


A 74-year-old man presented to the gastroenterology clinic with a 2-day history of retrosternal discomfort. His vital signs were normal, and laboratory testing showed a normal leukocyte count.
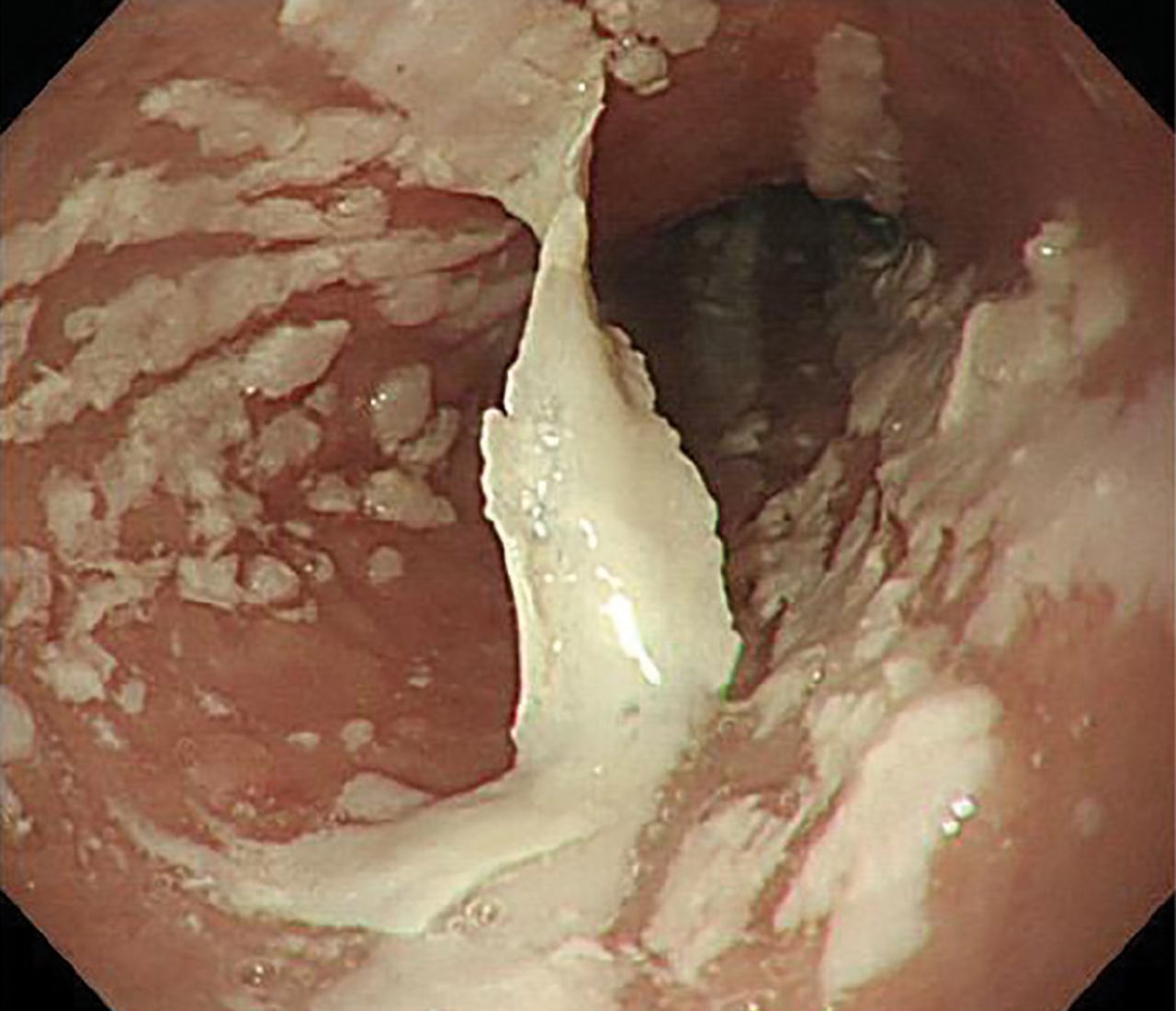
Esophagogastroduodenoscopy (EGD) revealed longitudinal sloughing mucosal casts in the middle and lower esophagus (Figure 1).

Endoscopy shows longitudinal sloughing mucosal casts in the middle and lower esophagus.
Esophageal candidiasis would be suspected on the basis of endoscopic findings of white or yellowish plaque-like lesions that could not be washed away.1 However, in this patient, the lesions were exfoliative, a picture compatible with chemical or “pill esophagitis.” The patient had no risk factors for esophageal candidiasis such as human immunodeficiency virus infection, alcohol abuse, or diabetes mellitus. Further, no Candida species were detected in EGD samples sent for microscopic study.
The patient had been taking dabigatran 110 mg twice daily for 2 years because of non-valvular atrial fibrillation. He was also taking amlodipine 2.5 mg/day for hypertension.
Risk factors and medications commonly associated with pill esophagitis are shown in Table 1. Further questioning of the patient revealed that he took his medications with very little water. Apixaban was prescribed as an alternative to dabigatran, in addition to the proton-pump inhibitor rabeprazole 10 mg/day. The symptoms disappeared within a few days.
Risk factors and medications associated with pill esophagitis
At follow-up 1 month later, EGD confirmed that the esophageal mucosa had completely healed (Figure 2).

Complete healing of the esophageal mucosa 1 month later.
DABIGATRAN-INDUCED ESOPHAGITIS
Dabigatran, an oral direct thrombin inhibitor, is widely used for thromboprophylaxis. Unlike other direct oral anticoagulants, it contains tartaric acid as an excipient, which reduces variability in the drug’s absorption. However, if the tablet gets stuck in the esophagus, the acid leaching out can damage the esophageal mucosa.
Although no study has investigated the overall prevalence of dabigatran-induced esophagitis, a retrospective database review of 91 patients taking dabigatran and undergoing upper-gastrointestinal endoscopy reported that 19 (20.9%) had endoscopic signs of dabigatran-induced esophagitis.2
Typical symptoms are the acute onset of chest pain, epigastralgia, odynophagia, and dysphagia. But patients can also have no symptoms or only mild symptoms.2,3
Despite dabigatran’s anticoagulant activity, there have been few reports of bleeding, perhaps because the lesions tend to be superficial on the surface of the esophageal mucosa.
Symptoms usually resolve within 1 week after stopping dabigatran and starting a proton pump inhibitor. To prevent mucosal injury, patients should be instructed to take dabigatran with sufficient water and to remain in an upright position for at least 30 minutes after-ward.4
- Copyright © 2019 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
{kind=link}