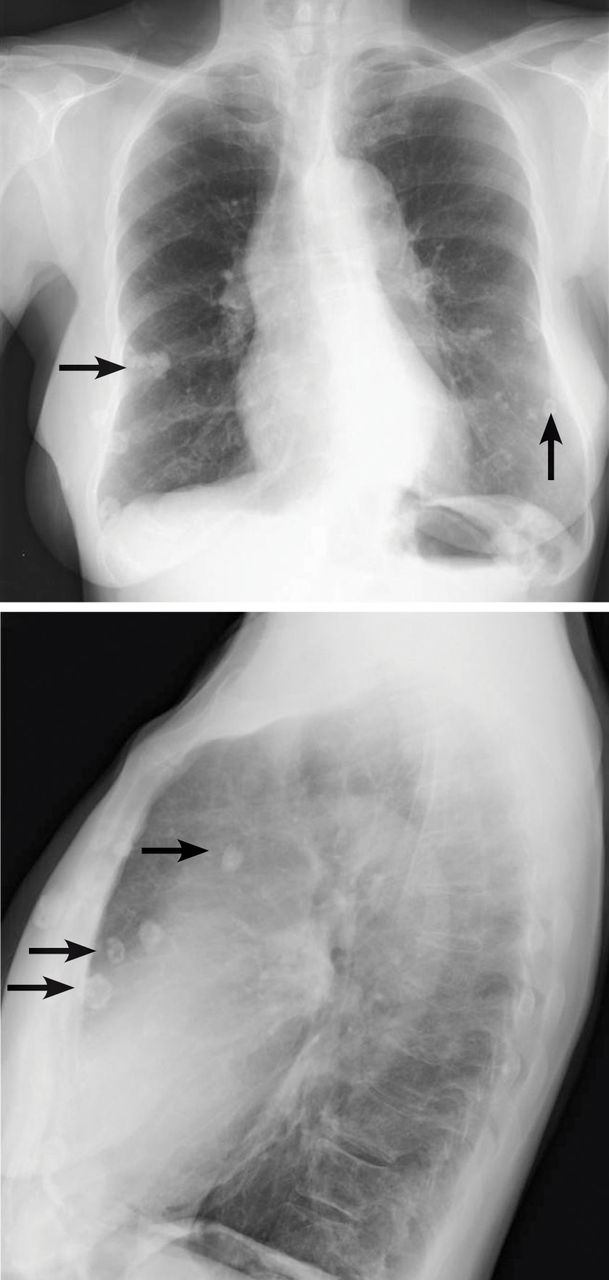
Chest radiography frontal and lateral views showed lesions suggesting pulmonary nodules.
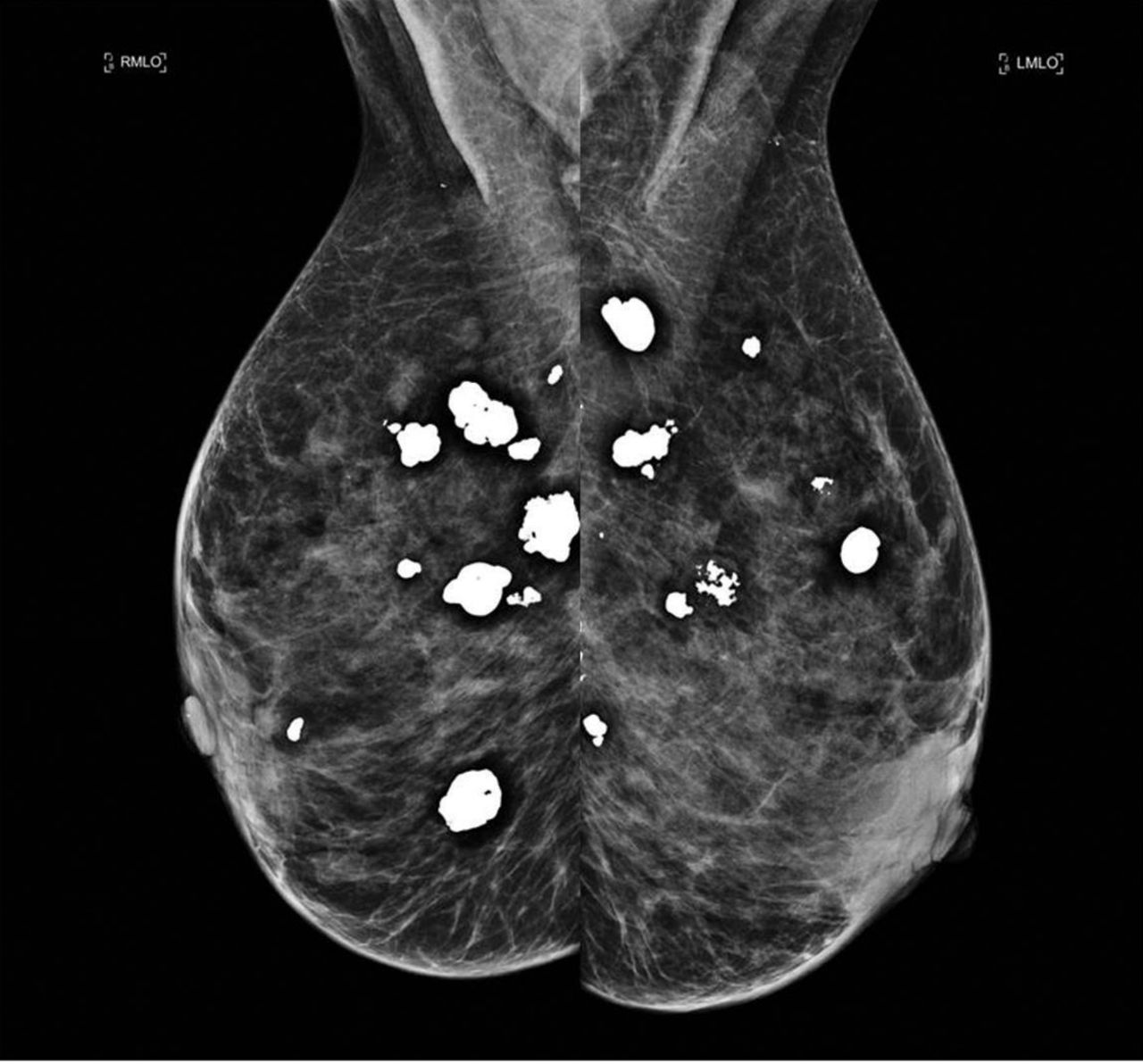
Mammography confirmed the presence of lesions in both breasts.
BREAST CALCIFICATIONS CAN MIMIC PULMONARY NODULES
Diffuse bilateral calcifications on mammography are typically benign and represent either dermal calcification (spherical lucent-centered calcification that develops from a degenerative metaplastic process) or fibro-cystic changes.1 Up to 10% of women have fibroadenomas, and 19% of fibroadenomas have microcalcifications.2–4 Therefore, given the high prevalence, calcified breast masses should be considered in the differential diagnosis when evaluating initial chest radiographs in women.
Calcifications in the breast can overlie the lung fields and mimic pulmonary nodules. When assessing pulmonary nodules, prior imaging of the chest should always be assessed if available to determine if a lesion is new or has remained stable.
Given our patient’s age and 35-pack-year history of smoking, apparent pulmonary lesions caused concern and prompted chest CT to clarify the diagnosis. However, if the patient has no risk factors for lung malignancy, it can be safe to proceed with mammography.
By including breast calcifications in the differential diagnosis of apparent pulmonary nodules on chest radiography, the clinician can approach the case differently and in-quire about a history of fibroadenomas and prior mammograms before pursuing a further workup. This can avoid unnecessary radiation exposure, the costs of CT, and apprehension in the patient raised by unwarranted concern for malignancy.
- Copyright © 2017 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.