


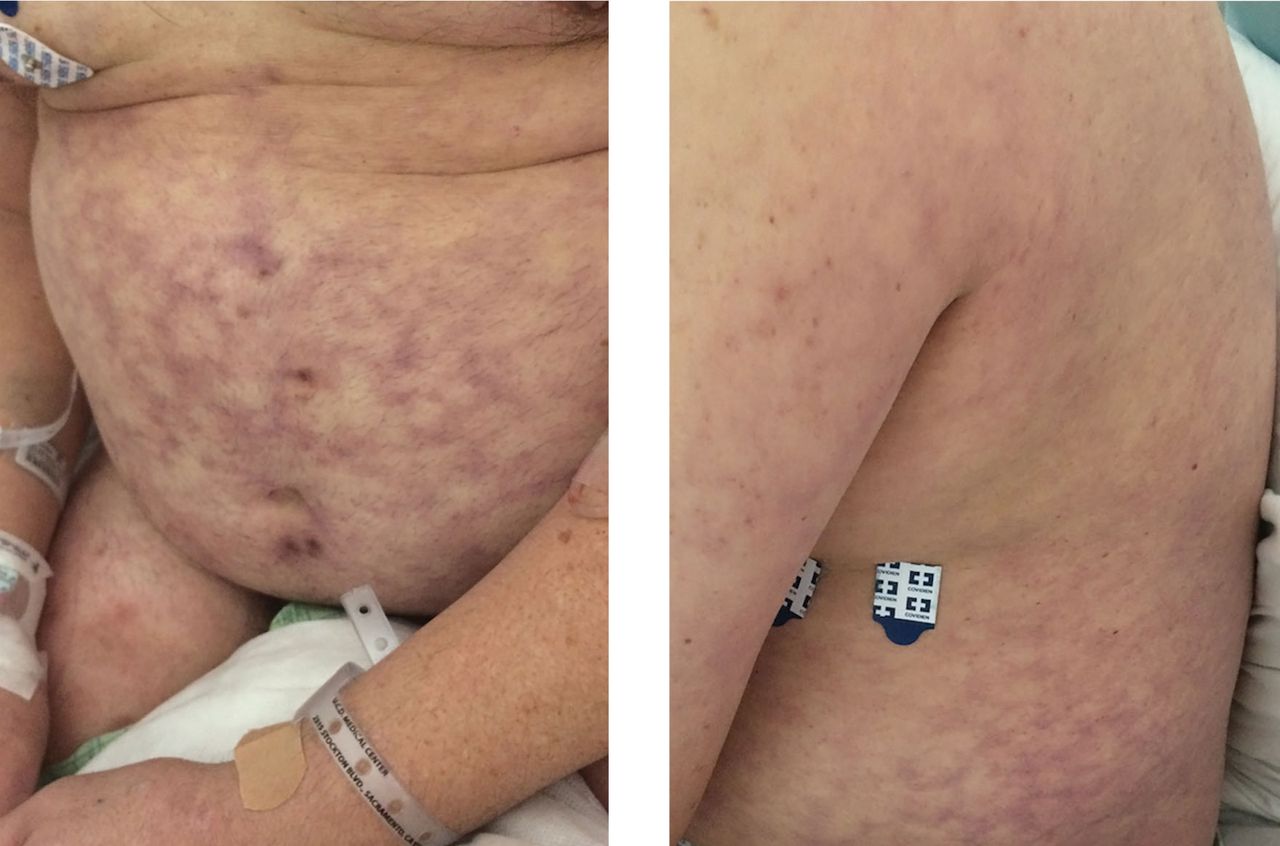
A 53-year-old man presented with acute altered mental status secondary to methamphetamine intoxication. On hospital day 2, he developed macular, violaceous skin lesions with interconnecting rings on his abdomen and back, consistent with livedo reticularis (Figure 1). The extensive distribution of the lesions on the abdomen raised concern for underlying disease.
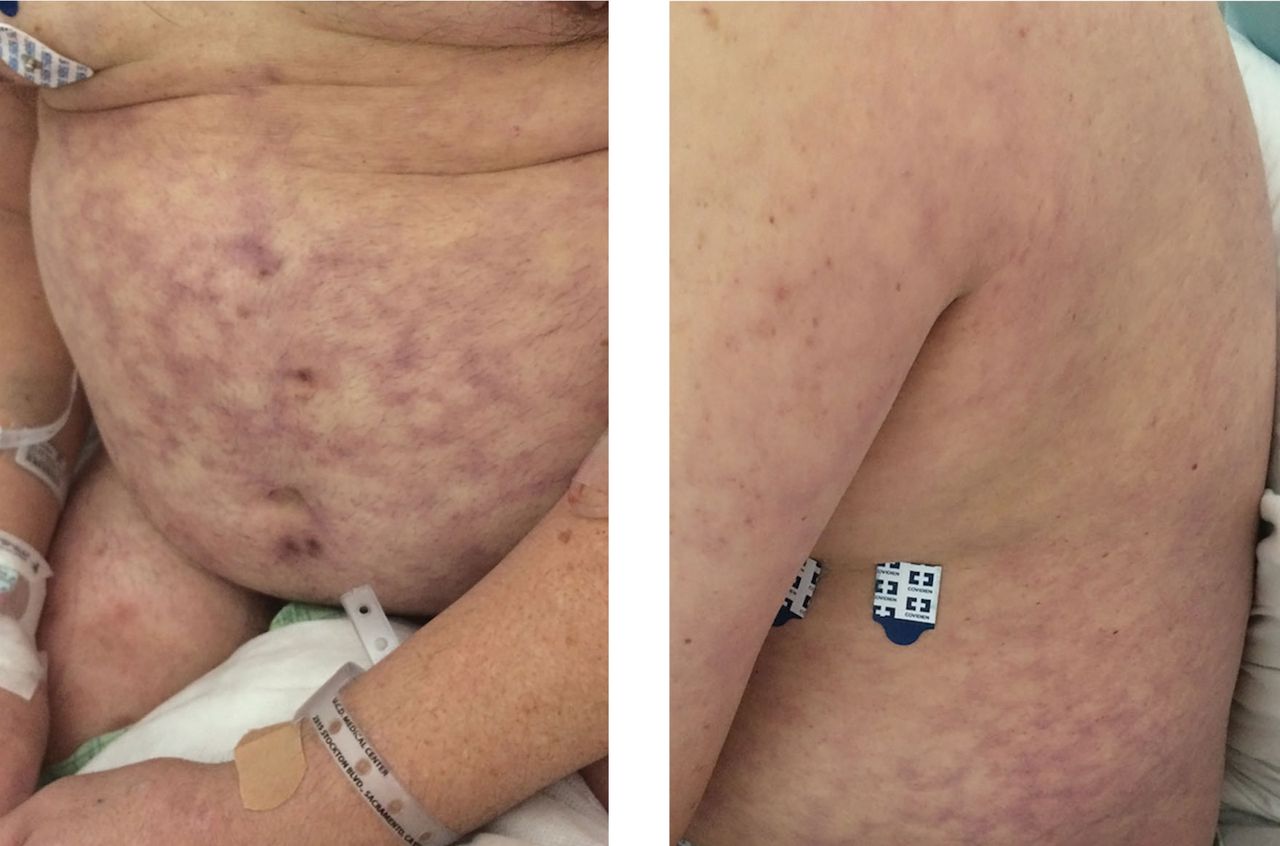
On hospital day 2, the patient developed macular, violaceous lesions with a reticular pattern on the abdomen and back. The extensive distribution of the lesions prompted an evaluation for an underlying systemic condition.
Livedo reticularis can be the manifestation of a wide range of conditions: hematologic and hypercoagulable states, embolic events, connective tissue disease, infection, vasculitis, malignancy, neurologic and endocrine conditions, and medication effects.1 Our patient had no recent history of vascular procedures or peripheral eosinophilia to suggest cholesterol embolization, and he had not recently started taking any new medications. His current medications included aspirin 81 mg, atorvastatin 40 mg, amlodipine 10 mg, and insulin glargine 20 units. Tests for cryoglobulin and antiphos-pholipid antibodies were negative. There was no evidence of malignancy, and evaluations for infectious and autoimmune diseases were negative.
Biopsy study of a skin lesion showed features consistent with livedo reticularis, with no evidence of vasculitis. The lesions resolved without definitive therapy by hospital day 3. This, in addition to other features of the lesions (eg, uniformity, unbroken reticular segments) and the extensive negative workup for systemic disease, suggested primary livedo re-ticularis.
CAUSES, TYPES, SUBTYPES
Livedo reticularis results from changes in the cutaneous microvasculature, composed of central arterioles that drain into an interconnecting, netlike venous plexus.1,2 Conditions such as arteriolar deoxygenation and venous plexus venodilation that result in a prominent venous plexus can give rise to clinical livedo reticularis.3
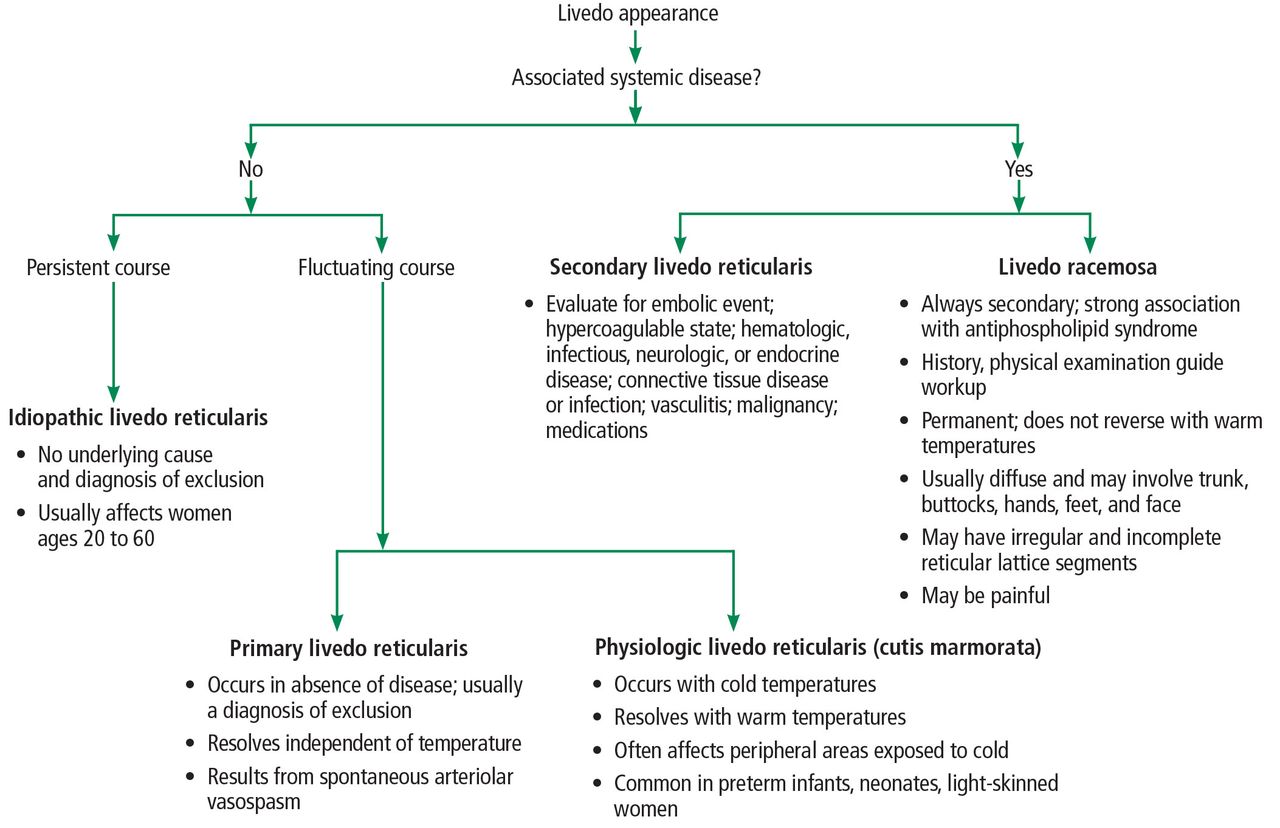
Livedo reticularis is divided into 2 broad categories depending on whether it is associated with systemic disease or not (Figure 2).3,4 In the absence of systemic symptoms, it can be further divided into 3 subcategories: idiopathic, physiologic, and primary.1 It is considered idiopathic if it is persistent, whereas physiologic and primary forms have a fluctuating course.4 Physiologic livedo reticularis often occurs in the periphery due to exposure to cold temperatures that cause vasospasm that resolves in warm temperatures.
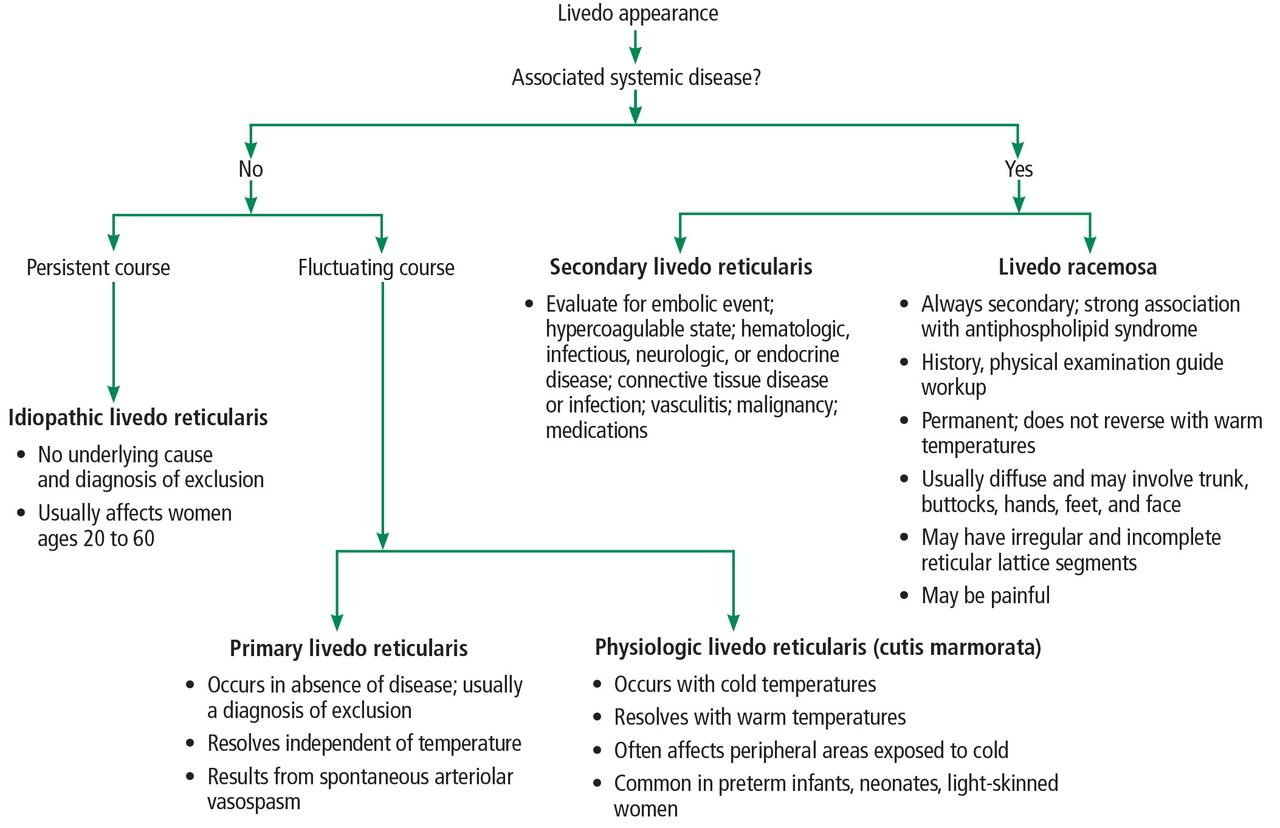
Algorithmic approach to the workup of livedo reticularis.
Primary livedo reticularis is thought to occur from spontaneous arteriolar vasospasm. It is a diagnosis of exclusion. An evaluation for underlying disease is important, as livedo re-ticularis can be associated with the range of conditions listed above.
In our patient, methamphetamine was considered a possible cause, but the findings of livedo reticularis were delayed and persisted longer than expected if they were drug-related.
Livedo racemosa
Distinguishing livedo reticularis from livedo racemosa is important. Livedo racemosa is always secondary and is often associated with an-tiphospholipid syndrome. It is present in 25% of cases of primary antiphospholipid syndrome and in up to 70% of cases of antiphospholipid syndrome associated with systemic lupus ery-thematosus.5 The reticular pattern of livedo racemosa is permanent and often has irregular and incomplete segments of reticular lattice, with a distribution that is more generalized, involving the trunk or buttocks (or both) in addition to the extremities.3,4 Consequently, a thorough history and physical examination are needed to guide additional workup.
- Copyright © 2018 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
{kind=link}