


Computed tomography (CT) is one of the most frequently utilized imaging modalities in medicine due to its ability to evaluate for a wide range of pathologies. The use of contrast agents, intravenous (IV) or oral, improves image quality by further delineating anatomical structures. However, contrast enhancement is not always necessary and does come with some risks. The appropriateness of contrast enhancement usually depends on the suspected diagnosis. In cases in which the diagnosis is uncertain, administration of contrast is reasonable, although the benefits should be weighed against any potential risks.
INTRAVENOUS CONTRAST
All modern IV contrast agents are iodine-based. The iodine causes increased absorption and scattering of the incoming radiation, which serves to increase the attenuation or “brightness” of the tissue or organ.1 Importantly, the IV contrast used in CT is distinct from the gadolinium-based IV contrast used in magnetic resonance imaging, meaning that there is no cross-reactivity between the two, which is important if the patient is allergic to one of them.
IV contrast is necessary for the evaluation of any kind of vascular disease, since it allows for easy identification of the blood vessel lumen.1 In abdominal imaging, IV contrast is recommended in most cases.
ORAL CONTRAST
The primary benefit of oral contrast is its ability to distend the bowels to help distinguish them from adjacent abdominal structures.
Oral contrast comes in two forms: neutral or positive. Neutral oral contrast consists of water or a dilute, low-attenuation solution that mirrors water. Positive oral contrast is an iodinated (ie, gastrografin) or barium-based solution with high attenuation that further demarcates bowel by opacification.
The advent of multidetector CT, which offers improved resolution, has made it easier to differentiate abdominal structures without the need for the opacification with positive oral contrast. As a result, some have argued that neutral oral contrast may be preferable to positive oral contrast due to similar efficacy, cost-effectiveness, and easier patient tolerability.2
GENERAL INDICATIONS FOR CONTRAST USE IN ABDOMINOPELVIC CT
The decision to use contrast in abdominopelvic CT depends on the diagnosis suspected.
IV contrast is recommended in most cases (Table 1).3 It is useful in the evaluation of infection (appendicitis, colitis, diverticulitis, pyelonephritis) (Figure 1); inflammation (pancreatitis, inflammatory bowel disease), masses and malignancies; and vascular abnormalities (gastrointestinal bleeding, aortic dissection, abdominal aortic aneurysm). However, IV contrast is not necessary to diagnose bowel perforations, nephrolithiasis, or hematomas.
Indications for intravenous contrast in abdominal and pelvic computed tomography

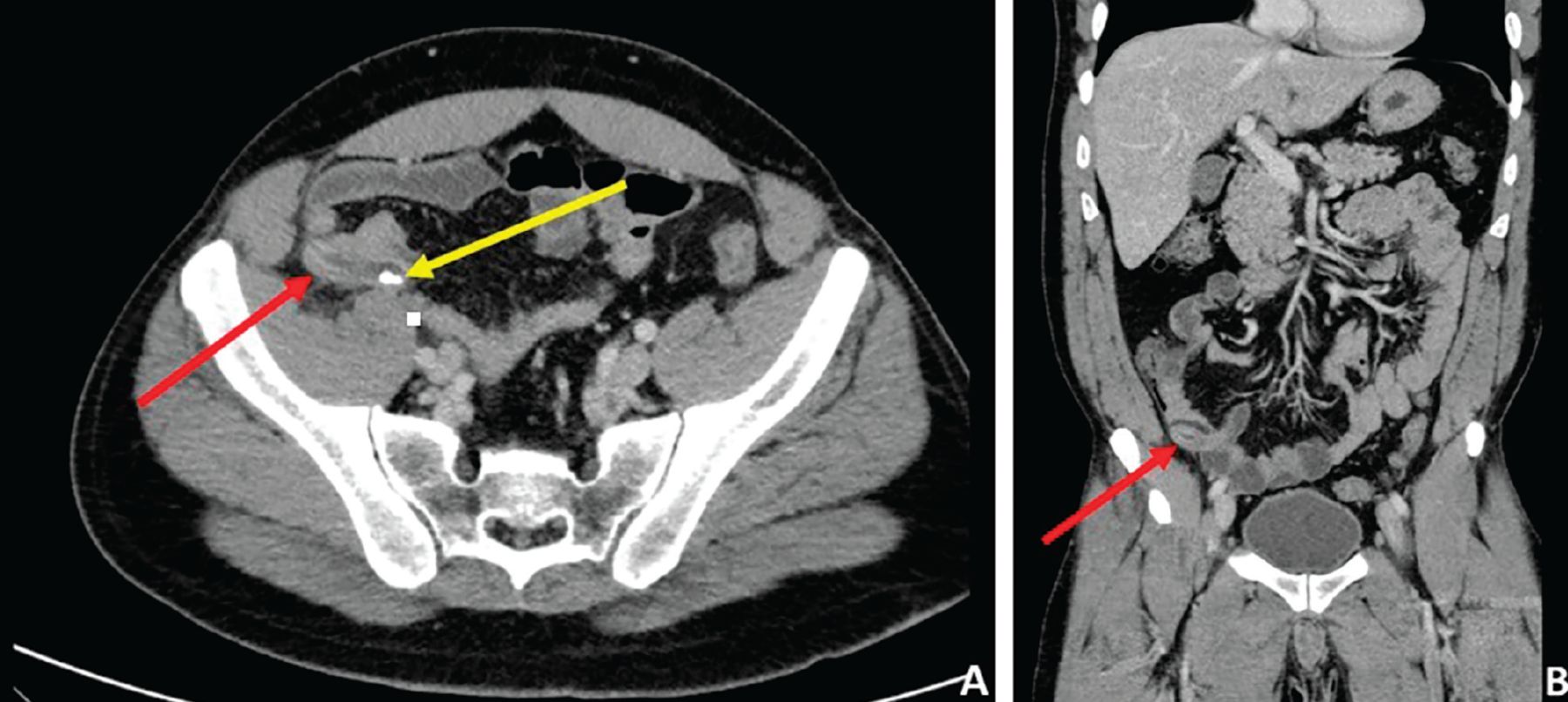
Computed tomography with intravenous contrast enhancement in a patient with right-lower-quadrant abdominal pain. Axial (A) and coronal (B) views reveal diffuse mural and periappendiceal edema, with thickening of the appendix (red arrows). Coarse calcification within the appendix (yellow arrow) likely represents an appendicolith.
In vascular imaging, the study of choice is CT angiography, which is timed so that the image is taken when the IV contrast reaches the arterial system, making it easier to identify active bleeding.
The use of oral contrast is more controversial.4–6 No clear consensus exists on the need for oral contrast, and expert opinion often drives current practices with regard to oral contrast use at academic medical centers.6 In general, when the primary reason for CT is to evaluate the liver, gallbladder, pancreas, spleen, adrenal glands, or urinary tract, oral contrast is unnecessary.
Alternatively, when evaluating the gastrointestinal lumen or bowel wall, oral contrast may be beneficial (Figure 2). However, oral contrast is not needed in the diagnosis of appendicitis or diverticulitis, even though both are luminal disorders.5
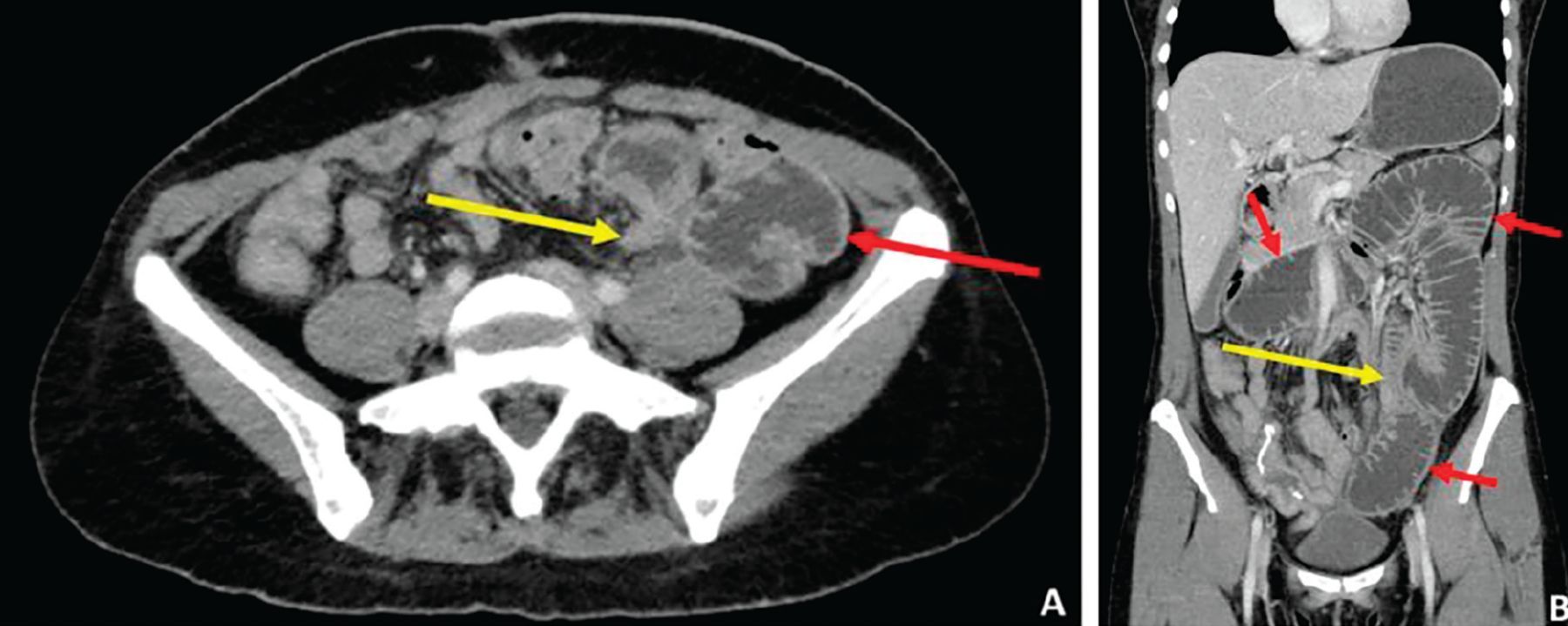
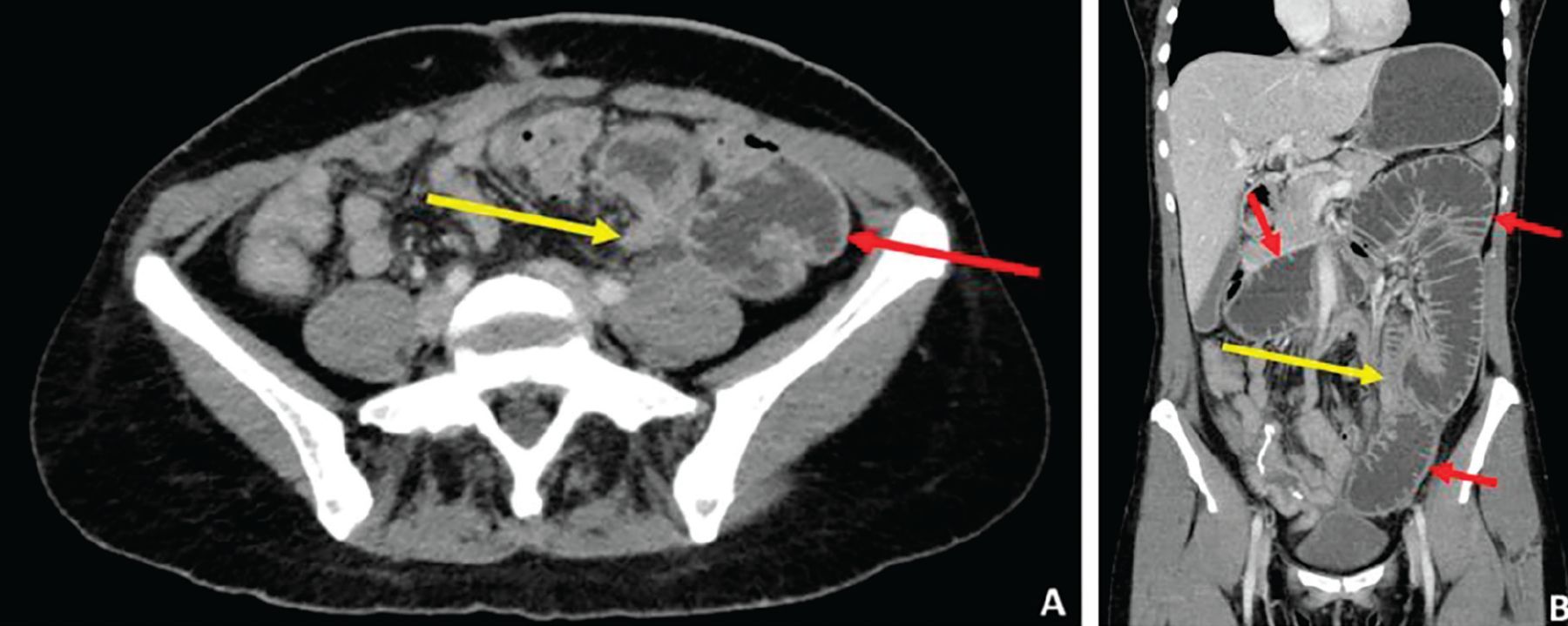
Computed tomography with a neutral oral contrast agent. Axial (A) and coronal (B) views reveal multiple loops of dilated bowel (red arrows) with a transition point—ie, site of sudden luminal narrowing (yellow arrows)—in the left lower quadrant, findings consistent with a small-bowel obstruction.
Bowel “illumination” achieved with positive oral contrast is useful when searching for “breaks” in the bowel wall, such as what would be seen with fistulas and perforations, or for identifying fluid collections or abscesses between loops of opacified bowel.
Conversely, neutral oral contrast is preferred when evaluating for mural abnormalities or a suspected gastrointestinal bleed, as positive contrast will opacify and mask the luminal surface, making it challenging to identify the bleeding source.4
In patients presenting with nonspecific abdominal complaints, some would argue that the addition of the use of oral contrast optimizes the diagnostic yield of abdominal CT.6 Woolen et al found that 89% of patients would prefer oral contrast if it had any diagnostic benefit.7 Thus, in patients undergoing abdominal CT for vague or nonspecific complaints, the addition of oral contrast to the study appears reasonable.
ADVERSE EFFECTS OF CONTRAST
IV contrast carries a risk of an allergic reaction (incidence 0.6%), which can manifest as urticaria, pruritus, bronchospasm with wheezing, or anaphylactic shock.8 Several premedication regimens consisting of a steroid with or without an antihistamine are available for at-risk patients (Table 2).8
Premedication regimens for patients allergic to intravenous contrast
Risk of nephropathy
Another concern with IV contrast is its use in patients with underlying renal disease. These patients are at risk for developing contrast-induced nephropathy (CIN), which is an acute kidney injury (AKI) that develops within 48 hours of IV contrast administration. The diagnosis is fairly controversial, with some studies having found similar rates of AKI in patients undergoing CT with and without IV contrast.9 IV contrast is considered unlikely to cause nephropathy in patients with normal renal function, but can cause CIN in those with impaired renal function.8
Current guidelines for IV contrast administration are based on the estimated glomerular filtration rate (eGFR).8,9 In general, patients with an eGFR of at least 30 mg/dL can receive IV contrast, whereas those with an eGFR less than 30 mg/dL (corresponding to stage 4 chronic kidney disease) are at high risk for renal failure. In these patients, a discussion should be held regarding the high probability of progression to end-stage renal disease, requiring dialysis.
Preventive measures to minimize the risk of contrast-induced nephropathy involve giving IV fluids at 100 mL/hour for 6 hours before and after contrast administration.8,9 Historically, sodium bicarbonate and N-acetylcysteine have been used as adjunctive agents, although there is a lack of evidence supporting their use.8,9
Risks of oral contrast agents
Oral contrast is generally safe and well tolerated, although some patients can experience bothersome symptoms. Neutral contrast agents may contain osmotically active substances that can promote loose stools or diarrhea. Of the positive oral contrast agents, iodinated agents should be avoided in patients at risk for aspiration, as they can cause aspiration pneumonitis. Barium-based oral contrast agents should be avoided in patients with suspected perforations (can cause mediastinitis or peritonitis) or bowel obstruction, as retained barium can harden to form a “barolith,” worsening the obstruction and requiring endoscopic or even surgical removal.10
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.