


A 74-year-old woman presented with a 6-month history of malaise, generalized fatigue, significant unintentional weight loss, and night sweats, as well as pain, weakness, and stiffness in the shoulder girdle most severe in the morning. She reported no headache, visual disturbances, or jaw claudication.
On examination, blood pressure in both arms was within normal limits, and cardiovascular examination including peripheral pulses was normal without bruits.
Laboratory testing results showed erythrocyte sedimentation rate 142 mm/hour (reference range for age < 30), C-reactive protein 15.80 mg/dL (0–1), hemoglobin 9.9 g/dL (12.0–15.5), and creatine kinase 55 U/L (22– 198); other results were unremarkable.
Initially, malignancy was high on the differential diagnosis, in view of the patient’s advanced age, weight loss, and elevated levels of inflammatory biomarkers. However, computed tomography of the chest, abdomen, and pelvis were unremarkable, and upper endoscopy and colonoscopy showed no abnormalities. Thus, an autoimmune cause was considered.
The patient underwent whole-body fluorine-18 fluorodeoxyglucose positron emission tomography and computed tomography (PET-CT), which showed diffuse hypermetabolism of the great vessel walls, including the aorta and major branches, axillary arteries, common carotid artery, and common iliac artery, consistent with large-vessel giant cell arteritis (GCA) (Figure 1).
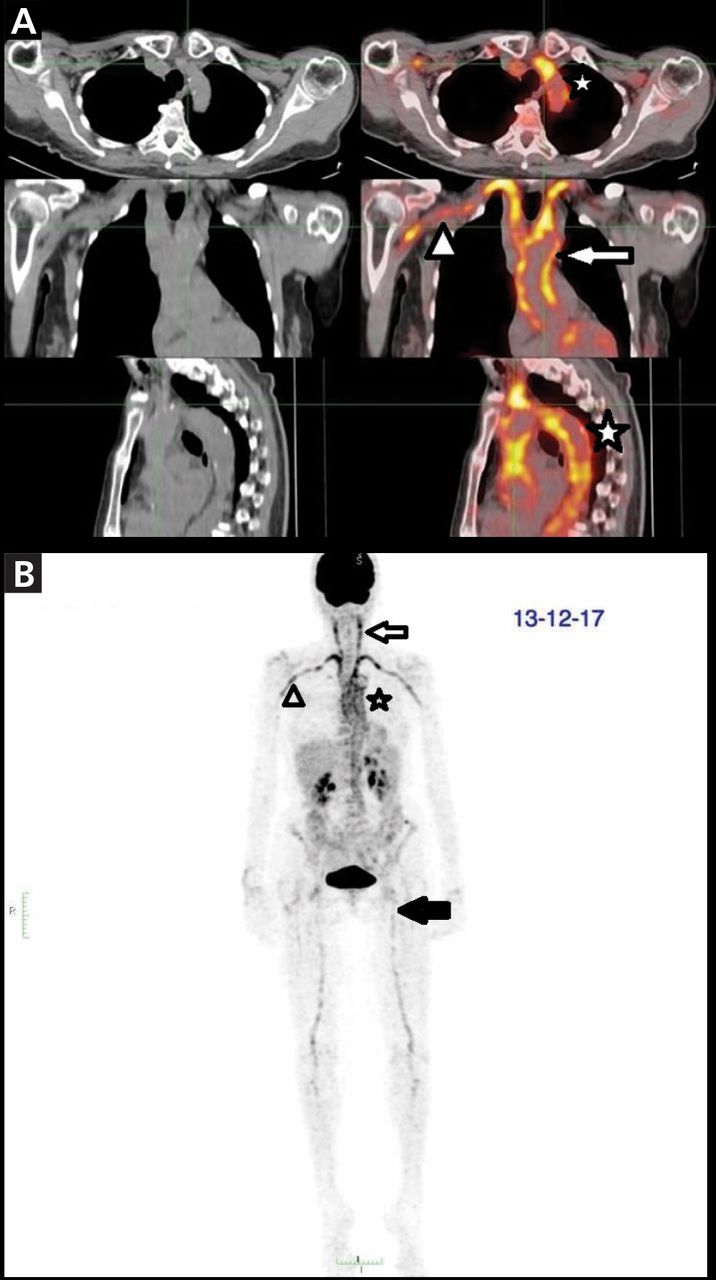
(A) Axial, coronal, sagittal, and (B) frontal positron emission tomography showed highly increased uptake of 18F-fluoro deoxyglucose in the aorta and major branches (star), axillary arteries (arrowheads), carotid arteries (arrows), and femoral arteries (black arrow).
Prednisone 50 mg/day (1 mg/kg/day) was started. This dosing was maintained for 4 weeks, after which it was gradually reduced 10% every 2 weeks. At this time, tocilizumab was not approved by the Argentine regulatory agency for the treatment of GCA, so methotrexate 15 mg weekly was added as a corticosteroid-sparing agent.
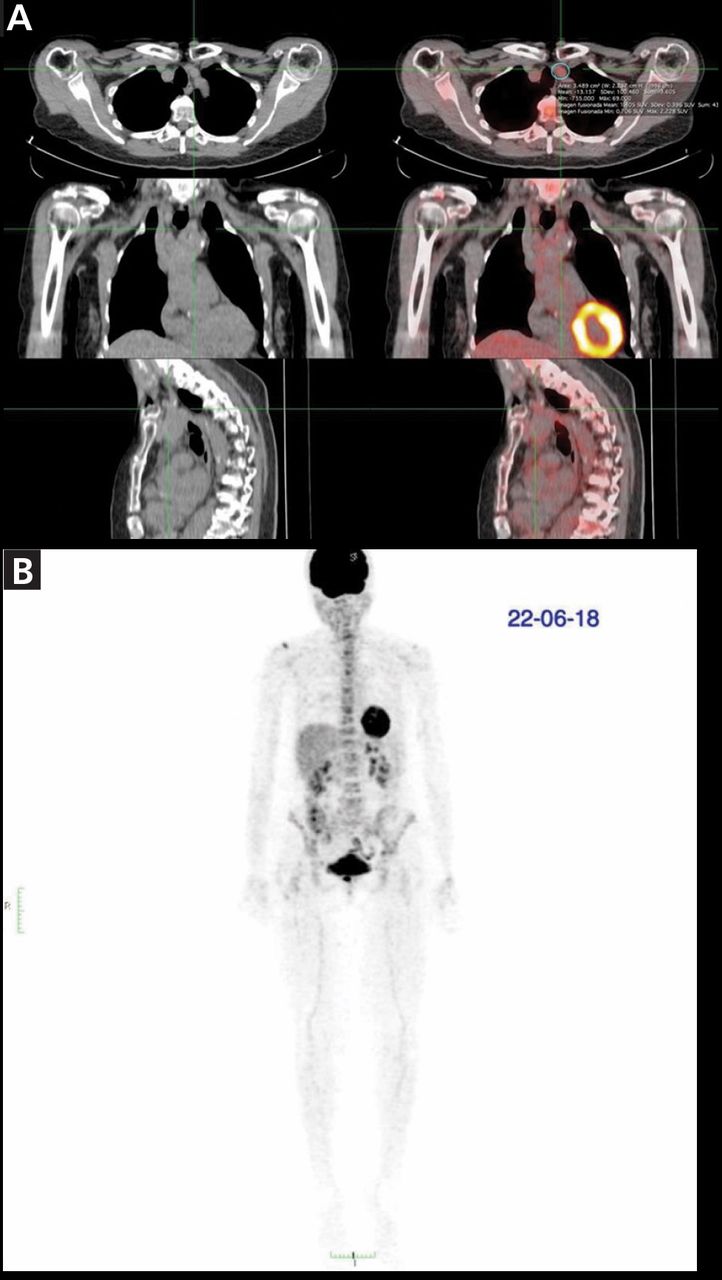
After 6 months of treatment, the patient was free of symptoms and her levels of inflammatory biomarkers had returned to normal; her erythrocyte sedimentation rate was 11 mm/hour and C-reactive protein 0.48 mg/dL. Repeat PET-CT showed significant improvement in vascular hypermetabolism, principally in the aorta and supra-aortic vessels, without metabolic activity in the subclavian arteries or extravascular metabolic hyperactivity (Figure 2).

After 6 months of treatment, (A) axial, coronal, sagittal and (B) frontal positron emission tomography showed improvement of uptake in all arterial territories.
LARGE-VESSEL GIANT CELL ARTERITIS
GCA is a granulomatous vasculitis that compromises medium and large arteries. The spectrum encompasses overlapping phenotypes including classic cranial arteritis and large-vessel (extracranial) GCA.1
Like cranial GCA, large-vessel GCA may present with constitutional symptoms such as fever of unknown origin, anorexia, weight loss, symptoms of polymyalgia rheumatica, or elevated inflammatory markers.2
In large-vessel GCA, especially if cranial symptoms are lacking, cross-sectional imaging such as magnetic resonance angiography, CT angiography, or PET-CT may be useful, because biopsy of the extracranial arteries is not feasible. In the Tocilizumab in Giant Cell Arteritis trial (GiACTA), the largest prospective study evaluating treatment in patients with GCA, 119 (86%) of a total of 138 patients who underwent cross-sectional imaging had findings consistent with large-vessel involvement.3
According to the European League Against Rheumatism recommendations for imaging in large-vessel vasculitis, the major advantage of PET in patients with suspected large-vessel vasculitis is the ability to identify GCA along with other serious pathology such as infection or tumor.4 This may be particularly relevant in elderly patients with constitutional symptoms without specific clinical features of GCA or polymyalgia rheumatica.
High cost, limited availability, and radiation exposure limit the use of PET. But combining PET with CT permits the evaluation of wall thickness and luminal changes.4
High doses of glucocorticoids (40–60 mg/day prednisone-equivalent) with gradual tapering are the mainstay of treatment. In patients with refractory disease or at increased risk of glucocorticoid-related adverse effects, methotrexate may be an alternative, glucocorticoid-sparing agent.5
In GiACTA, sustained remission rates at week 52 were 53% with tocilizumab treatment vs 17% with glucocorticoid monotherapy, while the cumulative glucocorticoid dose was reduced by 50% in tocilizumab-treated patients with fewer adverse events than those on glucocorticoids alone.6 These strikingly positive results led to tocilizumab’s approval by the US Food and Drug Administration.
Encouraging results have also been reported with ustekinumab, an interleukin 12 and interleukin 23 antagonist, and with abatacept, a selective T cell costimulation modulator.2 A new era in the treatment of an old disease is coming.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.