


Article Figures & Data
Figures
- Figure 1A
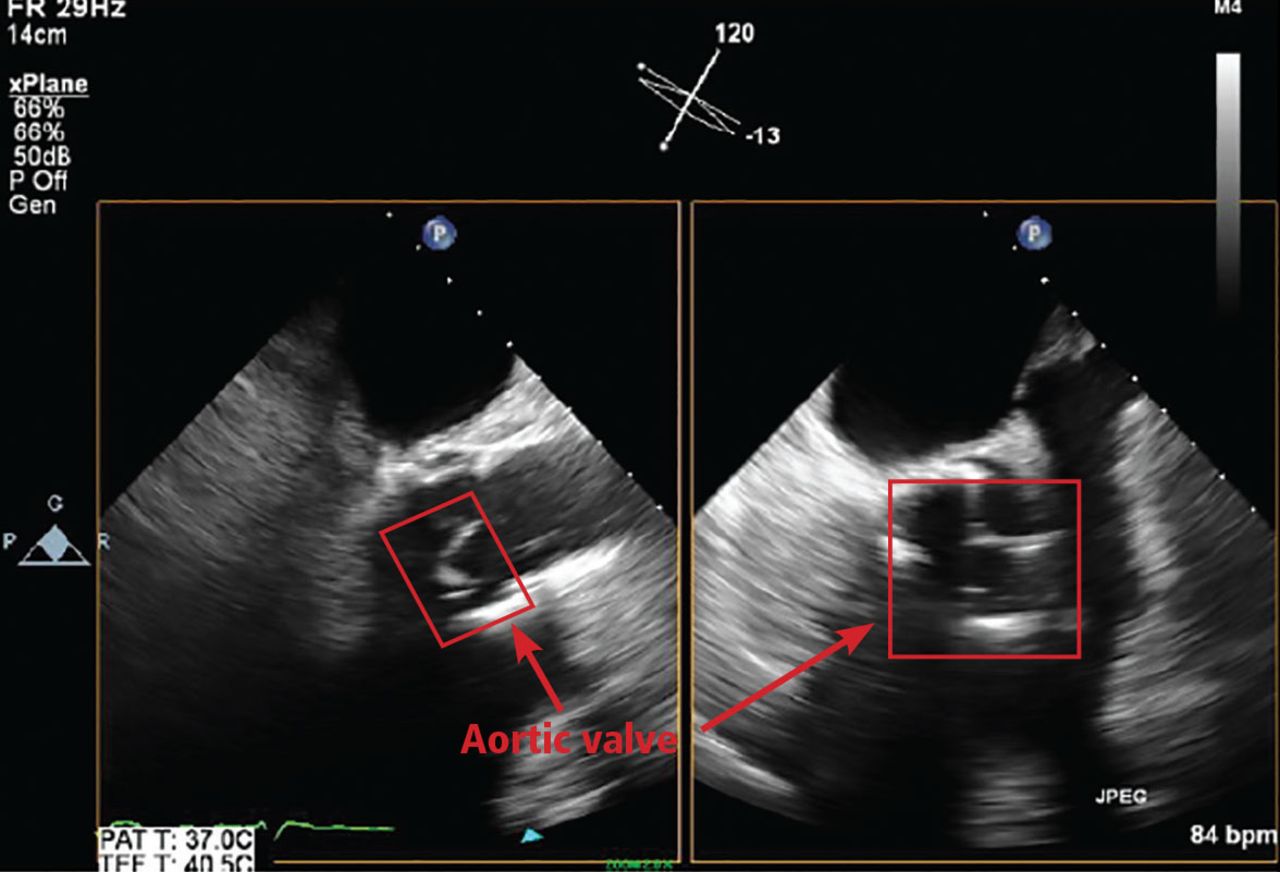
Transesophageal echocardiography in a 73-year-old man with a bioprosthetic aortic valve who presented with 2 months of fevers, chills, and night sweats. He had several negative blood cultures and 2 negative transesophageal echocardiograms over 1 month. No mass, vegetation, paravalvular abscess, or significant valve dysfunction was noted.
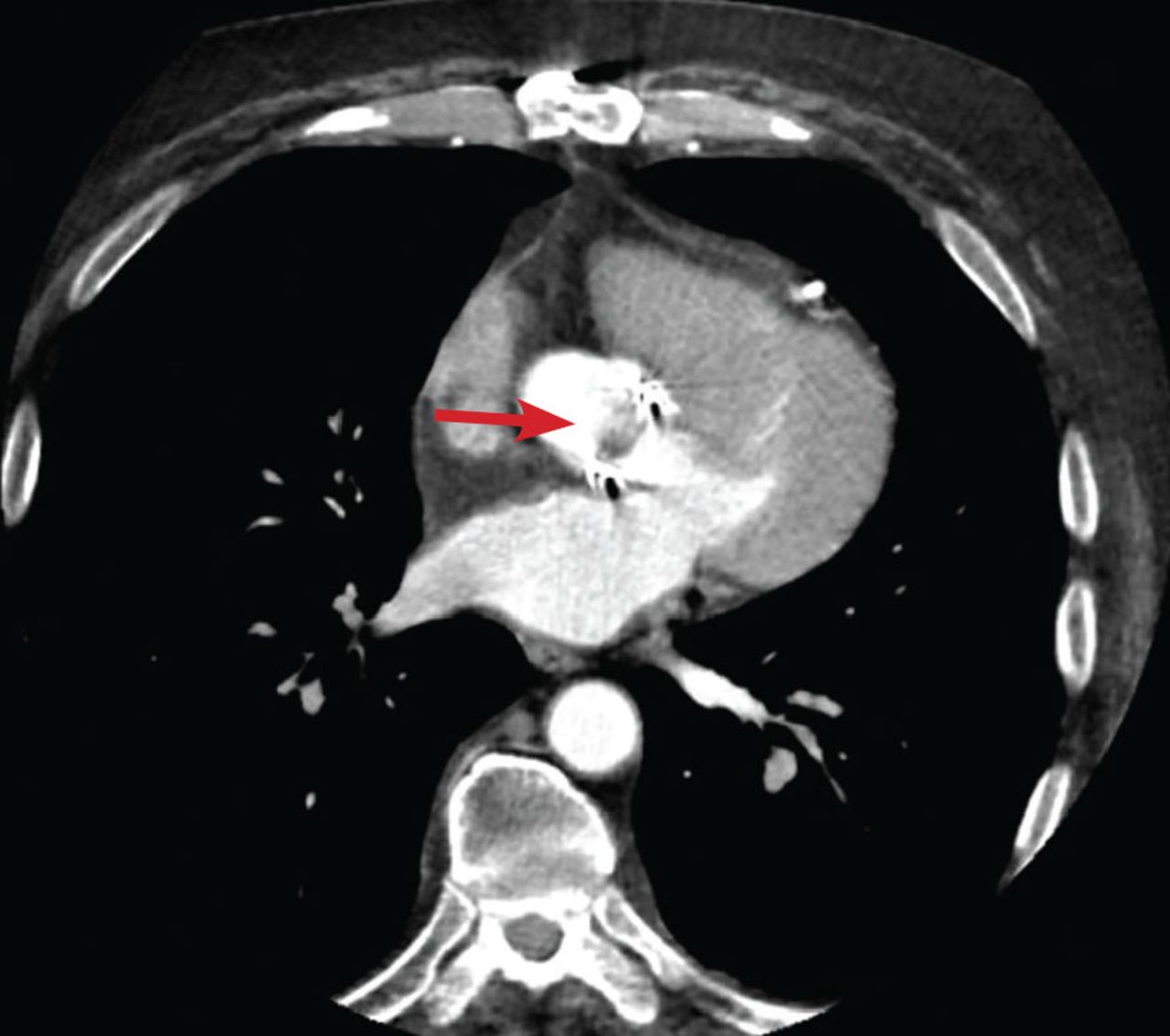
- Figure 1B
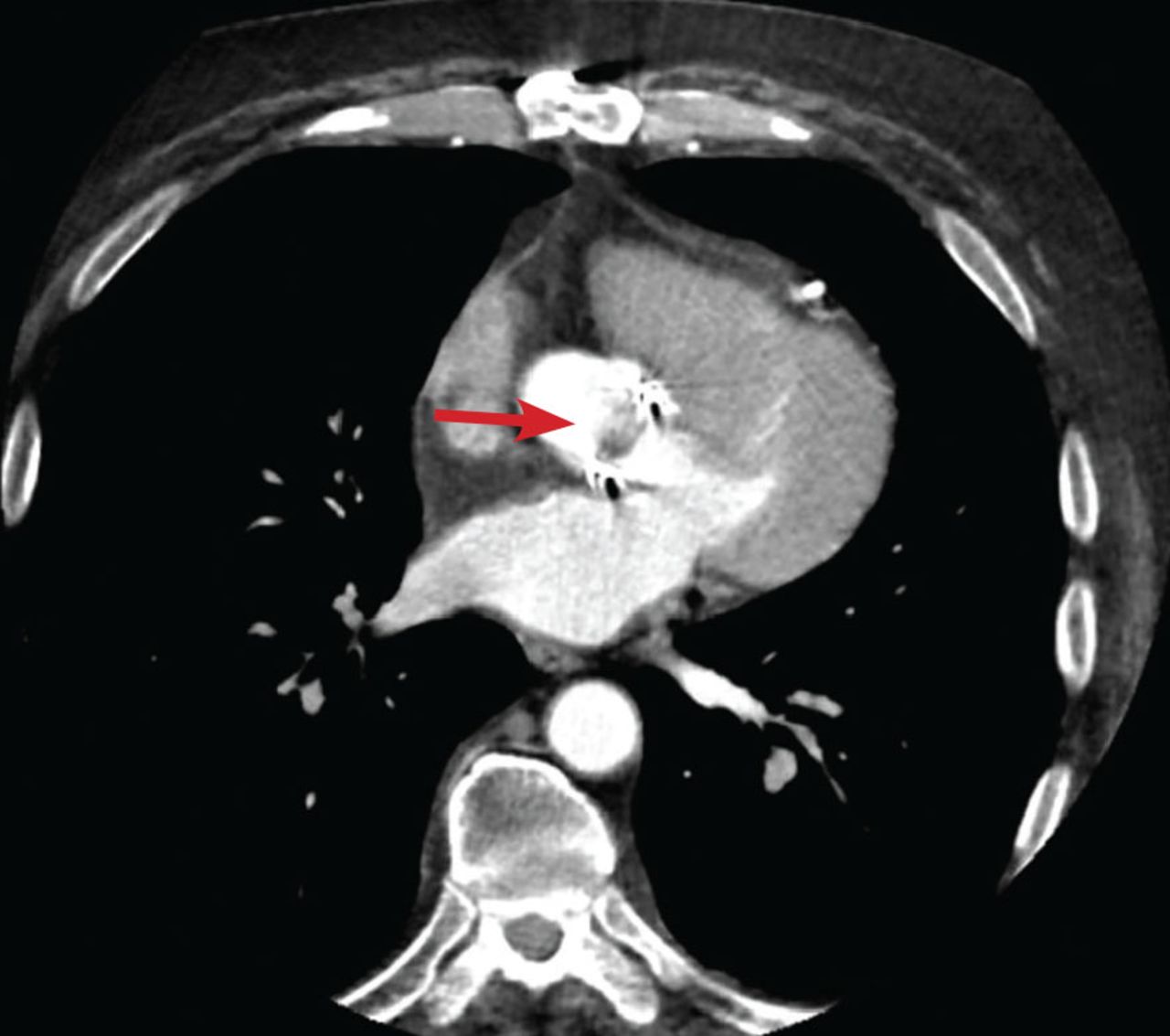
Cardiac computed tomographic (CT) angiography with iodinated contrast, including 4D reconstruction, in the same patient, however, shows an 11-mm vegetation on the bioprosthetic aortic valve leaflets (arrow).
- Figure 1C
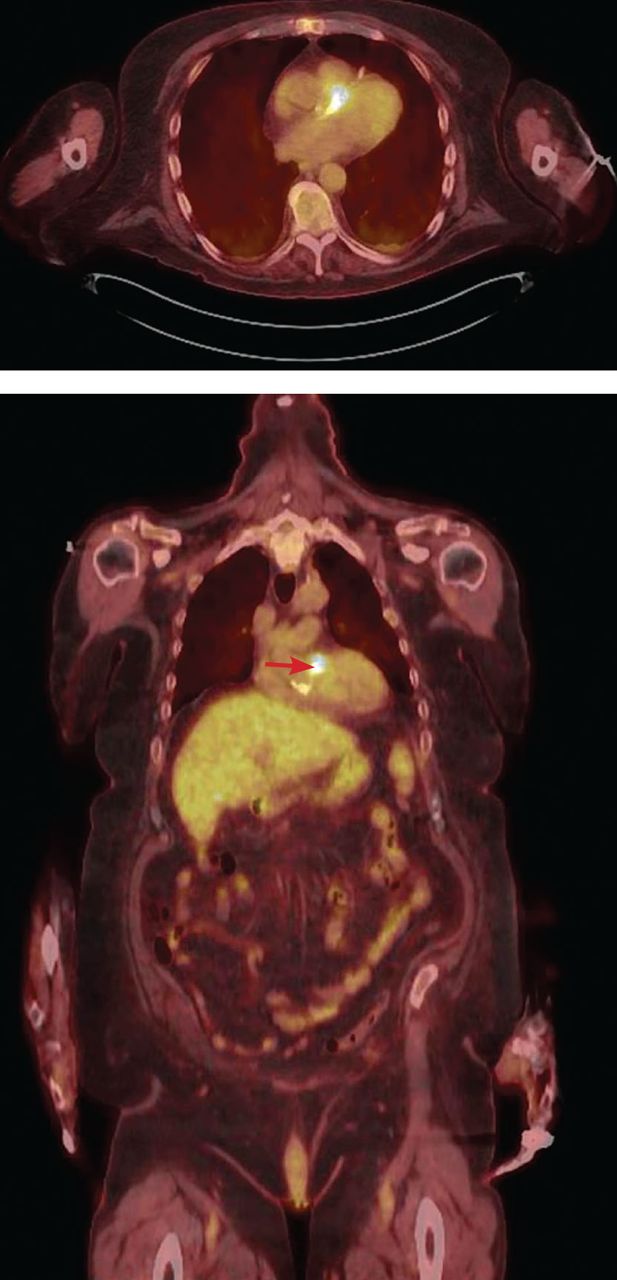
Fluorodeoxyglucose positron emission tomography (FDG-PET) in the same patient confirms the diagnosis, showing a 13-mm hypermetabolic focus on the prosthetic valve (arrow), yielding the diagnosis of infectious endocarditis.
- Figure 2
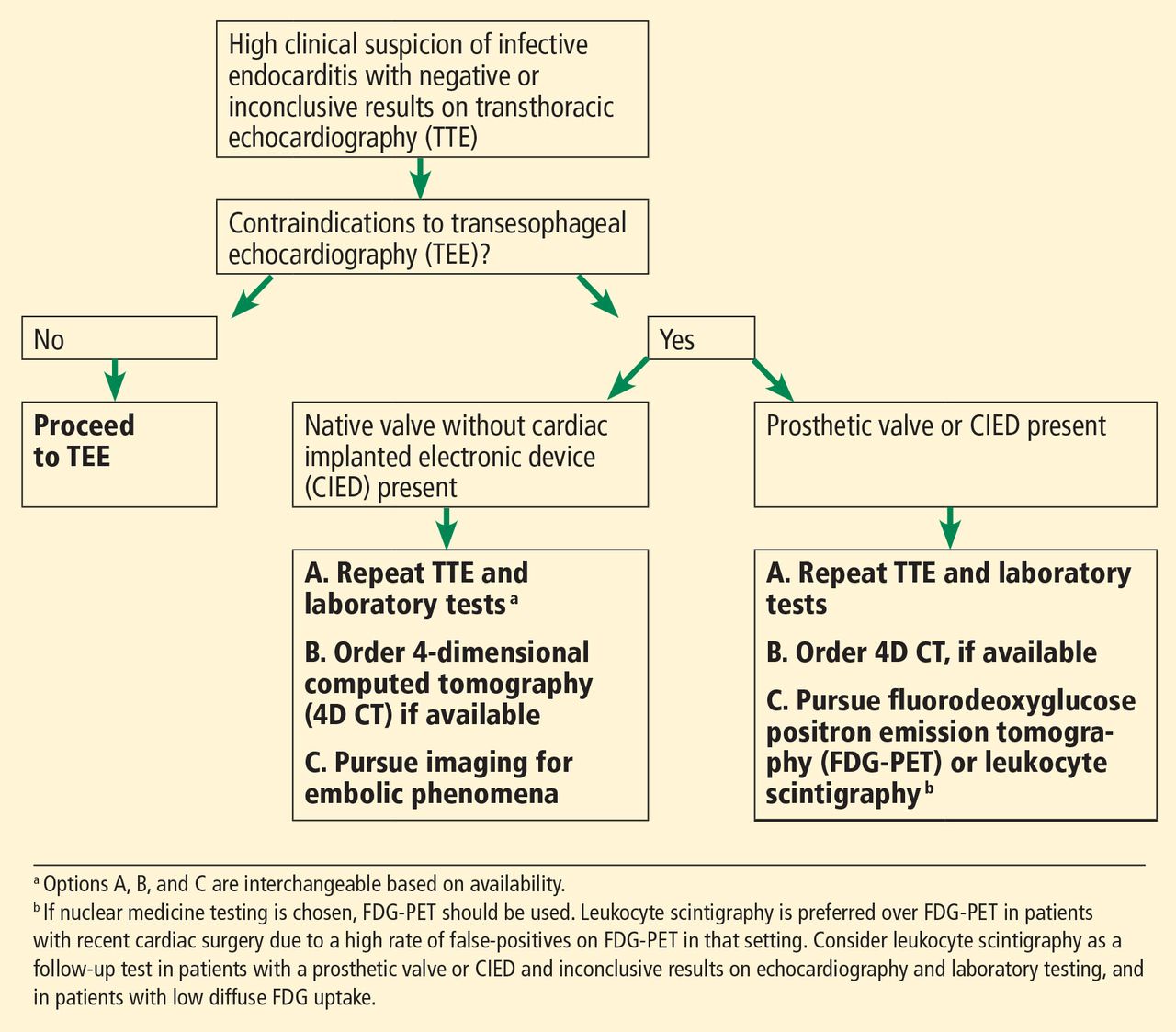
Suggested algorithm for evaluating suspected infective endocarditis with negative or inconclusive results on echocardiography.

Tables
Imaging test When to consider Advantages Limitations Transthoracic echocardiography (TTE) Suspected infective endocarditis in patients with risk factors Widely available
Relatively fast
Provides hemodynamic information
NoninvasiveDecreased sensitivity for abscesses
Can miss small vegetations
Limited sensitivity for prosthetic valve infective endocarditis
Operator-dependentTransesophageal echocardiography (TEE) Suspected infective endocarditis despite negative or inconclusive TTE
Suspected infective endocarditis in patients with prosthetic valvesHigher sensitivity than TTE for native-valve infective endocarditis, especially mitral valve infection
Higher sensitivity than TTE in the presence of prosthetic valves or cardiac implanted electronic device (CIED)
No radiation involvedPatients must fast before test
Cannot be used if oropharyngeal or esophageal structural abnormalities are present
Sensitivity still decreased if prosthetic valve or CIED is present
Anesthesia-associated risk
Operator-dependent4-dimensional computed tomography (4D CT), with or without coronary angiography Suspected infective endocarditisin patients with negative orinconclusive TTE andcontraindications to TEE
Perioperative assessment ofcoronary vasculature and aortictree in patients with knowninfective endocarditisCan detect local extension ofinfection, including abscess,fistula, and pseudoaneurysm
Can incidentally detectpulmonary emboli
Alternative to coronarycatheterization for preoperativeevaluationCan miss small valvular vegetations and perforations
Iodinated contrast may exclude patients with renal dysfunction or iodine sensitivity
Radiation exposure
Arrhythmia reduces sensitivity due to motion artifactFluorodeoxyglucose positron emission tomography (FDG-PET) Suspected infective endocarditisin patients with prosthetic valveor cardiac implanted electronicdevices and negative orinconclusive echocardiography
Patients with persistentbacteremia and negative CTto identify nidus ofinfection for source controlIdentifies metastatic sites
of infection
Increases sensitivity of Duke criteria, especially in patients with cardiac implanted electronic devices
Can identify source of bacteremia
Better than echocardiography at diagnosing intracardiac abscesses and pseudoaneurysmsFalse positives, particularly = 3months after cardiac surgery orwith vasculitis, tumors, foreignbodies, postsurgical inflammation
False-negatives with antibioticsfor several days
Limited diagnostic precision innative valve infective endocarditis
Limited ability to evaluate infectionin brain, gingiva, kidneys
Dietary carbohydrate restriction12–24 hours before study
Expensive, limited availabilityLeukocyte scintigraphy Same as for FDG-PET More specific than FDG-PET Long study duration
Expensive, limited availability
Radiation exposureCerebral magneticresonance imaging(MRI) Assess for mycotic aneurysm in patients otherwise deemed candidates for surgical intervention
Assess for cerebral hemorrhage, which may affect management (surgery, anticoagulation)More sensitive than CT for detecting intracranial lesions
Can lead to reclassification of patients (by adding a minor criterion), especially in those without neurologic symptomsDifficult in unstable patients
Contraindicated in patients with noncompatible metal hardware
Cannot be done with gadolinium enhancement in patients with contraindications (acute renal failure, chronic kidney disease with glomerular filtration rate < 30 mL/min/1.73 m2, dialysis)Cardiac MRI Quantify valvular regurgitation in patient with poor echocardiography images
Assess intracardiac spread of disease in patient unable to receive contrast and with poor echocardiography imagesMay be more sensitive than echocardiography for detecting vegetations Unclear if better than CT
Contraindicated in patients with noncompatible metallic hardware




{kind=link}
{kind=link}
{kind=link}
{kind=link}