


ABSTRACT
In a perimenopausal or postmenopausal woman, an elevation in human chorionic gonadotropin (hCG) can raise the concern of malignancy or even pregnancy, but it can also be a benign physiologic finding due to production in the pituitary gland in this patient population. Diagnosing the underlying cause of hCG elevation can be challenging, especially if a pituitary source is not considered. Pituitary hCG production remains largely underrecognized and can lead to unnecessary testing, harmful therapy such as chemotherapy, or delay in receiving appropriate care for other unrelated diseases. It is therefore important to establish guidelines to aid medical evaluation.
We do not recommend further evaluation in perimenopausal or postmenopausal women when hCG levels are less than 14 IU/L and follicle-stimulating hormone (FSH) levels are 40 IU/L or higher.
In patients with hCG levels of 14 IU/L or higher and FSH levels lower than 40 IU/L, we recommend following the USA hCG Reference Service protocol, which starts with confirming the high hCG level using multiple other assays.
The human chorionic gonadotropin (hcg) level is routinely measured to diagnose and monitor pregnancy. In addition, because hCG can be elevated in females with trophoblastic disease, germ cell tumors, and other malignancies, it is often used as a prognostic marker and for disease monitoring.1 These days, more women, even those in perimenopause and menopause, are having their hCG levels measured to rule out pregnancy before they undergo imaging studies or treatments that could harm a fetus.
However, elevated hCG levels have been detected in as many as 0.2% to 10.6% of perimenopausal and postmenopausal women who are not pregnant and have no disease or tumor.2–4 This phenomenon remains underrecognized, and appropriate patient care may be delayed while the source of the elevation is being sought.
In this paper, we review the evidence regarding how to assess perimenopausal and postmenopausal hCG elevation.
STRUCTURE AND BIOLOGY OF hCG
The heterodimeric glycoprotein hCG is composed of an alpha subunit and a beta subunit. Its alpha subunit is identical to the alpha subunits of luteinizing hormone (LH), follicle-stimulating hormone (FSH), and thyroid-stimulating hormone. The beta subunit, on the other hand, differs among these hormones and determines the hormone’s specificity and function.1
Fifteen variants of hCG have been detected,5 some of which are biologically active, while others are breakdown products and are inactive. The most common variants are listed in Table 1.6
Common detectable variants of human chorionic gonadotropin (hCG)
The variant can suggest the source of the hCG elevation. In normal pregnancy, intact hCG is the predominant form, whereas in trophoblastic disease or testicular tumors, the free beta subunit or hyperglycosylated hCG predominates.7,8 More than 100 immunoassay test kits are available to measure hCG.9 All kits measure intact hCG along with one additional variant, and it is important to be aware of which hCG variant is being measured in the immunoassay used, especially when evaluating for trophoblastic disease.
Measurement of hCG is usually done using a 2-site noncompetitive immunoassay in which the analyte (hCG) is sandwiched between two antibodies. Certain factors can interfere with the assay and lead to erroneous results. False-positive results can occur from cross-reactivity with other serum glycoproteins or from heterophilic antibodies that can bind to the antibodies used in the hCG assay.10,11 False-negative results can occur in cases in which the true hCG level is so high that the assay antibodies become supersaturated. This is known as the “hook effect” and can be avoided through serial dilutions.
ELEVATED hCG IN PERIMENOPAUSAL AND POSTMENOPAUSAL WOMEN
The exact role of hCG outside of pregnancy remains unclear. In premenopausal women, hCG and LH levels rise during ovulation.2 As women get older, hCG levels, like those of FSH and LH, rise due to loss of negative feedback inhibition from estrogen and progesterone.2–4,12–16 Levels of hCG and FSH reach a peak between the ages of 45 and 55 and remain at a plateau thereafter.14 In pregnant women, hCG levels have a diurnal variation, rising in the day and decreasing at night.17
Confusion can arise when hCG values are higher than the normal laboratory cutoff of 5 IU/L in nonpregnant perimenopausal and postmenopausal women. The prevalence of hCG levels of 5 IU/L or higher in women between the ages of 41 and 55 is 0.2% to 0.3%, while in older women it is 8% to 10.6%.14,15 When hCG is “elevated,” physicians often pursue an evaluation for gynecologic disease, malignancy, or paraneoplastic syndrome. Often overlooked, however, is the possibility that the hCG is coming from the pituitary gland.
THE ROLE OF PITUITARY PRODUCTION OF hCG
Pituitary hCG production was first described in the 1970s after hCG staining was seen in pituitary gland extracts.16,18,19 The pituitary gland was also confirmed as a source of hCG production by Stenman et al,16 whose work in 1987 showed that hCG levels rose 2- to 3-fold in healthy nonpregnant women and men who were given gonadotropin-releasing hormone (GnRH), and fell in postmenopausal women who were given combined estrogen and progesterone. (In this study, estradiol valerate 2 mg with medroxyprogesterone acetate 10 mg daily).16
Several studies have since investigated this physiologic phenomenon in an attempt to establish hCG cutoff values to help differentiate between a normal physiologic rise in hCG and a rise related to an underlying pathologic disease.2–4,17,19–21 In postmenopausal women, an hCG value of 14 IU/L has been established as the normal upper limit, while in perimenopausal women no clear cutoff value has yet been defined. This is important, as most laboratories give only the reference range for premenopausal nonpregnant women and not the reference range for postmenopausal women.
The FSH level can help distinguish the source of the excess hCG in perimenopausal women, ie, the pituitary vs the placenta (in pregnancy). FSH levels higher than 45 IU/L were found to have a 100% negative predictive value for a pituitary origin of elevated hCG.14 FSH levels were not found to correlate with hCG levels in postmenopausal women.15
Physiologic hCG elevations in perimenopausal and postmenopausal women are still largely unrecognized, and the confusion can delay medical therapy and even lead to unnecessary treatment. Cole et al3 described 28 cases of elevated hCG levels in which unnecessary chemotherapy was given, inappropriate surgery was done, or therapy for other medical conditions was delayed pending workup. The mean hCG level was 9.5 IU/L (range 2.1–32 IU/L), and the median was 7.7 IU/L. In 18 of these cases, a pituitary source was confirmed by hCG suppression after 2 weeks of hormone therapy.
In another study,2 18 of 36 perimenopausal and postmenopausal women with elevated hCG either received inappropriate medical therapy or experienced delay in surgery. The average hCG level in the perimenopausal women was 6.4 IU/L, and in the postmenopausal women it was 11.6 IU/L. In this series, 24 patients were given high-estrogen birth control pills, which suppressed hCG production in 23, confirming a pituitary origin. In contrast, hCG levels originating from germ cell tumors are generally significantly higher, as shown in a study by Arrieta et al in which the mean hCG level was 14,772 IU/L.22
A PROTOCOL FOR EVALUATING ELEVATED hCG IN POSTMENOPAUSAL WOMEN
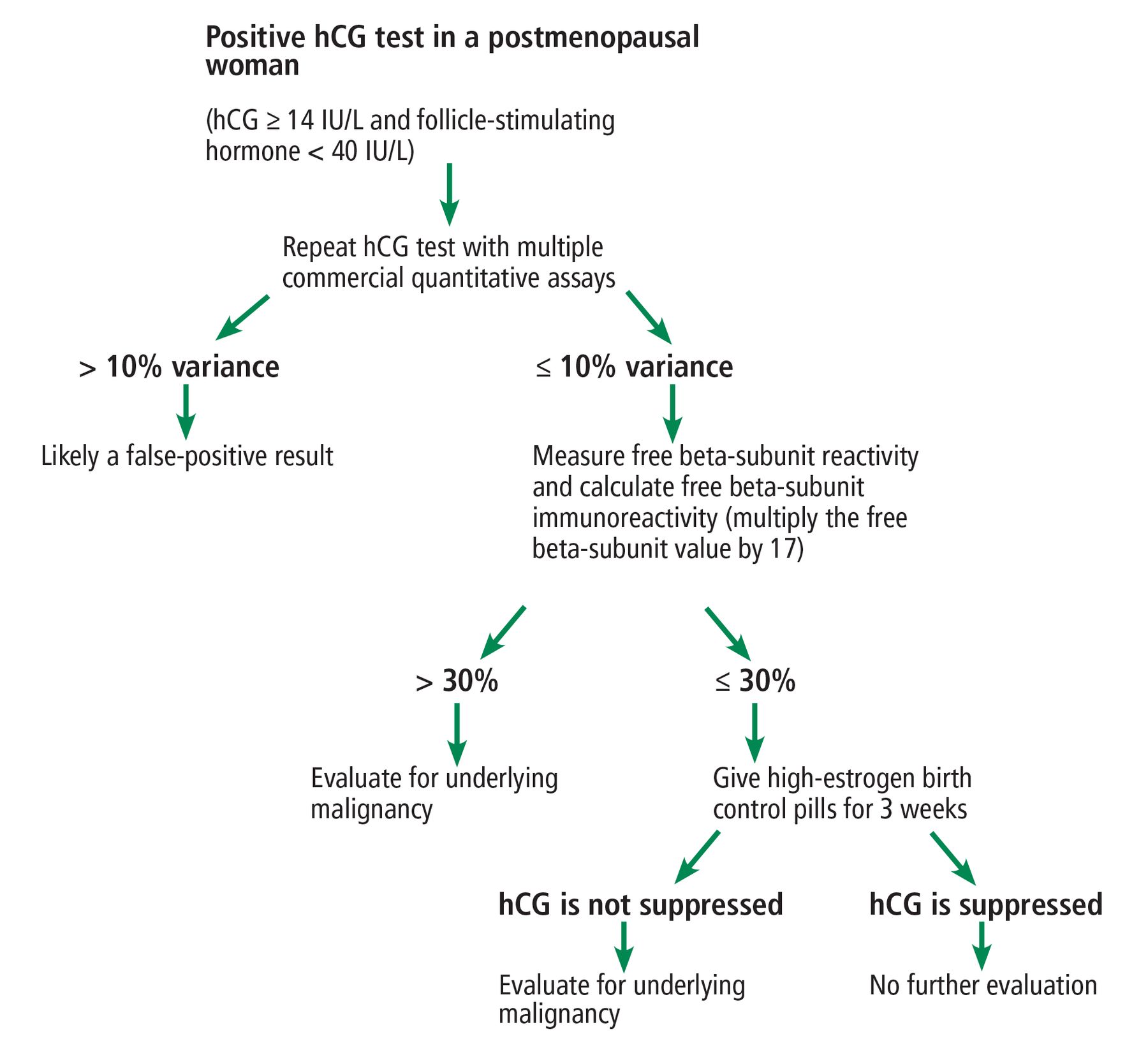
The USA hCG Reference Service provides a consulting service, maintains a database of cases of elevated hCG, and has presented a protocol for evaluating hCG elevations measured using commercial assays in postmenopausal women (Figure 1).2,23
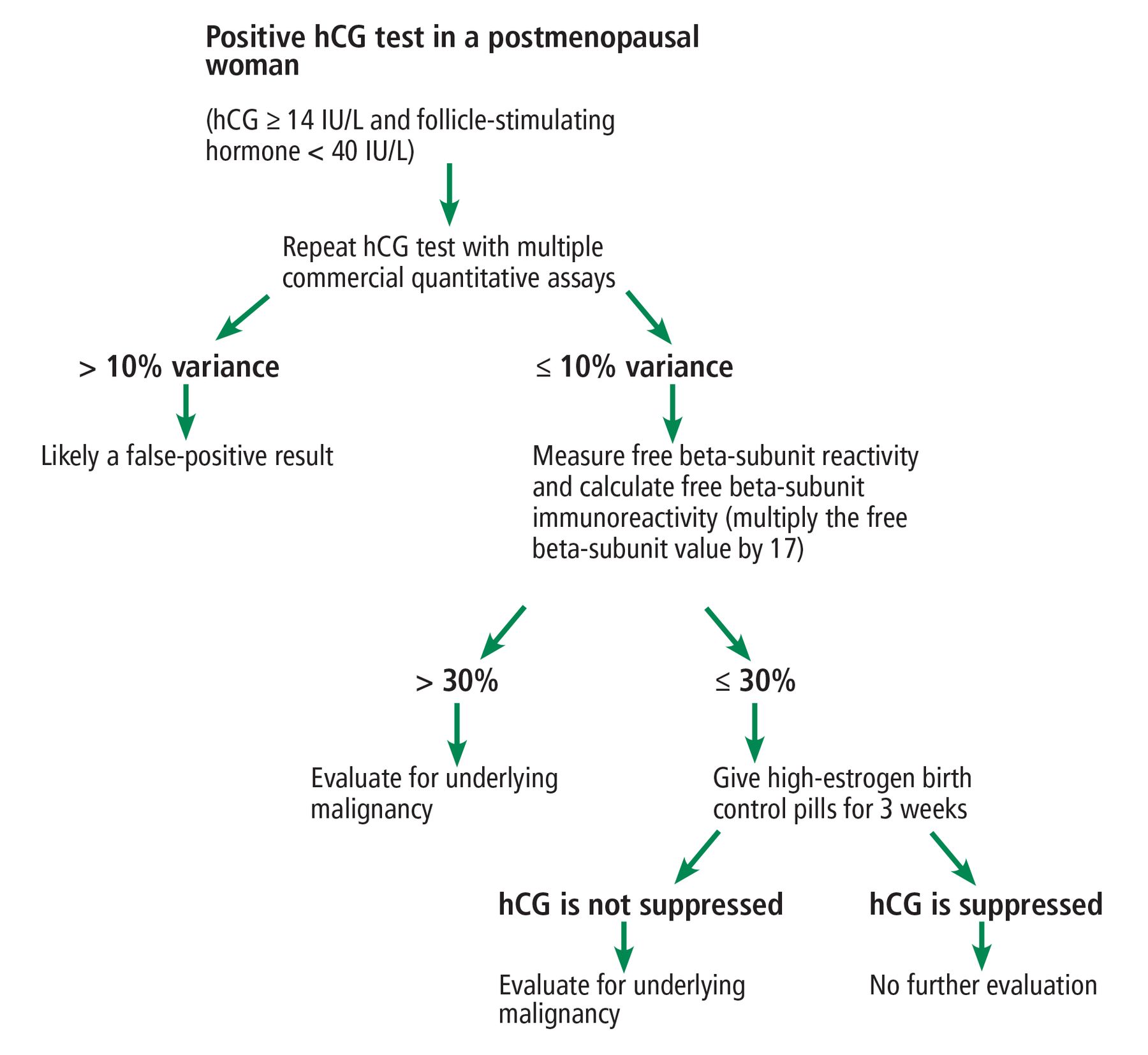
Recommended protocol for evaluating elevated human chorionic gonadotropin (hCG) in postmenopausal women.
The first step is to confirm hCG elevations and to exclude false-positive readings due to interfering heterophilic antibodies by repeating the measurement using different commercial assays. If the results differ by less than 10%, then interference can be excluded.
The next step is to exclude nontrophoblastic malignancy by measuring the free beta subunit and calculating the free beta subunit immunoreactivity (by multiplying the free beta subunit value by 17). If the calculated free beta subunit immunoreactivity is 30% or less, then malignancy is unlikely.
The last step is to confirm the pituitary gland as the source of hCG by demonstrating hCG suppression after 3 weeks of hormone therapy. High-estrogen birth control pills containing 50 μg of ethinyl estradiol plus progesterone are recommend. Hormone therapy can be discontinued after 3 weeks unless medically indicated for other reasons.
Women who cannot undergo hormone suppression can instead be tested using a GnRH analogue such as leuprolide 3.75 intramuscularly. Despite an initial surge of hCG after GnRH stimulation, the level becomes suppressed within 1 week through desensitization of the pituitary to a continuous GnRH output, as opposed to the pulsatile GnRH secretion seen in the physiologic state. Levels of hCG of pituitary origin will be suppressed several days after GnRH analogues are given, whereas hCG secreted from a tumor will not. A pituitary source is confirmed if hCG is suppressed to normal levels 10 days after injection.20,21
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2021 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}