


A 45-year-old man presented with 2 weeks of dysuria and urinary frequency. He said he had to urinate 30 to 40 times a day, but only a small volume each time. He also said he drank ten 750-mL bottles of wine daily. He had no history of nephrolithiasis, genitourinary infection, or pelvic surgery.
He had no abdominal or costovertebral angle tenderness. The bladder was not palpable, and there were no palpable masses. The prostate was not enlarged on digital rectal examination.
The serum creatinine was 4.3 mg/dL (reference range 0.58–0.96), up from 3.1 mg/dL several weeks earlier. Urinalysis showed a pH of 5.5 (4.5–8.0), 1+ protein (0), 8 red blood cells (0–5 per high-power field), and 42 white blood cells (0–3 per high-power field), with no granular casts. Urine culture was negative. The initial fractional excretion of sodium was 3.9%.
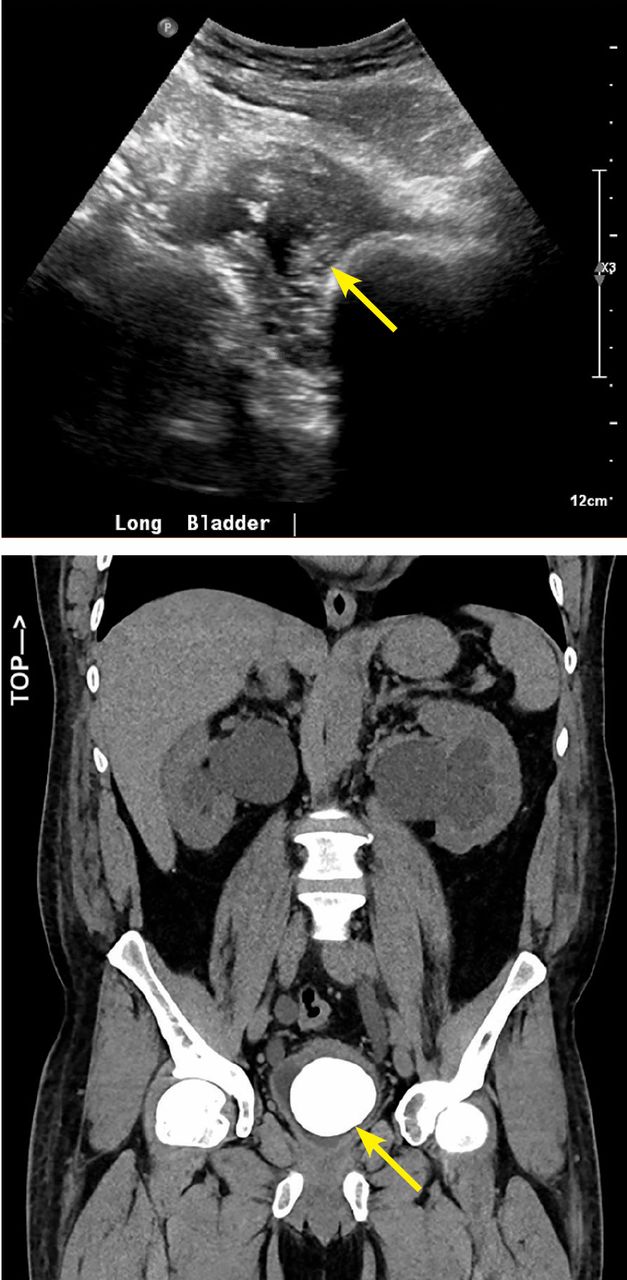
Attempts at urinary catheterization for strict output measurement were abandoned as the procedure caused the patient intense pain, especially during balloon inflation. Bladder scans showed a residual volume of 10 mL. The serum creatinine level peaked at 6.3 mg/dL on hospital day 3. Renal ultrasonography revealed severe bilateral hydronephrosis and a decompressed bladder, and computed tomography showed a radiopaque bladder stone occupying the entirety of the bladder (Figure 1).
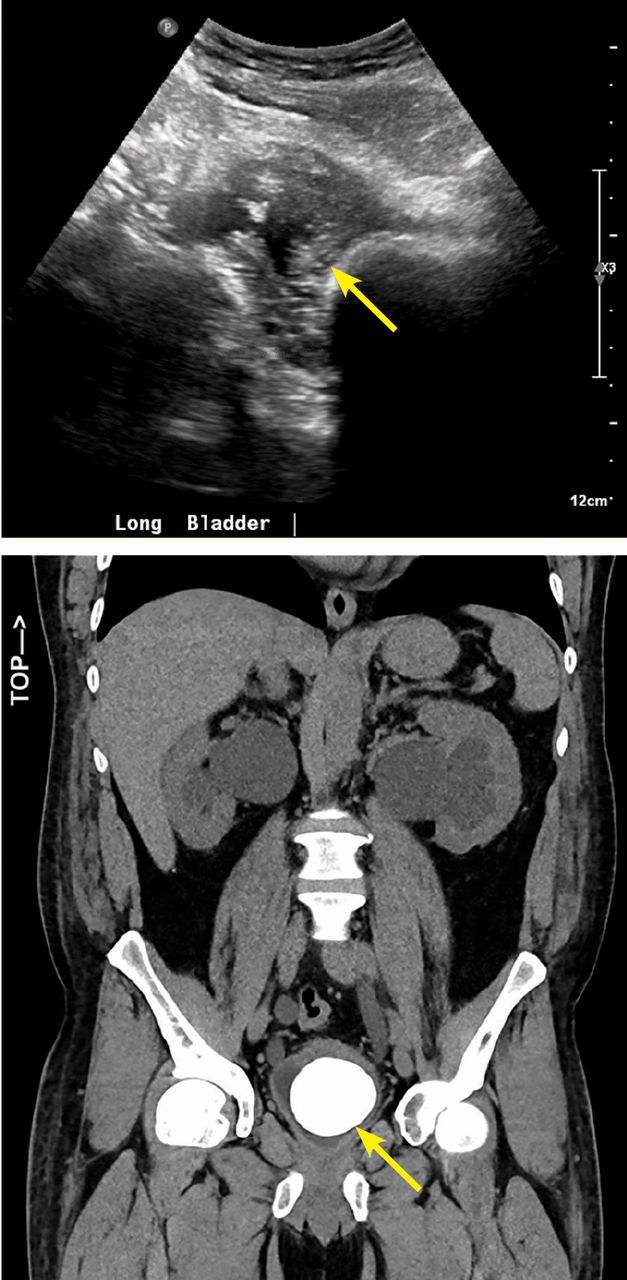
Renal ultrasonography (top) revealed a decompressed bladder (arrow). Computed tomography (bottom) showed a bladder stone occupying the entire bladder (arrow).
He underwent bilateral percutaneous nephrostomy tube placement followed by open cystolithotomy, and a large calculus (6.9 × 4.8 × 4.5 cm) was removed (Figure 2). Analysis of the stone revealed 100% uric acid composition and no evidence of a foreign body nidus. A 24-hour urine collection showed normal excretion of uric acid, calcium, citrate, phosphorus, and potassium. The acute kidney injury resolved, and his serum creatinine level came down to 1.9 mg/dL.

The bladder stone measured 6.9 cm × 4.8 cm × 4.5 cm.
GIANT BLADDER STONES
Giant bladder stones are rare and a rare cause of acute kidney injury.1 They are usually solitary and associated with urinary stasis in the setting of neurologic injury, neobladder reconstruction, or benign prostatic hypertrophy. They can also occur in chronic infections with urease-splitting bacteria or secondary to an iatrogenic foreign body.1,2
While this patient did not have any of these risk factors, computed tomography noted a small bladder diverticulum, a possible nidus of urinary stasis and calculus formation.1
There are case reports of retained surgical material and foreign bodies as a nidus for giant bladder calculi development.1 However, in our patient, no foreign body was identified during stone bisection.
Uric acid bladder stones have been associated with acidic urinary pH.3 Our patient’s initial urine pH was 5.5, which we attributed to chronic ketosis from alcoholism. It increased to 7.0 during his hospitalization with alcohol cessation, but it was again found to be 5.5 on urinalysis at follow-up visits after hospital discharge.
Bladder calculi account for only 5% of all urinary stones; they often arise in the setting of bladder outlet obstruction and are rarely associated with upper tract calculi.1,4 The earliest giant bladder stone was found in the skeleton of a 7,000 year-old Egyptian mummy, and the prevalence of these stones has dramatically decreased in the developed world due to modernization of diets.1 No specific nutritional deficiency has been causally linked to bladder stone formation, though these calculi remain most common in North Africa, the Middle East, and India in chronically undernourished children with diets low in animal protein and phosphate.1,5
Most giant bladder stones are composed of calcium phosphate or struvite, rarely uric acid. Studies suggest that only 7% of bladder calculi in men are composed of uric acid, with far more composed of calcium oxalate or struvite.6
Acknowledgment
The authors thank Dr. Juan Paredes Magaña for his care of this patient.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.