


Article Figures & Data
Figures
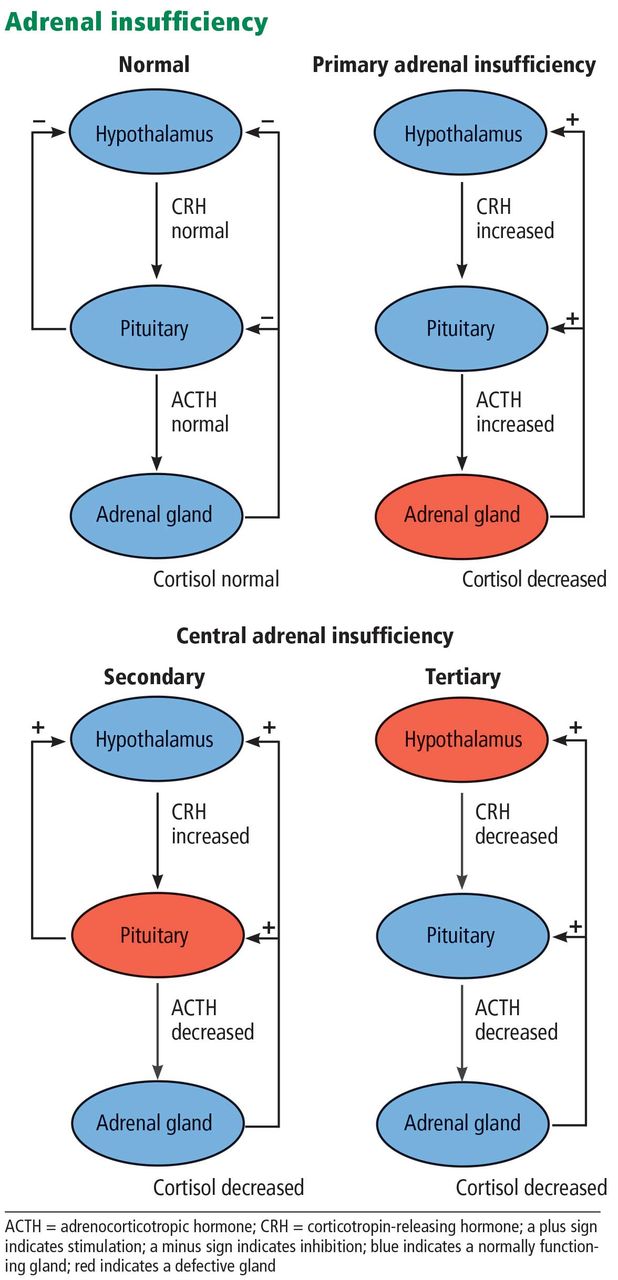
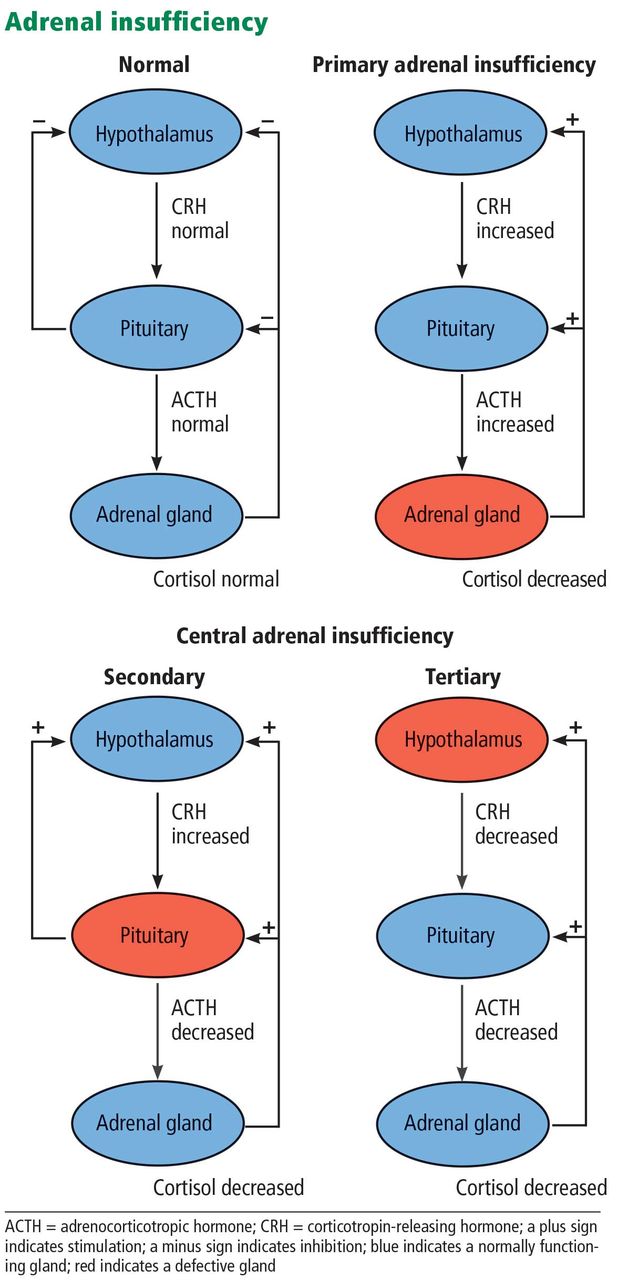
- Figure 1
Adrenal insufficiency is classified according to whether the defect lies in the adrenal gland (primary adrenal insufficiency) or centrally, ie, in the pituitary gland (secondary adrenal insufficiency) or hypothalamus (tertiary adrenal insufficiency).
Tables
Test Valuea Reference range Serum sodium 128 mmol/L 135–145 mmol/L Serum potassium 5.8 mmol/L 3.5–5.2 mmol/L Serum chloride 100 mmol/L 97–107 mmmol/L Serum creatinine 1.3 mg/dL 0.5–1.1 mg/dL Blood urea nitrogen 35 mg/dL 7–20 mg/dL Serum glucose (random, not fasting) 194 mg/dL 70–140 mg/dL Alanine aminotransferase 18 IU/L 7–35 IU/L Serum albumin 4.0 g/dL 3.5–5.5 g/dL Hemoglobin 10.1 g/dL 12.3–15.3 g/dL Mean corpuscular volume 85 fl 80–100 fl Mean corpuscular hemoglobin 28 pg/cell 26–34 pg/cell Mean corpuscular hemoglobin concentration 32.5 g/dL 31–36 g/dL White blood cell count 11.0 × 109/L 4.5–11.0 × 109/L Neutrophils 67% 40%–75% Lymphocytes 24% 20%–45% Monocytes 3.5% 2%–10% Eosinophils 5.0% 1%–6% Basophils 0.5% 0%–1% Platelet count 220 × 109/L 150–400 × 109/L International normalized ratio 6.13 2.0–3.0b Partial thromboplastin time 35 seconds 30–40 seconds Arterial partial pressure of oxygen 76 mm Hg 78–84 mm Hg (predicted for age) Oxygen saturation 94% Arterial partial pressure of carbon dioxide 30 mm Hg 35–45 mm Hg Serum bicarbonate 18 mmol/L 22–26 mmol/L Blood pH 7.34 7.35–7.45 General
Fatigue, generalized weakness
Muscle weakness
Muscle and joint pain
Loss of appetite
Weight loss
FeverbGastrointestinal
Nausea and vomiting
Abdominal pain
Acute abdomen with tenderness and rigidityb
Constipation or diarrhea
Salt cravingcDermatologic
Hyperpigmentation of skin, mucous membranes, hair, and nailsc
Vitiligoc
Dry, itchy skin
Auricular cartilage calcification (males)Cardiovascular
Shockb
Intravascular volume depletion
Hypotension/orthostatic hypotension
Tachycardia/orthostatic tachycardia
TachypneaNeuropsychiatric
Dizziness, postural dizziness
Depressiond
Memory impairmentd
Psychosis (rare)d
Confusionb
Decreased level of consciousnessbReproductive (women):
Decreased axillary and pubic hair
Decreased libido
AmenorrheaEndocrine
Autoimmune endocrine disorders,c eg, hypothyroidism
Other pituitary hormonal abnormalitieseAdrenal necrosis due to:
Adrenal hemorrhage
Sepsis
Emboli
Blunt traumaSudden withdrawal of corticosteroids in a patient who is steroid-dependent Deterioration of previously undiagnosed adrenal insufficiency after major stress, eg, severe infection Failure to increase corticosteroid dosage in steroid-dependent patients on days of major stress, eg, severe infection, surgerya Acute secondary or tertiary adrenal insufficiency, eg, pituitary apoplexy ↵a Some animal studies suggest that continuing the maintenance dose of glucocorticoids is adequate to prevent adrenal crisis. It is common practice to provide stress doses of glucocorticoids during an acute illness.
Hyponatremia Hyperkalemiaa Hypercalcemia Hypoglycemia Normal anion gap metabolic acidosisa Azotemia (prerenal)a Anemia (normochromic normocytic) Relative lymphocytosis Eosinophilia Mild elevation in serum thyroid-stimulating hormone Autoantibodies against 21-hydroxylase antigena ↵a May be present only in primary adrenal insufficiency.
- TABLE 5
Clinical features of primary vs central (secondary, tertiary) adrenal insufficiency
Feature Primary Central Possible explanation for difference Skin hyperpigmentation Yes No Adrenocorticotropic hormone production and thus melanocyte-stimulating hormone levels are increased in primary but not central adrenal insufficiency Gastrointestinal symptoms More prominent Less prominent More prominent electrolyte disturbances in primary adrenal insufficiency may play a role in gastrointestinal symptoms Intravascular volume depletion, hypotension More prominent Less prominenta Decreased serum aldosterone levels only in primary adrenal insufficiency Hyperkalemia Yes No Decreased serum aldosterone levels only in primary adrenal insufficiency Hypoglycemia Less prominent More prominent Concomitant growth hormone deficiency present in some cases of central adrenal insufficiency
More insidious progression in central adrenal insufficiency resulting in delayed presentation and more prominent corticosteroid deficiency symptoms such as hypoglycemiaBlood urea nitrogen elevation More frequent Less frequent Intravascular volume depletion resulting in prerenal azotemia is present more frequently in primary adrenal insufficiency Hypopituitarism, headaches, visual field defects No Yes Depends on the underlying cause ↵a Secondary adrenal insufficiency such as pituitary apoplexy may present with hypotension and, if not treated, may lead to azotemia. However, this may occur much more frequently in patients with primary adrenal insufficiency.




{kind=link}
Jump to section
- Article
- INITIAL EVALUATION AND MANAGEMENT
- DIFFERENTIAL DIAGNOSIS
- CASE CONTINUED: CARDIOMEGALY, PERSISTENT HYPOTENSION
- PROMPT MANAGEMENT OF ADRENAL CRISIS
- CASE RESUMED: IMPROVEMENT WITH HYDROCORTISONE
- ESTABLISHING THE DIAGNOSIS OF ADRENAL INSUFFICIENCY
- CASE RESUMED: PATIENT DISCHARGED, LOST TO FOLLOW-UP
- MINERALOCORTICOID VS CORTICOSTEROID DEFICIENCY
- TAKE-HOME POINTS
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.