


Article Figures & Data
Figures
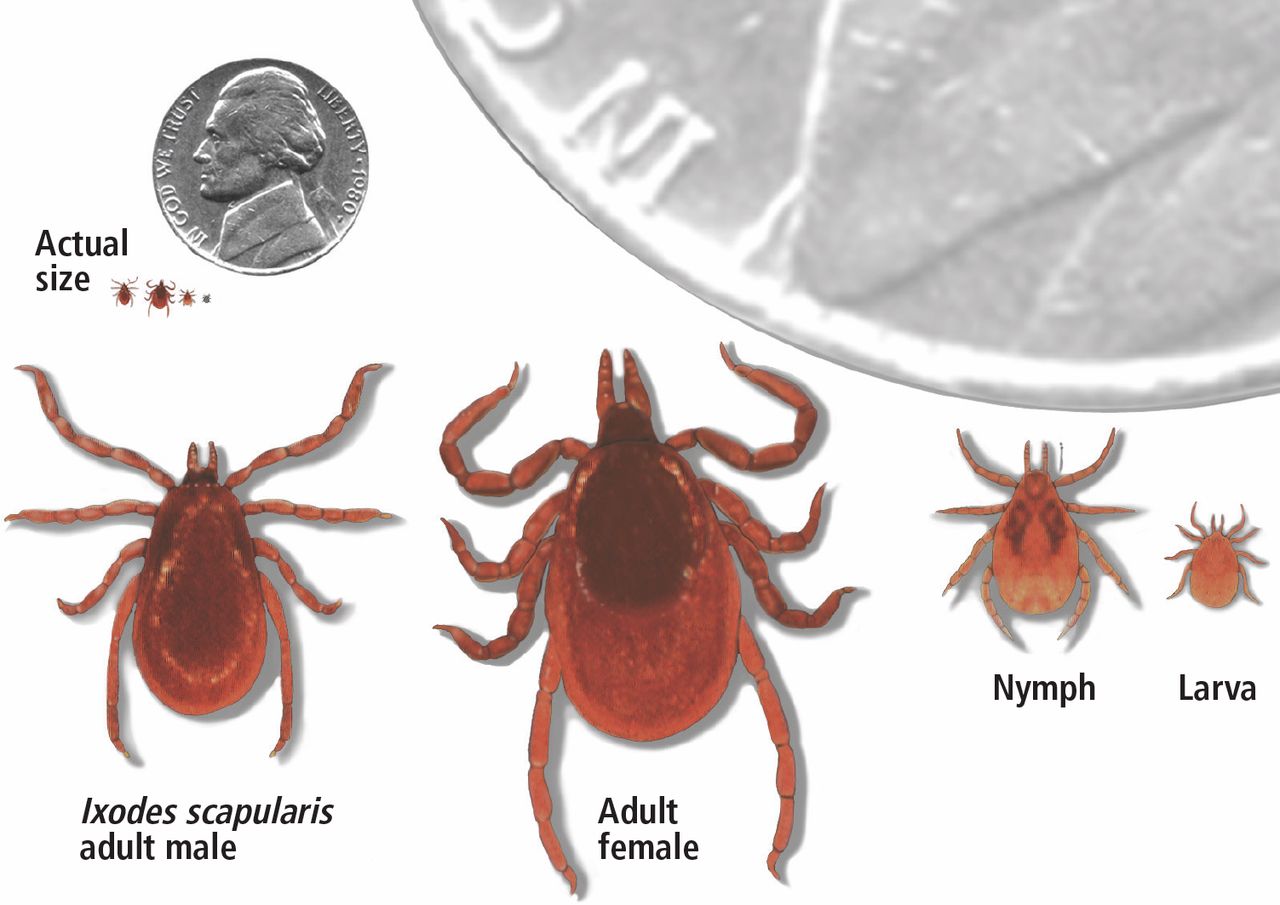
- Figure 1
Ixodes scapularis is the vector of Lyme disease in the eastern United States. Infected nymphs account for most cases.
From Sigal LH. Myths and facts about Lyme disease. Cleve Clin J Med 1997; 64(4):203–209. doi:10.3949/ccjm.64.4.203
- Figure 2
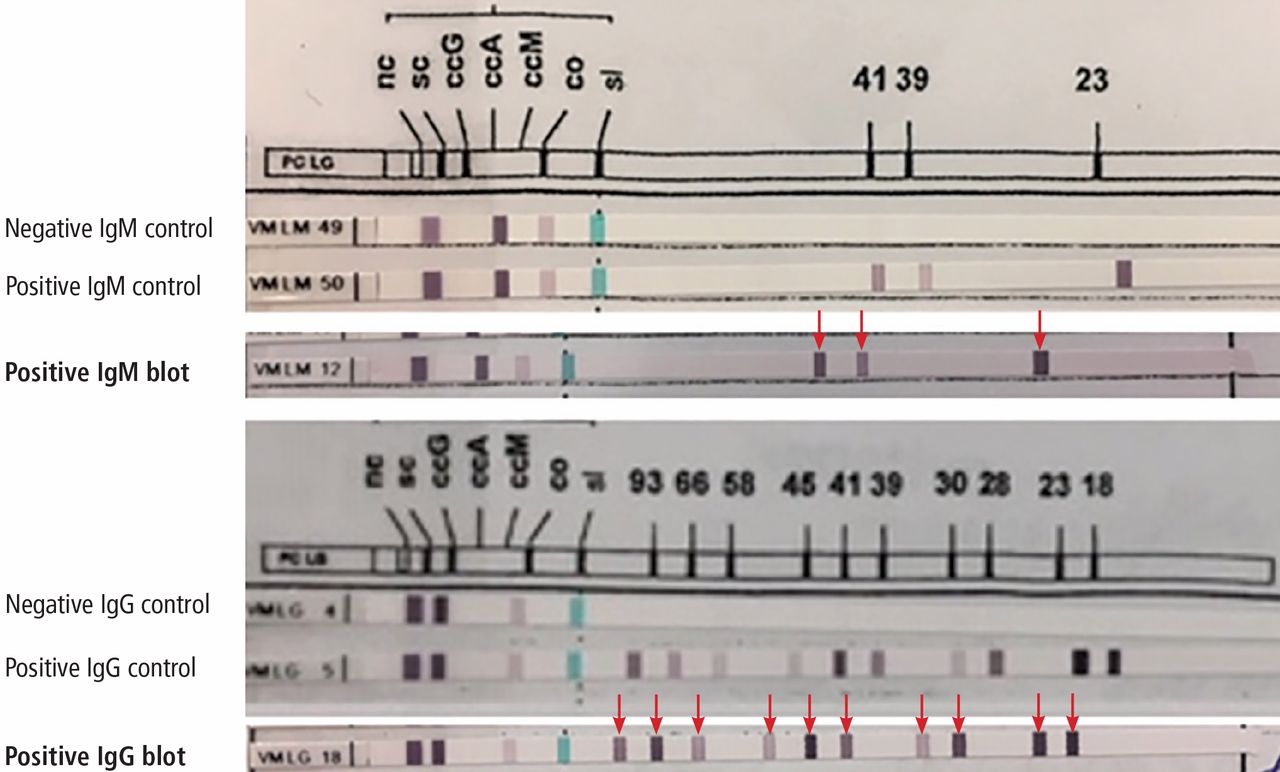
Positive Western blot test (Borrelia B31 ViraStripe [Viramed Diagnostics]) in a patient who presented with rash and arthritis. This test uses purified specific antigens of strain B31 of Borrelia burgdorferi sensu stricto. Note that the patient has 3 of 3 IgM bands and 10 of 10 IgG bands (arrows).
- Figure 3
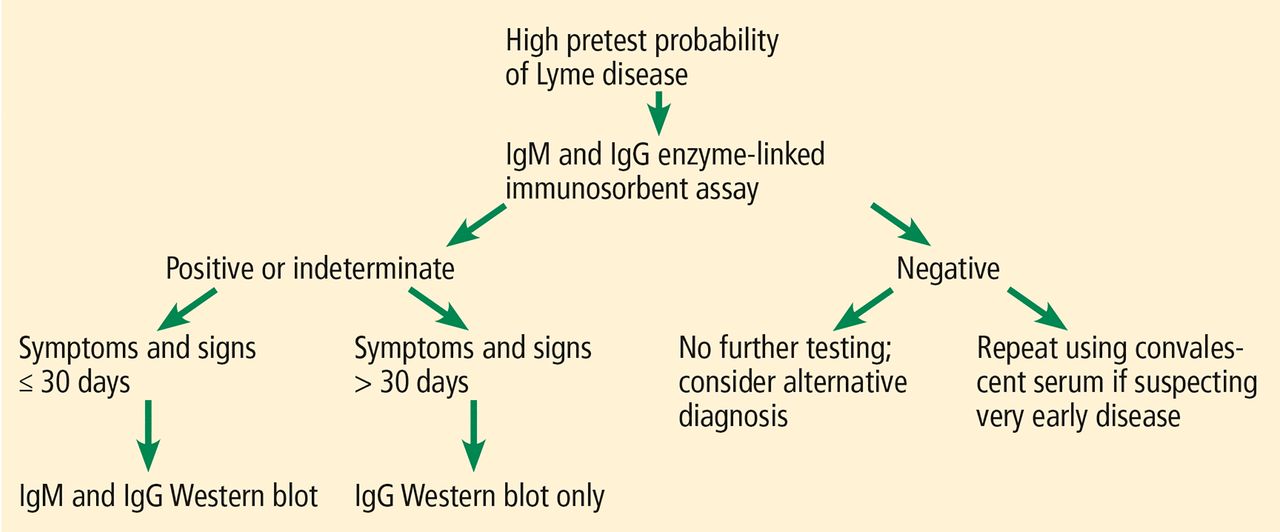
Standard 2-tier testing for Lyme disease. Ig = immunoglobulin.

Tables
State Confirmed cases per 100,000 persons 1 Maine 89.2 2 Vermont 86.7 3 Pennsylvania 66.7 4 Rhode Island 53.4 5 New Hampshire 51.9 6 Connecticut 41.8 7 New Jersey 40.5 8 Delaware 40.0 9 Wisconsin 26.6 10 Minnesota 23.4 11 Maryland 20.6 12 Massachusetts 16.6 13 New York 15.8 14 Virginia 12.3 15 Washington, DC 10.1 Data from reference 2.
Direct methods Borrelia culture Polymerase chain reaction Indirect methods Immunofluorescent assay Enzyme-linked immunosorbent assay Western blot - TABLE 3
Causes of false-positive enzyme-linked immunosorbent assay testing for Lyme disease
Infections Bacterial infection Infective endocarditis Other borrelial disease (eg, relapsing fever) Other spirochetal infection (eg, syphilis, leptospirosis) Viral infection Epstein-Barr virus (polyclonal antibody production) Parasitic infection Malaria (polyclonal antibody production) Noninfectious causes Autoimmune conditions Systemic lupus erythematosus Rheumatoid arthritis Antibody Antigen (molecular mass) Positive test Immunoglobulin M OspC (24 kDa)a 2 of 3 bands BmpA (39 kDa) Fla (41 kDa) Immunoglobulin G OspC (18, 21 kDa)b 5 of 10 bands BmpA (28, 30, 39 kDa) Fla (41, 45, 58, 66, 93 kDa) ↵a The apparent molecular mass of OspC depends on the strain of Borrelia burgdorferi being tested. The 24 and 21 kDa proteins are the same.
Based on information in reference 16.
Stage of illness Clinical features Primary testing recommended Additional testing Stage 1 Early localized disease
(< 4 weeks)
Erythema migransNo serologic testing Stage 2 Early disseminated disease
Lymphocytic meningitis Facial palsy
Radiculoneuropathy or carditisTwo-tiered testing
If initial test is negative, useacute and convalescent phase serologyStage 3 Late Lyme disease (> 4 weeks)
Lyme arthritisTwo-tiered testing Synovial fluid polymerase chain reaction (PCR) if no improvement after 2 months of oral antibiotics Lyme neuroborreliosis Cerebrospinal fluid (CSF) anti-bodies and 2-tiered testing CSF PCR or CSF culture




{kind=link}
{kind=link}
{kind=link}