


Article Figures & Data
Figures
- Figure 1
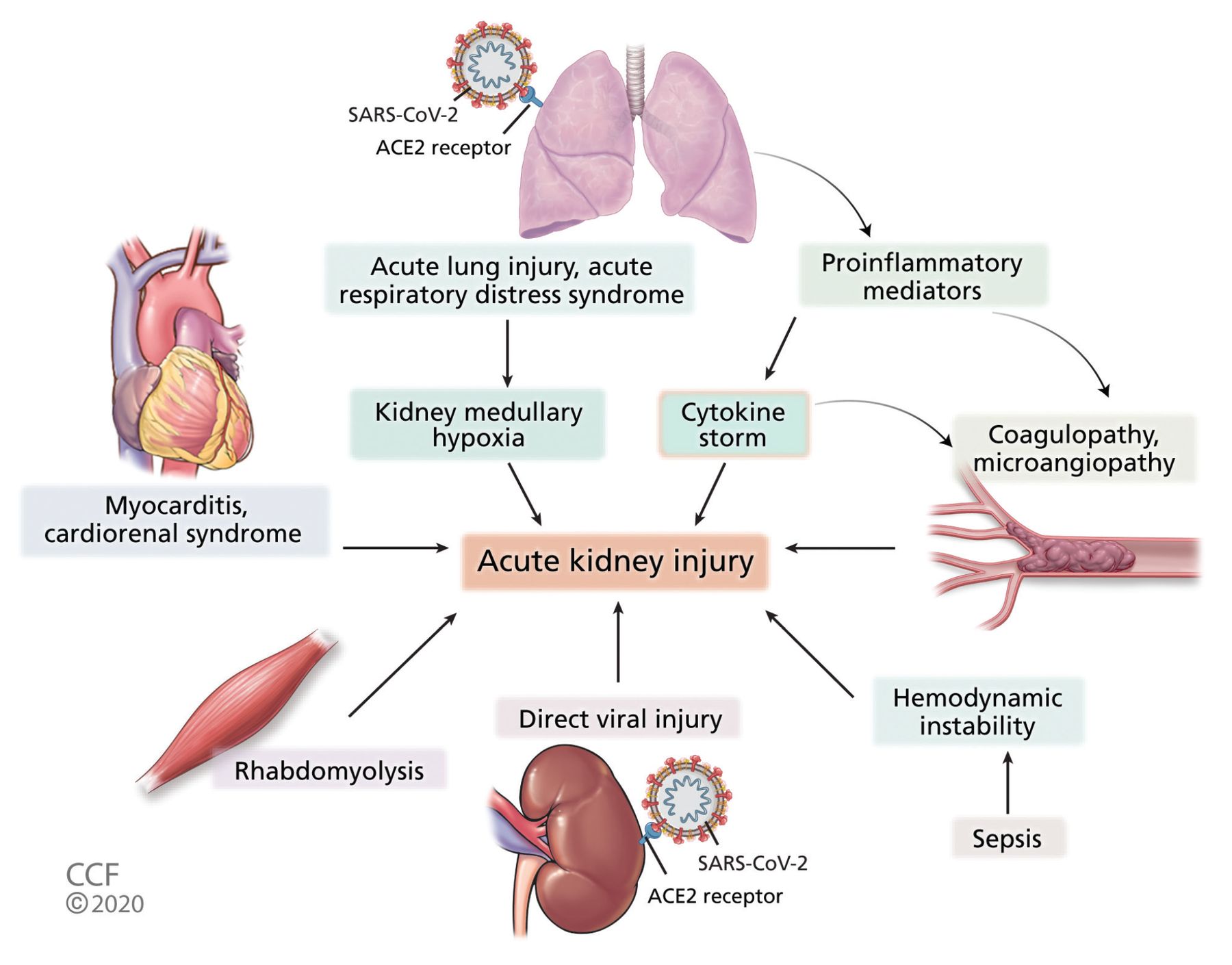
Pathophysiology of acute kidney injury in COVID-19 (ACE2 = angiotensin-converting enzyme 2; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2).
- Figure 2
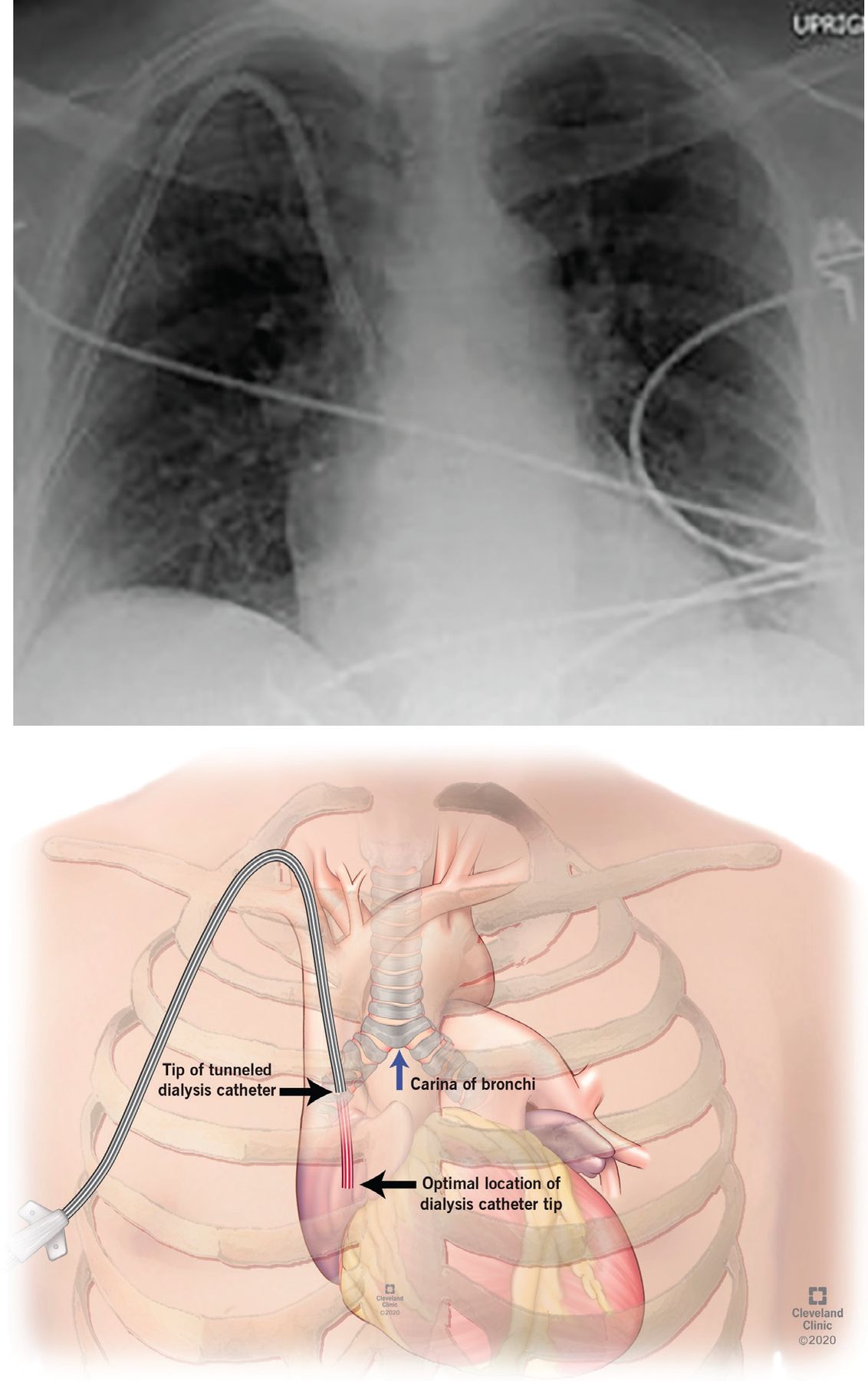
(Top) Radiography shows a short dialysis catheter with its tip in the superior vena cava in a patient with COVID -19 with frequent clotting. (Bottom) Illustration of the optimal location of the dialysis catheter in the mid-atrium.

Tables
- TABLE 1
COVID-19: Incidence of acute kidney injury and need for kidney replacement therapy
Author No. of patients Incidence of acute kidney injurya Use of kidney replacement therapy Huang et al5 41 7% 7% Chen et al16 99 3% 9% Wang et al6 138 3.6% 1.4% Yang et al14 52 29% 17% Guan et al4 1,099 0.5% 0.8% Zhou et al15 191 15% 5% Cheng et al13 701 5.1% Not reported Arentz et al22 21 19.1% Not reported Richardson et al18 2,351 22.2% 3.2% Pei et al21 333 6.6% Not reported Hirsch et al17 5,449 36.6% 5.2% Cummings et al20 257 Not reported 31% Fisher et al19 3,345 56.9% 4.9% ↵a As defined by the Kidney Disease Improving Global Outcomes criteria, ie, increase in serum creatinine by ≥ 0.3 mg/dL within 48 hours or increase in serum creatinine to ≥ 1.5 times baseline within the previous 7 days.
Cause Supporting evidence Prerenal (volume depletion) Increased blood urea nitrogen: creatinine ratio (> 20), urine sodium < 20 mmol/L, fractional excretion of sodium < 1%
Urine sediment may show hyaline castsAcute tubular injury Urine sodium > 20 mmol/L, fractional excretion of sodium > 1%
Urine sediment with granular or muddy brown castsAcute interstitial nephritis Rash, eosinophilia, white blood cells on urine microscopy
Urine sediment with white blood cell casts (urine eosinophils are not sensitive or specific)Postrenal (obstruction) Bladder scan with high postvoid residual volume, oliguria improving with Foley catheter placement
Kidney ultrasonography showing hydronephrosisRhabdomyolysis Increased serum creatine kinase and myoglobin in urine
Positive urine dipstick for blood, no red blood cells on microscopyAbdominal compartment syndrome Increased intra-abdominal pressure (> 20 mm Hg) Coagulopathy Elevated prothrombin time, partial thromboplastin time, D-dimer, fibrinogen Cardiorenal syndrome Jugular venous distention, low ejection fraction on echocardiography, urine sodium < 20 mmol/L Drug Mechanism of action Evidence, comments Possible nephrotoxicity Antiviral therapy Chloroquine, hydroxychloroquine Prevent glycosylation of host receptors and inhibit viral entry into host cells
Immunomodulatory effect through inhibiting cytokine productionInitially thought to improve viral clearance and disease duration60,61 but evidence is increasingly unsupportive
The emergency use authorization of hydroxychloroquine for severe COVID-19 was revoked in June 2020, as potential risks outweighed the benefits62Podocytopathy of the kidney mimicking Fabry disease (rare)57 Lopinavirritonavir Inhibits 3-chymotripsin-like protease Antiretroviral combination drug approved for treatment of human immunodefi ciency virus infection
No difference in viral clearance, mortality63
No benefit for patients with severe COVID-19 compared with standard care63Reversible acute kidney injury57 Ribavirin and favipravir Inhibit RNA polymerase and inhibit viral replication Favipravir is currently being evaluated in clinical trials in the United States
No prospective data to support use of ribavirinRemdesivir Inhibits RNA polymerase and inhibits viral replication Possible improvement in oxygen support status in severe COVID-19 with remdesivir58
Use of remdesivir in COVID-19 patients was associated with shortened time to recovery, but overall 14-day mortality rate was not significantly different compared with placebo66
Emergency use authorization issued for use in severe COVID-19 and recently expanded use to include all hospitalized patients with COVID-19 regardless of severity.56,57Potential mitochondrial toxicity with remdesivir57 Immunomodulatory and anti-inflammatory therapy Corticosteroids Decrease Inflammation and decrease lung injury Unpublished analysis from the United Kingdom showed a reduction in 28-day mortality rate in patients with severe COVID-19 on mechanical ventilation with the use of dexamethasone65 Tocilizumab, sarilumab Monoclonal antibodies against interleukin 6 receptor; decrease cytokine storm Repeated doses of tocilizumab may be required to decrease interleukin 6 levels7,59
Tocilizumab is recommended by the Infectious Diseases Society of America only in the context of a clinical trial72Convalescent plasma, intravenous immunoglobulin Viral antibodies from previously infected and recovered patients Clinical improvement in 5 critically ill patients with COVID-1968
High-dose intravenous immunoglobulin reportedly effective in case series with severe COVID-1969
Convalescent plasma has been granted emergency use authorization for hospitalized patients with COVID-19.58Proximal tubular injury with intravenous immunoglobulin69 ↵a This information is current at the time of this publication but may change as new findings are published.




{kind=link}
{kind=link}