


A 73-year-old man presented with lymphocytosis and retroperitoneal lymphadenopathy and was found to have chronic lymphocytic leukemia (CLL), Rai stage II (possible stages are 0–IV). He was not initially treated for it but was monitored until 5 months later, when he was admitted to the hospital with multilobar pneumonia with acute hypoxic respiratory failure and a white blood cell count of 139 × 109/L (reference range 4.5–10.9 × 109/L). He was treated with a combination of broad-spectrum antibiotics, vasopressor support, and high-dose corticosteroids.
FIRST EPISODE OF ANEMIA
His hospital course was complicated by complement-fixing nonimmunoglobulin G autoimmune hemolytic anemia, as well as tumor lysis syndrome. During this episode, he had the following laboratory values:
Hemoglobin 5.5 g/dL (14–18 g/dL)
Mean corpuscular volume 106 fL (80–100 fL)
Lactate dehydrogenase 903 mg/dL (135–225 mg/dL)
Reticulocyte count 96 × 109/L, 4.4% (90–130 × 109/L, 1%–2%)
Haptoglobin undetectable.
Most likely, a factor contributing to tumor lysis syndrome was the use of corticosteroids to treat his respiratory failure, which led to destruction of lymphocytes and spilling of intracellular components. This was manifested by hyperphosphatemia, hyperuricemia, and acute kidney injury, consistent with tumor lysis syndrome.
To control his autoimmune hemolytic anemia, the patient was given a combination of prednisone 1 mg/kg tapered over 6 weeks and intravenous immune globulin 500 mg/kg daily for 5 days, followed by rituximab 375 mg/m2 once a week for 4 doses, and his anemia resolved.
SECOND EPISODE OF ANEMIA
Four months later his anemia recurred, with a hemoglobin level of 6.5 g/dL.
1. What would be your next step in managing this patient’s anemia at this time?
Restart steroids; this is a recurrence of his autoimmune hemolytic anemia
Perform a workup to determine the cause of his anemia, including reticulocyte count, lactate dehydrogenase, haptoglobin, bilirubin counts, direct antiglobulin test, and peripheral smear review
Perform bone marrow aspiration and biopsy
No need for further evaluation, start treatment of CLL
Check flow cytometry
The next step should be to perform a workup to determine the cause of the anemia.
FINDING THE CAUSE OF ANEMIA
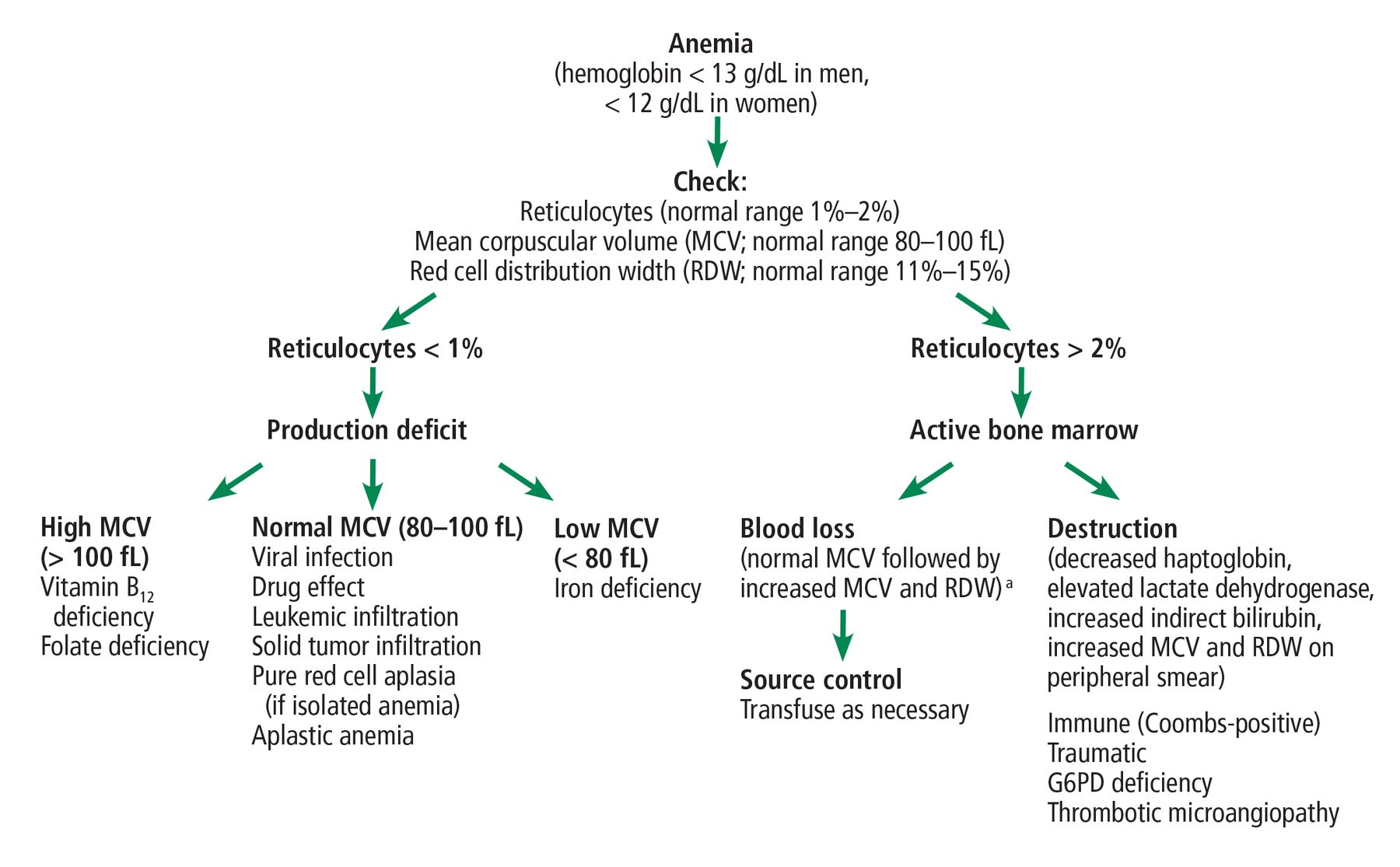
Anemia—a hemoglobin below 13 g/dL in men and below 12 g/dL in women1—can result from a deficit in red blood cell production, destruction of red blood cells, or blood loss. An evaluation of new anemia following the algorithm outlined in Figure 1 as an initial step will help define the mechanism and guide its management. The first step is to check the reticulocyte count, a marker of bone marrow production that can help differentiate the underlying mechanism of acquired anemia.
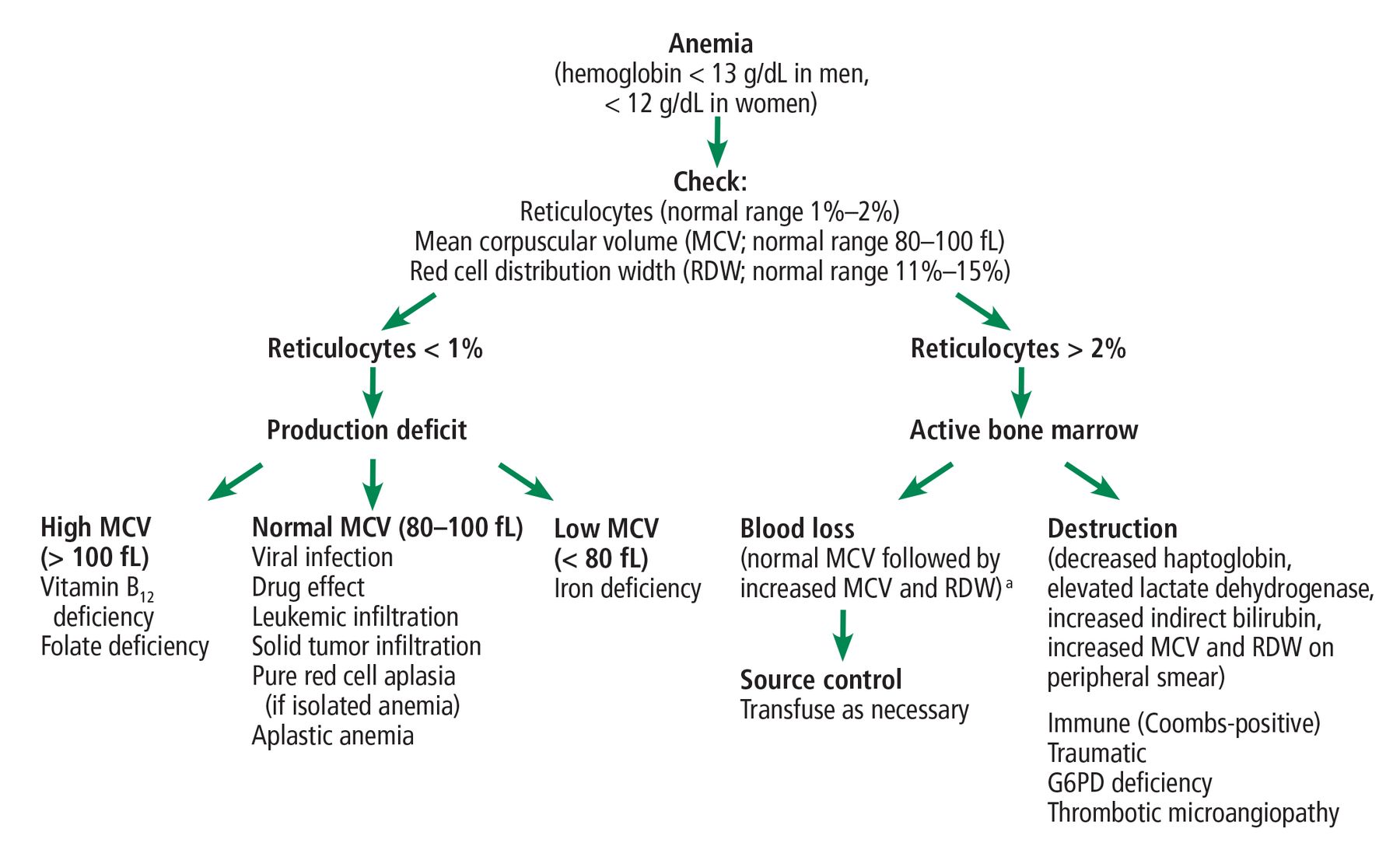
General approach to finding the mechanism of anemia.
aBlood loss initially presents with a normal MCV and RDW due to strict whole volume loss. However, with subsequent reticulocytosis, the MCV will increase, thus increasing the RDW. Chronic blood loss leads to iron deficiency, which manifests with anemia that has a low MCV and high RDW.
G6PD = glucose-6-phosphate dehydrogenase
If the reticulocyte count is high
Reticulocytes are immature red blood cells. If there are more of them than usual in the blood of a patient with anemia, it means that the bone marrow is functioning and is responding to the red blood cell destruction or blood loss by increasing the production of red blood cells.
Reticulocytes are larger than mature red blood cells, and an increased proportion of reticulocytes causes an increase in the mean corpuscular volume as well as the red cell distribution width, which represents the variability in size of the red blood cells.
An elevated reticulocyte count associated with low haptoglobin, elevated lactate dehydrogenase, and elevated indirect bilirubin is consistent with a hemolytic process.2
A positive direct antiglobulin test (also called the direct Coombs test) and spherocytes on the peripheral smear suggest auto immune hemolytic anemia. On the other hand, a negative direct antiglobulin test points to traumatic hemolysis, thrombotic microangiopathy, or oxidative hemolysis due to enzyme defects such as glucose-6-phosphate dehydrogenase (G6PD) deficiency as the cause of hemolysis. Traumatic hemolysis and thrombotic microangiopathy present with schistocytes on the peripheral smear, while G6PD deficiency manifests with bite and blister cells.
A negative hemolytic workup with an elevated reticulocyte count suggests hemorrhage. Management of a clinically overt hemorrhage is directed at controlling the source. In cases in which the source of blood loss is not obvious, imaging and endoscopy to look for internal bleeding can be helpful.
With acute blood loss, the mean corpuscular volume is initially normal until reticulocytes enter circulation. Chronic blood loss leads to iron deficiency, which is associated with a low mean corpuscular volume and elevated red blood cell distribution width, as red blood cells will have different sizes depending on the amount of iron available as they develop.
If the reticulocyte count is normal or low
If the reticulocyte count is not elevated in the setting of anemia, this suggests impaired bone marrow function. Bone marrow dysfunction can be due to a viral illness, drug effect, nutritional deficiency, infiltration of the marrow by malignant cells, infection, fibrosis, pure red cell aplasia, aplastic anemia, or myelodysplasia. The clinical history and review of medications are helpful in identifying a viral or drug effect. Diagnosis of an infiltrative process requires bone marrow aspiration and biopsy.
Vitamin B12 and folate are essential for nucleic acid synthesis. Deficiency in either of these nutrients will lead to asynchrony in nucleic acid and cytoplasmic development of red blood cells, leading to megaloblastic anemia with elevated mean corpuscular volume and a low reticulocyte count.
Moreover, because iron, folate, and vitamin B12 are required for erythropoiesis, the reticulocyte count could be falsely low in a patient with anemia that is due to red blood cell destruction or blood loss in case of a concomitant nutritional deficiency.
Causes of anemia in chronic lymphocytic leukemia
Anemia is a manifestation of many different diseases, not a disease itself. With each episode of anemia, a new evaluation is needed to determine if it is a recurrence of the previous condition—in our patient, autoimmune hemolysis. Whether or not the patient has CLL, it is important to keep in mind the common causes of anemia in elderly people, such as gastrointestinal angiodysplasia, diverticulosis, and myelodysplasia. However, certain complications and associations are more frequent in patients with CLL, and these include the following:
Enlarged spleen
Autoimmune hemolytic anemia (such as in our patient’s initial episode)
Marrow suppression due to extensive disease infiltration
Marrow suppression secondary to drug or chemotherapy
Gastrointestinal blood loss that is related to drug adverse effects (glucocorticoids or ibrutinib), thrombocytopenia, or coagulopathy
Pure red blood cell aplasia.
The prevalence of autoimmune hemolysis in CLL varies among different case series, ranging between 5% and 10%.3,4 The development of autoimmune hemolysis in CLL is more frequent in men, older patients (over age 65), and patients with a lymphocyte count greater than 60 × 109/L.4
Of note, patients with CLL can have a positive direct antiglobulin test without autoimmune hemolysis. In a retrospective series by Ricci et al,5 the prevalence of direct antiglobulin test positivity in patients with CLL was 14%, but only 8 (40%) of the 20 patients with positive tests had autoimmune hemolysis.
Autoimmune hemolysis in chronic lymphocytic leukemia is treated with steroids
Treatment of autoimmune hemolysis in a patient with CLL follows the same algorithm as for idiopathic autoimmune hemolytic anemia. Glucocorticoids are the initial treatment. However, treatment with steroids should not be started again in our patient before confirming that his second episode of anemia is also of autoimmune origin. Only in cases that are refractory to steroids is treatment of underlying CLL indicated, according to an international working group on CLL.6 Interestingly, in patients with CLL, autoimmune hemolysis does not have independent prognostic significance.4
THE PATIENT UNDERWENT BIOPSY
The patient received steroids and intravenous immunoglobulin followed by rituximab, which would affect both the B-cell clone secreting the antibodies causing the hemolytic anemia and the B-cell clone responsible for his CLL.
Laboratory testing during the second episode of anemia revealed a low reticulocyte count, normal lactate dehydrogenase and indirect bilirubin levels, and a high haptoglobin level, suggesting bone marrow suppression (Table 1). The patient did not have any clinical signs to suggest a viral infection, and he was receiving no drugs commonly associated with anemia.
The patient’s laboratory values in his second episode of anemia
Because the pattern was different than in his first episode and pointed to a problem in the bone marrow, the patient underwent bone marrow aspiration and biopsy, which revealed pure red blood cell aplasia and marrow infiltration by CLL.
Pure red cell aplasia
Pure red cell aplasia is a well-described but uncommon autoimmune complication of CLL, seen in less than 1% of patients.7 It is characterized by anemia with severe reticulocytopenia, with reticulocyte counts usually less than 10 × 109/L, and by marked reduction or absence of erythroid precursors on bone marrow aspiration and biopsy. Pure red cell aplasia affects only the erythrocyte lineage, leading to a decrease in production of otherwise-normal red blood cells. Therefore, as in our patient, the peripheral smear red blood cells would have a normal morphology.8
Viral infections and thymoma should be ruled out in all patients who develop acquired pure red cell aplasia. Thymomas are rare in the general adult population, and although previous reports suggested that up to 50% of patients with pure red cell aplasia had thymomas, the prevalence is now thought to be much lower.8
The management of acquired pure red cell aplasia depends on the cause and includes intravenous immune globulin for viral infections and surgical resection for thymomas. In pure red cell aplasia secondary to a lymphoproliferative disorder, the treatment is directed at the underlying disease, which in our patient is CLL.8
WHEN SHOULD CLL BE TREATED?
While both autoimmune hemolysis and pure red cell aplasia are associated with CLL, not all cases of anemia that arise in a patient with CLL are due to disease progression. Most patients with CLL are elderly, and therefore the causes of anemia that arise in the elderly population such as gastrointestinal angiodysplasia, diverticulosis, or myelodysplasia need to be excluded.
Many people with CLL can forgo therapy for an extended time with close observation. CLL is chronic and currently incurable, and the goal of treatment is to manage its complications. Treatment is indicated when disease is bulky, symptomatic, or rapidly evolving or causes cytopenias.6
Indications for treatment, per the CLL working group,6 include the following:
Progressive marrow failure evidenced by the development or worsening of anemia or thrombocytopenia
Splenomegaly that is massive (ie, ≥ 6 cm below the left costal margin), progressive, or symptomatic
Lymphadenopathy that is massive (ie, ≥ 10 cm in longest diameter), progressive, or symptomatic
Rapidly progressive lymphocytosis with a doubling of the lymphocyte count over less than 6 months or an increase of more than 50% over a 2-month period
Autoimmune anemia or thrombocytopenia that is refractory to corticosteroids
Constitutional “B symptoms.”
Constitutional B symptoms include the following:
Unintentional weight loss of 10% or more within the previous 6 months
Significant fatigue (ie, Eastern Cooperative Oncology Group performance status ≥ 2 on a scale of 0–5; inability to work or perform usual activities)9
Fever, with a temperature greater than 100.5°F (38.0°C) for at least 2 weeks without other evidence of infection
Night sweats for at least 1 month without evidence of infection.
Is flow cytometry needed?
There is no reason to repeat flow cytometry during an episode of anemia, as it would only reconfirm the diagnosis of CLL and would not have any effect on management.
CASE CONTINUED
As noted above, the patient’s second episode of anemia was determined to be due to pure red cell aplasia.
A trial of steroids was ineffective, and the patient was subsequently started on ibrutinib with rituximab to treat his CLL. The anemia resolved, but the patient developed severe neutropenia that resolved after withdrawing the rituximab. The patient remained well for more than 2 years while taking ibrutinib alone, with resolution of anemia and no additional complications of CLL.
A third episode of anemia
At a follow-up telehealth visit, the patient’s hemoglobin level was noted to have decreased from 11.6 g/dL to 8.9 g/dL over the course of 6 months. He said he had no signs or symptoms of bleeding and no new palpable lymph nodes. Repeat blood tests and imaging were arranged.
When the patient came in for computed tomography, he appeared pale, his heart rate was rapid, and he reported having dyspnea on exertion. Sent to the emergency department, he said he had had no recent hematochezia, melena, bleeding, or trauma, and he had no palpable lymphadenopathy or hepatosplenomegaly.
He was found to have severe anemia, with a hemoglobin level of 4.3 g/dL (Table 2). Results of his basic metabolic panel on presentation are shown in Table 3. He was given a transfusion of 3 units of packed red blood cells.
The patient’s complete blood cell count in the emergency department in his third episode of anemia
The patient’s basic metabolic panel in the emergency department in his third episode of anemia
WHAT IS THE NEXT STEP?
2. Which of the following is the appropriate next step in evaluating the patient’s anemia?
No need for further evaluation, start next-line treatment for CLL
Anemia workup including reticulocyte count, lactate dehydrogenase, haptoglobin, bilirubin, direct antiglobulin test, and peripheral smear review
Bone marrow aspiration and biopsy
Hold ibrutinib
Computed tomography of the chest, abdomen, and pelvis
Anemia workup
As previously mentioned, every episode of anemia requires a new evaluation, following the algorithm outlined in Figure 1, and therefore this is again the best next step.
Bone marrow aspiration and biopsy
Findings of a decreased reticulocyte count with normal iron, vitamin B12, and folate would indicate an impaired bone marrow necessitating biopsy and aspiration. While bone marrow biopsy carries minimal risk, it is still an invasive procedure that is uncomfortable for the patient, and therefore it would be unjustified before excluding other causes through a repeat anemia workup.
Holding the ibrutinib would also be reasonable in managing this patient’s anemia. Ibrutinib is an irreversible inhibitor of Bruton tyrosine kinase, an integral component of the B-cell receptor signaling and cytokine receptor pathways that allow malignant B cells to survive. It can contribute to anemia through 2 mechanisms, ie, by inducing cytopenia and by inhibiting platelet activation, leading to bleeding. Drug-induced anemia improves when the inciting factor is removed. Treatment of bleeding in a patient receiving ibrutinib includes discontinuing the ibrutinib and transfusing platelets. The incidence of bleeding with ibrutinib is highest in the first 2 years of treatment, then decreases with time.10
Treating the CLL
Clinical examination is helpful in evaluating anemia in CLL. Disease progression can cause splenomegaly that can lead to anemia. Bulky adenopathy can be a manifestation of progression of CLL and is an indication for treatment. However, not all adenopathy is clinically palpable.
Computed tomography
Further investigation with computed tomography is controversial but can be considered to look for lymphadenopathy in nonpalpable sites such as the mediastinum and retroperitoneum.
CASE CONTINUED: UNEXPECTED BIOPSY FINDINGS
The results of further laboratory evaluation of the patient’s third episode of anemia are included in Table 4.
Further laboratory findings in the patient’s third episode of anemia
After the patient received a transfusion of packed red blood cells his hemoglobin level increased to 7.2 g/dL. Laboratory testing revealed that he again had decreased reticulocytes and no indications of hemolysis.
The patient again underwent bone marrow aspiration and biopsy, which this time revealed focal clusters of epithelial cell proliferation, mostly in solid nests with focal glandular formation (Figure 2). In addition, there was a trace population of kappa light-chain restricted monoclonal B cells (0.08%) with a flow cytometry phenotype consistent with CLL. Staining of the epithelial clusters was positive for AE1 and AE3 (which are cytokeratins positive in carcinomas) and NKX3.1 (which is 98.6% sensitive and 99.7% specific for prostate adenocarcinoma).11,12
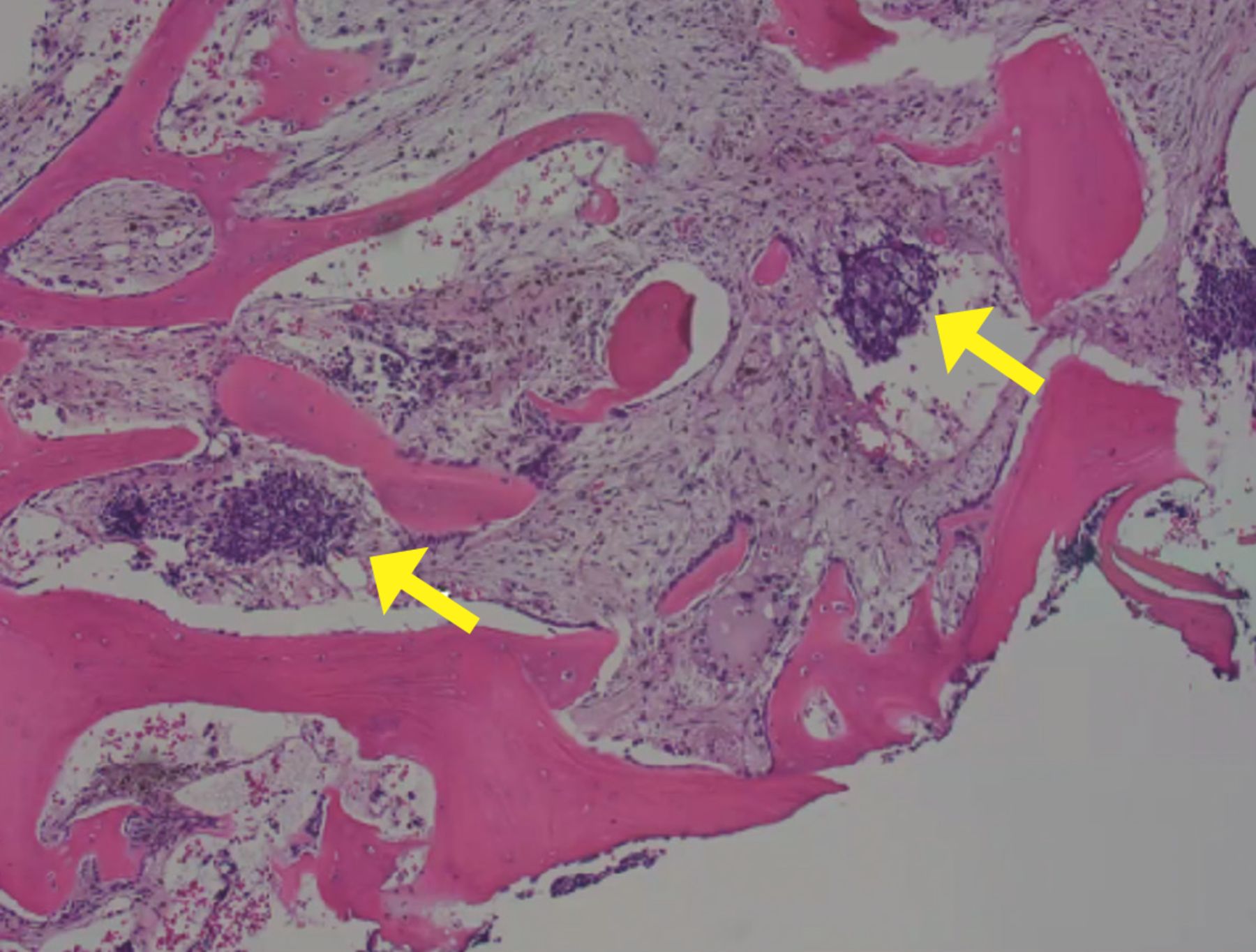
Focal bone marrow infiltration by solid nests of tumor cells (arrows) in the patient’s third episode of anemia (hematoxylin and eosin, × 20).
The biopsy results suggested that the cause of the anemia was metastatic prostate adenocarcinoma, and treating the prostate cancer would treat the anemia. In metastatic hormone-sensitive prostate adenocarcinoma, the first step in treatment includes androgen deprivation therapy through either surgical castration or medical castration with the use of gonadotropin-releasing hormone agonists and antagonists.13
EFFECT OF PROSTATE CANCER ON THE PERIPHERAL BLOOD SMEAR
Myelophthisis refers to displacement of hematopoietic cells from the bone marrow by an infiltrative process, most commonly malignancy, fibrosis, or a granulomatous process. In some cases, hematopoietic stem cells relocate to niches outside of the marrow, a phenomenon known as extramedullary hematopoiesis. Extramedullary hematopoiesis usually develops in the liver, spleen, or both.
Myelophthisis often leads to immature precursors, including nucleated red blood cells, immature granulocytes such as myelocytes or meta-myelocytes, as well as teardrop-shaped red blood cells spilling into the circulation. The constellation of these findings on the peripheral blood smear is termed leukoerythroblastosis.14,15
Myelophthisis is found in less than 10% of cases of metastatic carcinoma and is most frequent in prostate, breast, and lung cancers.16 In one review,17 among patients with carcinoma that was metastatic to the bone marrow, only 44% exhibited signs of leukoerythroblastosis. Our patient’s peripheral blood smear did not show any of the typical signs of leukoerythroblastosis, revealing only a normocytic anemia. Treatment of myelophthisis is aimed at managing the underlying infiltrative process, improving bone marrow function, and resolving cytopenias.
CASE CONCLUDED
Imaging and blood tests revealed that the patient’s previously noted mesenteric lymphadenopathy had decreased in size with no new sites of lymphadenopathy. However, he had new diffuse bony sclerotic lesions and a prostate-specific antigen level of 664 ng/mL (normal < 4 ng/mL). These findings suggested that his CLL was still under control but he also had stage IV prostate cancer with bone metastases.
The patient’s CLL continues to be managed with ibrutinib. He was started on anti-androgen therapy with leuprolide, a gonadotropin-releasing hormone agonist, as well as abiraterone acetate, an inhibitor of CYP17, an enzyme required for androgen biosynthesis. His bone metastases have responded to treatment. He feels back to normal and has regained his energy and takes care of all his activities of daily living.
TAKE-HOME POINTS
CLL is generally considered an incurable, chronic disease. The current treatment strategy is to manage the complications of the disease, which can include cytopenias. It is therefore essential to understand the multiple mechanisms of anemia in patients with CLL, how to diagnose them, and how to manage them.
Every new episode of anemia does not automatically imply disease progression, and each should be evaluated completely. The initial evaluation should include at least the reticulocyte count to assess bone marrow response, the mean corpuscular volume, the red cell distribution width, and review of the peripheral smear with further testing as needed.
This case also highlights the importance of avoiding anchoring bias, as each new episode of anemia had a different cause that called for different treatment.
DISCLOSURES
Dr. Gonsky reports ownership interest in Abbvie Pharmaceuticals, Johnson & Johnson, and Pfizer. Dr. Ghanem reports no relevant financial relationships which, in the context of his contributions, could be perceived as a potential conflict of interest.
- Copyright © 2022 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
- Article
- FIRST EPISODE OF ANEMIA
- SECOND EPISODE OF ANEMIA
- FINDING THE CAUSE OF ANEMIA
- THE PATIENT UNDERWENT BIOPSY
- WHEN SHOULD CLL BE TREATED?
- CASE CONTINUED
- WHAT IS THE NEXT STEP?
- CASE CONTINUED: UNEXPECTED BIOPSY FINDINGS
- EFFECT OF PROSTATE CANCER ON THE PERIPHERAL BLOOD SMEAR
- CASE CONCLUDED
- TAKE-HOME POINTS
- DISCLOSURES
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.