


A 45-year-old man with known human immunodeficiency virus infection presented with a 5-day history of dyspnea. When his dyspnea had become symptomatic, he had restarted his home dapsone prophylaxis, but his dyspnea had progressively worsened, and his urine became dark.
On presentation to our institution, he was tachycardic, tachypneic, hypoxic, and cyanotic (Figure 1). Chest radiography revealed multifocal bilateral airspace opacities. He was started on vancomycin and piperacillin-tazobactam for treatment of presumed pneumonia, and his dapsone was continued for prophylaxis against Pneumocystis jirovecii pneumonia.

The patient’s hands on presentation (top) and after treatment with intravenous methylene blue (bottom).
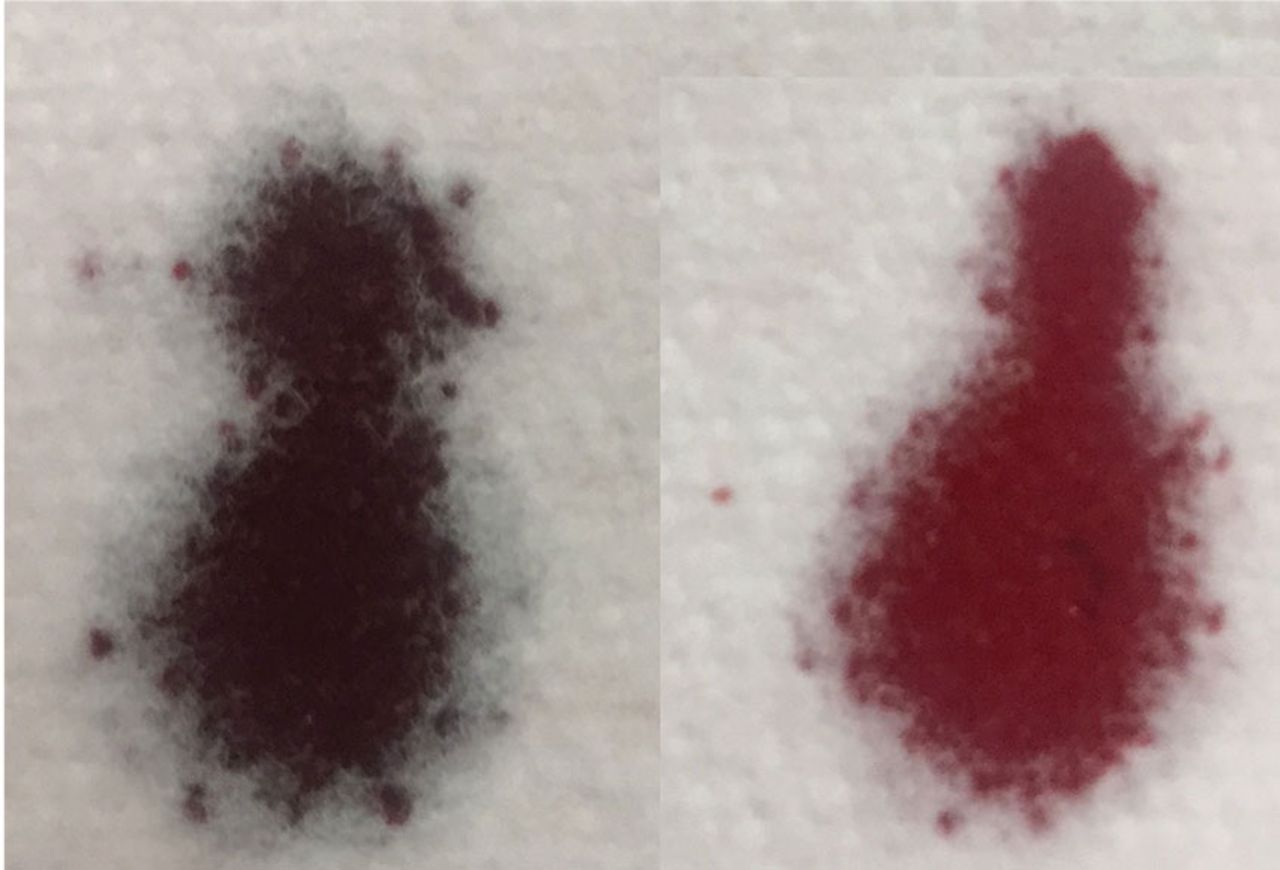
During the next several hours, his hypoxia worsened, and his peripheral capillary oxygen saturation was 87% despite use of a Venturi mask at a 35% fraction of inspired oxygen. Arterial blood gas testing revealed an elevated partial pressure of oxygen (143 mm Hg) and chocolate-brown colored arterial blood. Due to the low peripheral capillary oxygen saturation, high partial pressure of oxygen, and abnormal color of his blood (Figure 2), serum methemo-globin testing was ordered and revealed a concentration of 22.9% (normal value < 1.5%).

The patient’s arterial blood on presentation (left) compared with a sample of normal arterial blood (right).
Based on these test results, the patient’s dapsone was stopped and replaced with atovaquone. Intravenous infusion of methylene blue was started, with subsequent improvement of the hypoxia and cyanosis (Figure 1). His urine became green, but it returned to a normal color in a matter of hours. He was ultimately diagnosed with P jirovecii pneumonia and completed a course of atovaquone with total resolution of his symptoms.
THE MECHANISMS BEHIND METHEMOGLOBINEMIA
Heme iron is normally in the ferrous state (Fe2+), which allows for hemoglobin to carry oxygen and release it to tissues.1 Exposure to an oxidative stress can lead to methemoglobin-emia from an increase in abnormal hemoglobin that contains iron in a ferric state (Fe3+).1,2
Methemoglobin reduces oxygen-carrying capacity in two ways: it is unable to carry oxygen, and its presence shifts the oxy gen dissociation curve to the left, causing any remaining normal hemoglobin to be unable to release oxygen to the tissues.1,2
Causes of acquired methemoglobinemia include topical anesthetics (eg, benzocaine, lidocaine) and antibiotics (eg, dapsone).2,3 Signs and symptoms include cyanosis, headache, fatigue, dyspnea, lethargy, respiratory distress, and dark-colored urine.1,2
MANAGEMENT
Treatment consists of intravenous methylene blue, which reduces the hemoglobin from a ferric state to a ferrous state.1–4 Methylene blue is a water-soluble dye excreted primarily in the urine, and common side effects include dizziness, nausea, and green urine.5–7 The blue pigments from methylene blue combine with urobilin (a yellow pigment in the urine), producing a green color.7 This is not pathological and requires no treatment, as the urine returns to normal color after the body fully excretes the dye.5–7
If intravenous methylene blue fails to produce a response, other treatments to consider include hemodialysis, blood transfusion, exchange transfusion, and hyperbaric oxygen therapy.2
- Copyright © 2018 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.