


A 63-year-old woman presented to the outpatient metabolic bone disease clinic with a 6-month history of lumbar and dorsal back pain. Initially, facet arthrosis was suspected and physical therapy suggested.
See related editorial, page 339
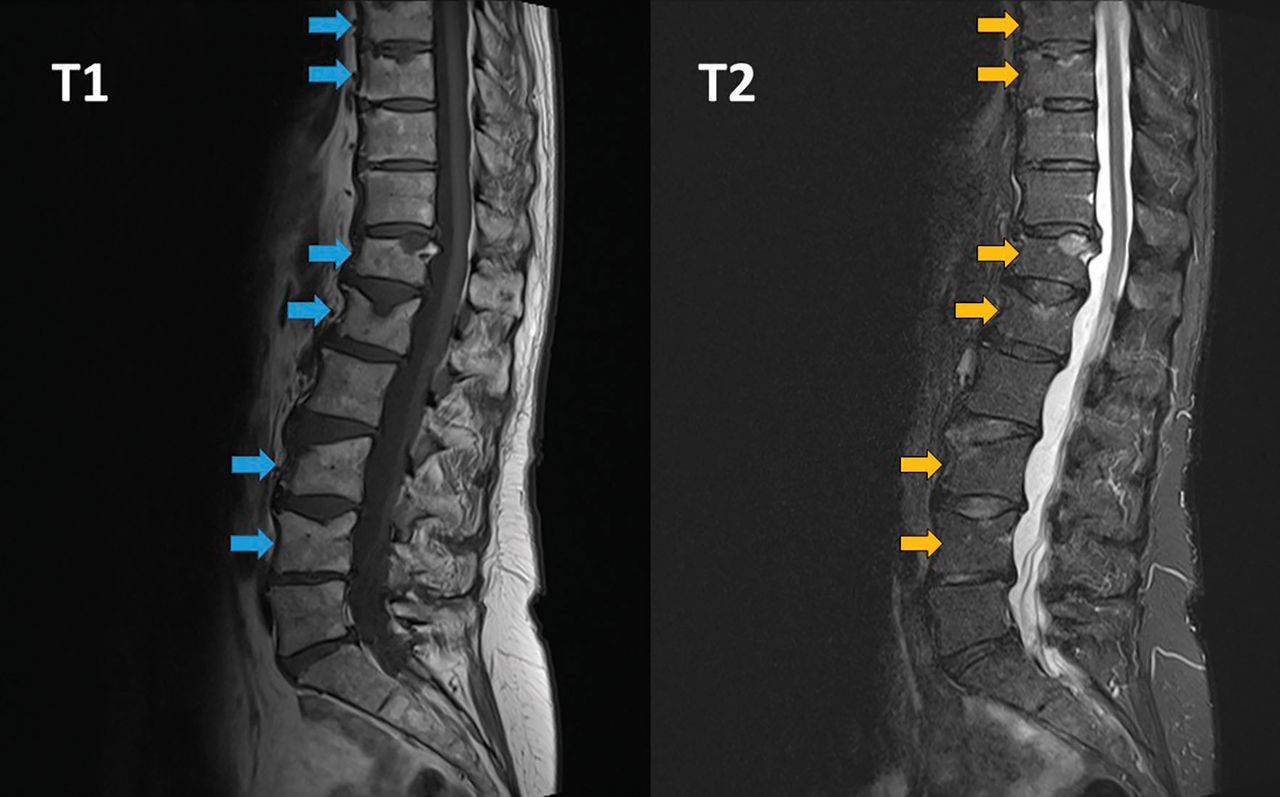
Physical therapy for 1 month brought no improvement in her pain. Lumbar radiography was performed, which showed a vertebral fracture at T12. Magnetic resonance imaging (MRI) of the thoracic and lumbar spine (Figure 1) revealed vertebral fractures at T6, T7, T8, T9, T12, L1, L3, and L4. T2-weighted MRI revealed bone marrow edema, which suggested that all fractures were recent.
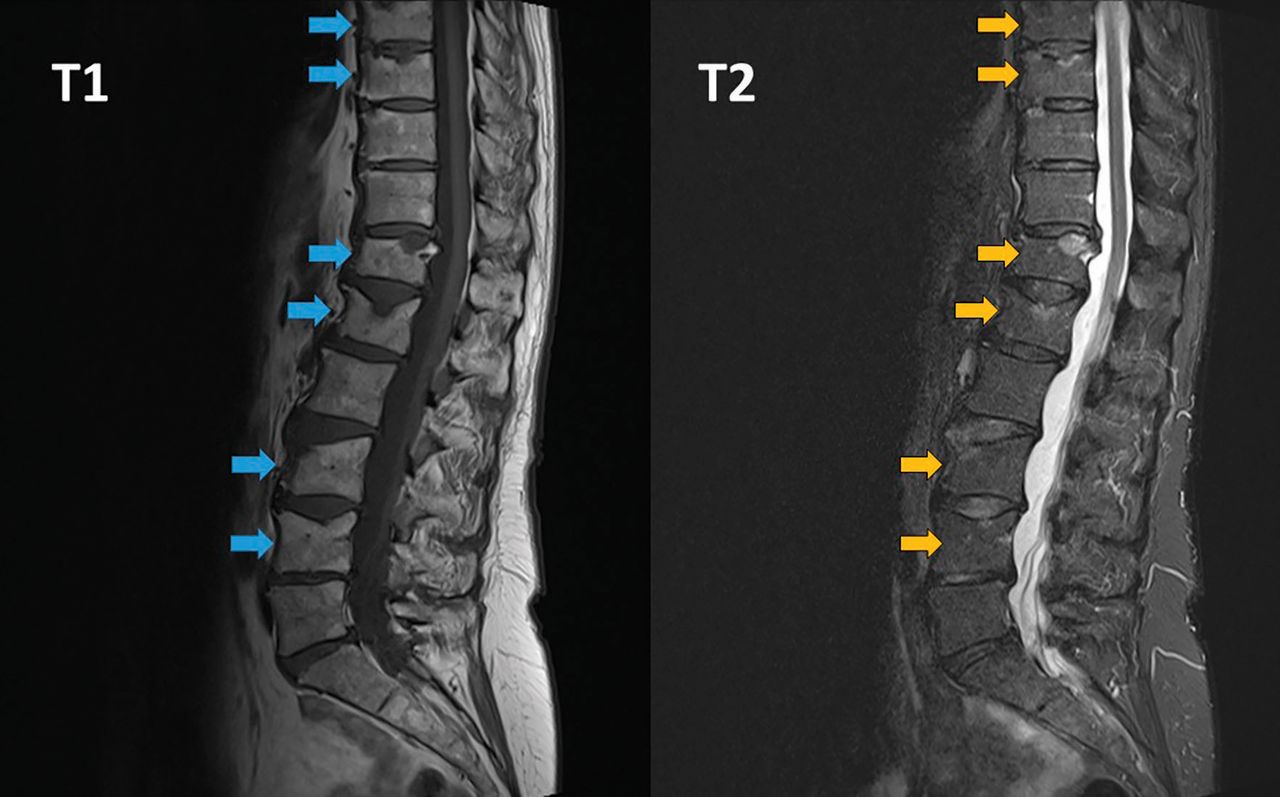
T1-weighted magnetic resonance imaging (left) indicated vertebral fractures of T8, T9, T12, L1, L3, and L4 (arrows). T2-weighting (right) showed bone marrow edema (arrows).
The patient had a history of postmenopausal osteoporosis without prior fractures, treated with subcutaneous denosumab injections every 6 months for 5 years. Ten months before the onset of her first symptoms and 16 months before diagnosis of vertebral fractures, denosumab was stopped for a “drug holiday” after 5 years.
There was no imaging available from before the start of denosumab, although computed tomography done for kidney stones 9 months after denosumab cessation showed no lumbar vertebral fractures (thoracic spine not visible on these images). Moreover, her beta-C-terminal telopeptide concentration—a marker of bone turnover—was 852 ng/L (reference range 104–1,008 ng/L) at the time of MRI and diagnosis of vertebral fractures. These findings suggested recent rebound-associated vertebral fractures after denosumab cessation.
REBOUND-ASSOCIATED VERTEBRAL FRACTURE
Denosumab is a commonly used antiresorptive that increases bone mineral density and reduces the risk of vertebral, nonvertebral, and hip fractures in postmenopausal osteoporosis. It has a reversible effect, and after denosumab cessation, bone turnover markers transiently rebound above baseline levels.1
A 2018 post hoc analysis of data from the Fracture Reduction Evaluation of Denosumab in Osteoporosis Every 6 Months (FREEDOM) trial on study participants who discontinued denosumab suggested that the rate of vertebral fracture increased after denosumab cessation to a level comparable with that in untreated patients,2 a phenomenon often described as rebound-associated vertebral fracture.3–10 In patients who subsequently developed fractures, there was a significant increase in the number of those sustaining multiple vertebral fractures, with previous vertebral fracture being the main risk factor.2
Most rebound-associated vertebral fractures occur 2 to 10 months after the effect of the last dose is depleted,2,3 as in our patient’s case.
There is no optimal management protocol for denosumab cessation based on evidence from randomized controlled trials. Based on current knowledge, it is recommended not to stop denosumab without considering alternative treatments (eg, a potent bisphosphonate) in order to prevent rapid loss of bone mineral density and a potential rebound in vertebral fracture risk.2,11,12 Our patient was treated with zoledronate intravenously immediately after diagnosis of the fractures. At most recent follow-up, she has suffered no additional fractures.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}