


Article Figures & Data
Figures
- Figure 1
Silicone breast implants. Left, textured and anatomically shaped; right, smooth and round. Note the sloping projection of the anatomic implant. The fuller portion would be oriented inferiorly in the patient to simulate a native breast shape.
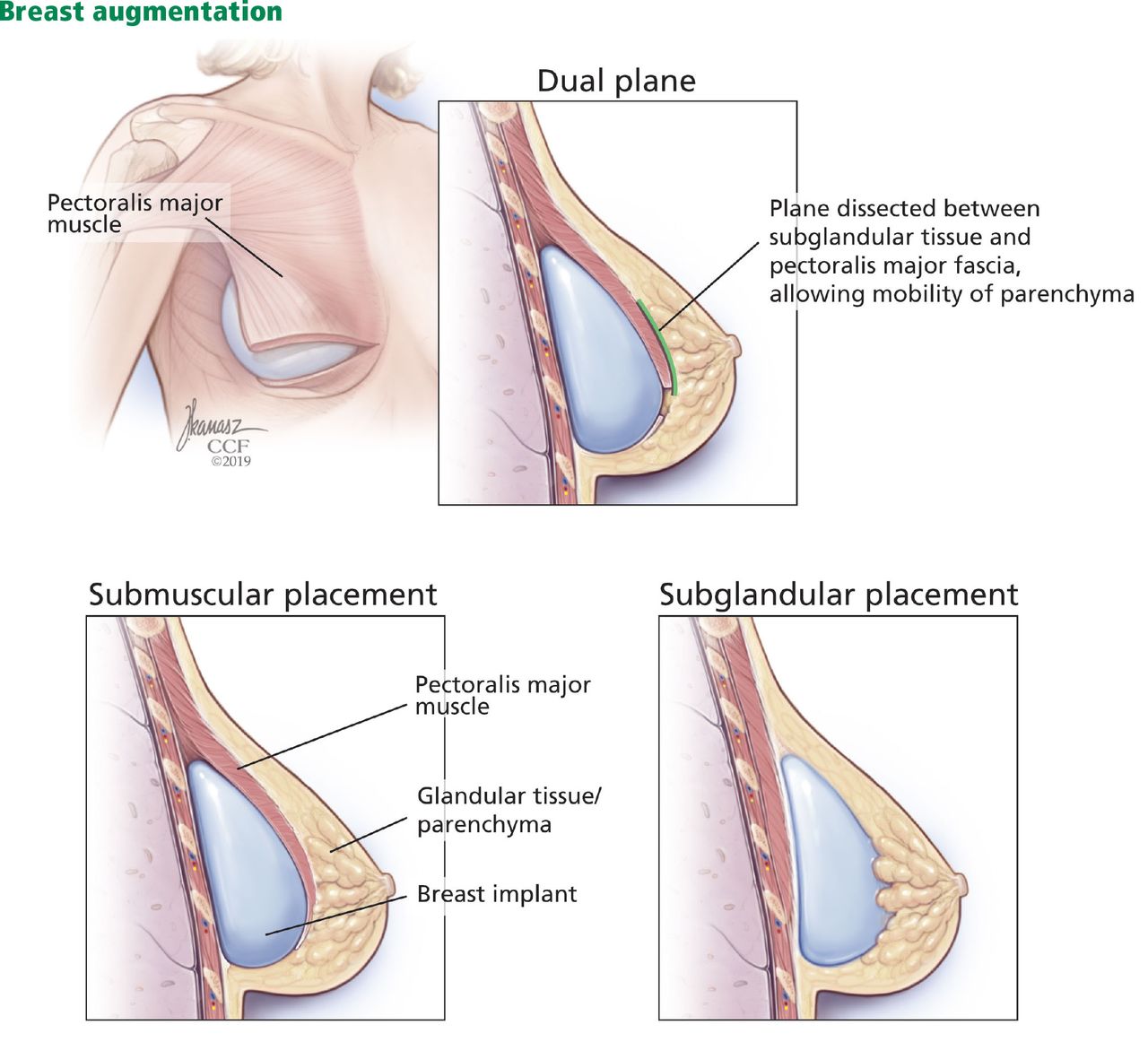
- Figure 2
Placement of breast implants.
- Figure 3
The images in the top row are before breast augmentation. Those in the bottom row are 7 months after breast augmentation surgery with 350-cc smooth, round silicone breast implants placed via an inframammary incision in a subpectoral pocket.



Tables
First generation (1960s) Shell Thick, smooth, silicone elastomer in 2 pieces with Dacron patches posteriorly to facilitate positioning along the chest wall Filler Silicone gel, moderate viscosity Shape Anatomic or “teardrop” Complications High capsular contracture rate (approached 100% at 10 years after implantation) Second generation (1970s)a Shell Thinner, smooth, seamless, no Dacron patches Filler Silicone gel, thinner and less viscous Shape Round Complications Rupture (nearly 60%), diffusion or “bleeding” of silicone molecules into periprosthetic space and onto breast implant capsule Third generation (1980s)b Shell Thicker, multilayer silicone elastomer, no Dacron patches Filler Silicone gel with larger particles, increased crosslinking, more viscous and thick Fourth and fifth generation (1990s to present)c Shell and filler Shell thickness and gel viscosity redesigned according to strict criteria by American Society for Testing Methodology and US Food and Drug Administration Shape Anatomic (teardrop) ↵a During this period subpectoral implant placement gained popularity, decreasing capsular contracture rates.
↵b Restricted from US market temporarily in 1992; textured surfaces were introduced during this period in an effort to decrease capsular contracture.
↵c Greater quality control during manufacturing; wider variety of implant shapes and surface texturing available.
Advantages Disadvantages Silicone Consistency with palpation mimics dense, natural breast tissue
Quicker adjustment to alterations in the external environmentExposure to silicone in the event of rupture, and rupture not immediately evident
Higher initial cost (nearly double that of saline implants), including cost of recommended monitoring (imaging) to ensure implant integritySaline Only a small incision is required for implant insertion (implant filled with saline to desired volume through a port)
Saline is safely absorbed by the body in the event of rupture, and rupture is immediately evident (breast deflation)
No concern for silicone exposure in the event of ruptureOverfilling leads to increased firmness, palpability of the implant edge
Underfilling results in rippling and a higher risk of rupture from the shell folding upon itself
Consistency with palpation mimics water (as opposed to natural breast tissue)
Slow to adjust to alterations in the external environment (eg, feels cold after swimming)
Slightly higher rate of ruptureLocation Advantages Disadvantages Inframammary Most common choice
Excellent visualization of both the subpectoral and suprapectoral planes of dissectionVisible scar along inferior pole of the breast Periareolar Excellent exposure of the implant pocket
Less sensory deficit to lower breast polePotentially higher rate of capsular contracture
Associated with moderate-severe implant malposition and increased risk for secondary procedures
Greater propensity for nipple-areola complex dysesthesia
Scar located on visible breast surfaceTransaxillary Ideal for saline implants (only require small incisions)
Does not affect subsequent sentinel lymph node biopsies
High satisfaction rate vs inframmary incisionsDifficult route to place silicone implants
Associated with moderate to severe implant malposition and increased risk for secondary proceduresTransumbilical Remote incision, may be obscured by umbilicus Less control of implant positioning




{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- ABSTRACT
- EVOLUTION OF IMPLANTS
- CURRENT IMPLANT OPTIONS
- PATIENT ASSESSMENT
- ANTIBIOTICS
- PERIOPERATIVE PERIOD
- POSTOPERATIVE PERIOD
- IMPLANT LONGEVITY AND RUPTURE
- CAPSULAR CONTRACTURE
- ADDITIONAL COMPLICATIONS
- BREAST CANCER AND DETECTION
- AUTOIMMUNE DISEASES
- BREAST IMPLANT-ASSOCIATED ANAPLASTIC LARGE-CELL LYMPHOMA
- ARE PATIENTS HAPPIER AFTERWARD?
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.