


ABSTRACT
Primary care physicians are typically the frontline clinicians who assess female patients for their risk of breast cancer, doing so by using a combination of risk algorithms and collecting personal and family medical histories. Patients found to be at increased risk of breast cancer, defined as > 20% overall lifetime risk, are candidates for enhanced screening. This review notes risk factors, determinants of risk, and a systematic approach for primary care physicians to assess and manage patients at risk of breast cancer.
A personalized risk assessment for breast cancer should be performed in all female patients, using a combination of risk calculators and collecting a complete history of breast cancer risk factors.
Known breast cancer risk factors include genetic mutations, previous exposure to thoracic radiation, older age, obesity, breast density, and a first-degree relative with a history of breast cancer.
Many breast cancer risk calculators are available, with strengths, weaknesses, and variables that impact the primary care physician’s efficiency and accuracy in determining screening and care.
Two commonly used risk calculators include the National Cancer Institute Breast Cancer Risk Assessment Tool, or Gail Model, and the International Breast Cancer Intervention study, or Tyrer-Cuzick Risk Model.
Breast cancer (BC) is the most commonly diagnosed cancer in women in the United States and the second most common cause of female cancer deaths.1 As such, many female patients present to primary care physicians for further guidance regarding their concerns and risks of developing BC. Risk assessment involves a significant amount of time to complete with many available risk calculation models, all of which have varied limitations.2–5
However, a personalized risk assessment for BC should be performed, to some degree, in all female patients using a combination of risk calculators and obtaining a complete medical history of BC risk factors. Approaching patients systematically; gathering basic information such as age, body mass index (BMI), family BC history, reproductive risk factors; and gathering specific risk factors such as known genetic mutations, prior chest radiation, or history of atypical hyperplasia or lobular carcinoma in situ (LCIS) can help determine which patients need more formal and in-depth evaluation. This can be undertaken by the primary care clinician or a high-risk BC specialist and lead to shared decision making regarding screening and risk-reduction strategies. Some patients need not undergo extensive BC risk calculation if already considered high risk.
It is prudent to consider the patient’s personal values, individual risk factors, as well as differences in BC screening recommendations by societies and organizations (American Cancer Society [ACS], American College of Obstetrics and Gynecology, National Comprehensive Cancer Network [NCCN], and United States Preventative Services Task Force [USPSTF]).6–9 When individual risk is better understood, timing for appropriate initiation of screening, frequency of screening, implementation of lifestyle modifications for prevention, as well as recommendations for risk-reducing medications can be determined.
Patients who are found to be of high risk for BC, defined as an overall lifetime risk greater than 20%, are also candidates for enhanced BC screening.10 The ACS recommends that patients with elevated risk (based on family history risk calculations such as those from the International Breast Cancer Intervention study [IBIS]) should undergo annual magnetic resonance imaging (MRI) breast screening in addition to annual mammography,6 although this recommendation is not currently supported by USPSTF.7
Recent American Society of Clinical Oncology, IBIS, and USPSTF recommendations, support the use of risk assessment to determine benefit of certain endocrine therapies (eg, tamoxifen, raloxifene, anastrozole) for postmenopausal female patients with one or more of the following: diagnosis of atypical (ductal or lobular) hyperplasia or LCIS, an estimated 5-year risk (National Cancer Institute [NCI] Breast Cancer Risk Assessment Tool [BCRAT]) ≥ 3%, 10-year risk (IBIS/Tyrer-Cuzick risk calculator) ≥ 5%,8,9,11 or relative risk of ≥ 4 times the population risk for their age group if 40 to 44 years old, or > 2 times the population risk if 45 to 69 years old.8 Despite consistent national guidelines, less than 4% of candidates for endocrine therapy are currently prescribed these medications.12
In this article, we review BC risk factors, determinants of risk, and a pragmatic systematic approach to manage patients in the primary care setting.
KNOWN BREAST CANCER RISK FACTORS
Gene mutations/hereditary breast and ovarian cancer genetic syndromes
Approximately 8% to 10% of BCs are attributed to mutations in cancer susceptibility genes; more than 50% of germline mutations can be attributed to BReast CAncer gene (BRCA1) and BRCA2 mutations13,14 followed by mutations in genes such as checkpoint kinase 2 (CHEK2), ataxia-telangiectasia mutated (ATM), and partner and localizer of BRCA2 (PALB2). Despite the minority of BCs being attributable to genetics, BC attributable to mutations can be more lethal, and genetic counseling with discussion of genetic testing should be offered and available to patients with a significant family history of BC and/or ovarian cancer or known familial gene mutations, and in whom identifying a potential genetic mutation may change assessment and management options.13–15 For instance, patients with BRCA1 and BRCA2 should seriously consider surgical options for risk reduction, whereas BC from mutations in genes such as ATM, CDH1, CHEK2, NBN, NF1, PALB2, or STK11 can be followed by enhanced screening with breast MRI in conjunction with mammography.14,15 There are other gene mutations (such as BARD1, MSH2, MLH1, MSH6, PMS2, EP-CAM, BRIP1, RAD51C, RAD51D) without clear evidence supporting increased lifetime risk of BC, and thus guidelines for screening in these populations are unclear at this time.14
History of high-risk breast lesions
Atypical hyperplasia, which includes atypical ductal hyperplasia and atypical lobular hyperplasia as well as LCIS are characterized by dysplastic proliferation of epithelial mammary cells and differentiated based on histologic patterns and cytology seen on pathology. These patterns are significant risk factors for BC. Atypical hyperplasia is identified in around 10% of all benign breast biopsies.13,16,17
In the Mayo Benign Breast Disease Cohort and the Nashville Breast Cohort, incidence of BC in patients with atypical hyperplasia without chemoprevention was found to be around 1% to 2% per year17 with a cumulative incidence of BC of 30% at 25 years.18 Younger age at diagnosis of atypical hyperplasia is associated with increased likelihood of developing BC, as is increased foci of atypical hyperplasia on pathology.18
LCIS is associated with an increased risk of BC to varying degrees from 3- to 8-fold higher risk when compared with the general population, regardless of whether the primary lesion has been removed.19 Using data from the National Surgical Adjuvant Breast and Bowel Project P-1 Study, it was found that there was a 1.3% annual risk of development of invasive BC among patients with LCIS.20
Personal history of thoracic radiation
Ionizing radiation is a recognized risk factor for development of BC; this has been observed in the past in people exposed to atomic explosions such as Hiroshima or Nagasaki21 as well as in patients exposed to radiation treatments for diseases such as Hodgkin disease.22,23 Risk is inversely associated with age at radiation exposure and increased in women exposed to radiation before age 20 years compared with patients without a history of exposure.23–27 Personal risk in these patients has been shown to be as high as 56.7-fold greater than in the general population.28,29
Mantle radiation therapy is a form of extended field radiation and refers to radiation therapy that is administered to the mantle field that encompasses lymph nodes in the neck, chest, mediastinum, and axillary regions with the breast receiving about 3% to 15% of the administered dose.30
Most studies demonstrate increased BC risk 10 to 15 years following radiation treatment with development of secondary BC being rare within 10 years of treatment.27,30 Current guidelines recommend that patients who underwent thoracic radiation treatment between the ages of 10 and 30 begin annual screening MRI in addition to mammogram beginning 8 to 10 years after undergoing radiation treatment.9,29,31
Age/menopause
As more risk factors associated with BC are discovered, age remains one of the most significant.1,13 BC is most frequently diagnosed among women ages 65 to 74 with median age of diagnosis at 63.16 Based on data from 2015 to 2017, 12.9% of women will receive a diagnosis of BC at some point during their lifetime.16 Age-related BC risk according to the NCI Surveillance, Epidemiology, and End Results database between 2013 and 2017 shows increasing risk associated with each decade increase (Table 1).16
Annual breast cancer case distribution by age
Breast density
Dense breast tissue is very common, with 35% to 50% of the population being categorized as having dense breast tissue based on American College of Radiology Breast Imaging Reporting and Database System scoring.32 Increased breast density has been shown to be an independent risk factor for the development of BC. The presence of extremely dense breast tissue on mammogram purports a 4- to 6-fold increase in BC risk compared with almost entirely fatty breast tissue.5 Owing to this significantly increased risk, breast density has been added to the most recent IBIS risk calculator and has been shown to increase accuracy of the model.5 In addition to increased BC risk with increased density, mammographic sensitivity is significantly decreased32; therefore, consideration of density as a component of risk, particularly in patients with other risk factors, is important.
First-degree relatives with breast cancer
Family history is a well-recognized risk factor for development of BC. A first-degree relative (eg, mother, sister, daughter) with BC increases an individual’s relative risk of developing BC to 1.7 when compared with patients without an affected first-degree relative; this relative risk increases to 5 when two first-degree relatives are affected.13 Risk is further increased with younger age of diagnosed family members.
The risk ratio for BC was analyzed on the basis of number of first-degree relatives being affected, with a risk ratio of 1.80 (99% floated confidence interval [FCI] 1.69–1.91) for patients with one affected first-degree relative having BC, 2.93 (99% FCI 2.36–3.64) for patients with two first-degree relatives, and 3.90 (99% FCI 2.03–7.49) for patients with three or more first-degree relatives.33 Overall, 12.9% of patients with BC reported having at least one first-degree relative having BC whereas 7.3% of controls reported having at least one affected first-degree relative.33 Thus, while having a family history of BC in at least one first-degree relative increases BC risk, most patients with a family history of BC will not go on to develop BC themselves.
Obesity
Obesity is known to be correlated with increased risk of several malignancies, including BC.34 The types of BC, namely hormone receptor (HR)-positive or HR-negative BC and the association with obesity can be further stratified by menopausal status. Obese premenopausal patients have not been shown to be at increased risk of HR-positive malignancy; however, they do appear to be at an increased risk of HR-negative/triple-negative and inflammatory cancers.34
Obese postmenopausal patients, however, are at a significantly increased risk of HR-positive BC.35 The Million Woman Study followed 1.2 million women in the United Kingdom and demonstrated a 39% increased risk of HR-positive BC for postmenopausal women with a BMI ≥ 30.35 Others have demonstrated that increased waist circumference and waist-to-hip ratio are also indicative of an increased risk for estrogen receptor (ER)-positive/progesterone receptor (PR)-positive cancers. Similarly, data from the Women’s Health Initiative Observational Study showed that patients with a BMI > 31.1 had an increased relative risk of postmenopausal BC (relative risk 2.52, 95% CI 1.62–3.93) compared with women with a BMI < 22.6.36 This association is postulated to be secondary to increased circulating estrogen levels and secondary to peripheral conversion of estrogen precursors to estrogen in adipose tissue despite the menopausal state resulting in decreased estrogen levels.37 Furthermore, hyperinsulinemia secondary to weight gain may increase growth factors and cytokine activation resulting in a microenvironment favorable to tumor development. Accordingly, postmenopausal obesity is not as clearly associated with HR-negative BC.34
Weight loss has been associated with lower BC risk.34 Weight loss after 18 years as well as after menopause have both independently demonstrated a decrease in postmenopausal BC risk.34 Additionally, bariatric surgery was shown to reduce BC incidence at 5 years postoperatively.34 These data can be used to counsel patients regarding current risk, as well as possible incentive to pursue weight loss in the future.
METHODS TO EVALUATE RISK
Breast cancer risk calculators
Several BC risk calculators exist; however, few are used in clinical practice regularly. The two most commonly used BC risk calculators in the United States—and what we use regularly in our practice—are the National Cancer Institute BCRAT, also known as the Gail Model, and the IBIS/Tyrer-Cuzick Risk Model calculator. Both can be used to identify candidates for risk-reducing medications and for supplemental MRI screening.2,5,38–42
The BCRAT (https://bcrisktool.cancer.gov) is validated for patients ages 35 and older in many different populations2,38–40 but is not as useful for patients with a biopsy diagnosis of atypia as it underestimates overall risk.41 BCRAT can be used to calculate an estimated 5-year and lifetime risk and provide a population risk and not an individual risk assessment. It does not consider extensive family history, therefore is not recommended to determine need for enhanced screening with MRI.
The IBIS risk assessment tool (http://www.ems-trials.org/riskevaluator) considers reproductive history, body composition, and extensive family history; the most recent version includes mammographic breast density. A 5-year, 10-year, and lifetime risk estimate is available for patients under the age of 85.5 In contrast to the BCRAT, the IBIS calculator can be used to “qualify” patients for supplemental BC screening with MRI. However, this model tends to overestimate risk for patients with a biopsy diagnosis of atypia, and therefore, should not be used in this population.42
In the office setting, the BCRAT model offers a quick estimate of BC risk. However, the IBIS model is more comprehensive and includes a more in-depth family history. There are many models available including Claus, BRCAPRO and BOADICEA models.2–5
A SYSTEMATIC APPROACH TO RISK EVALUATION
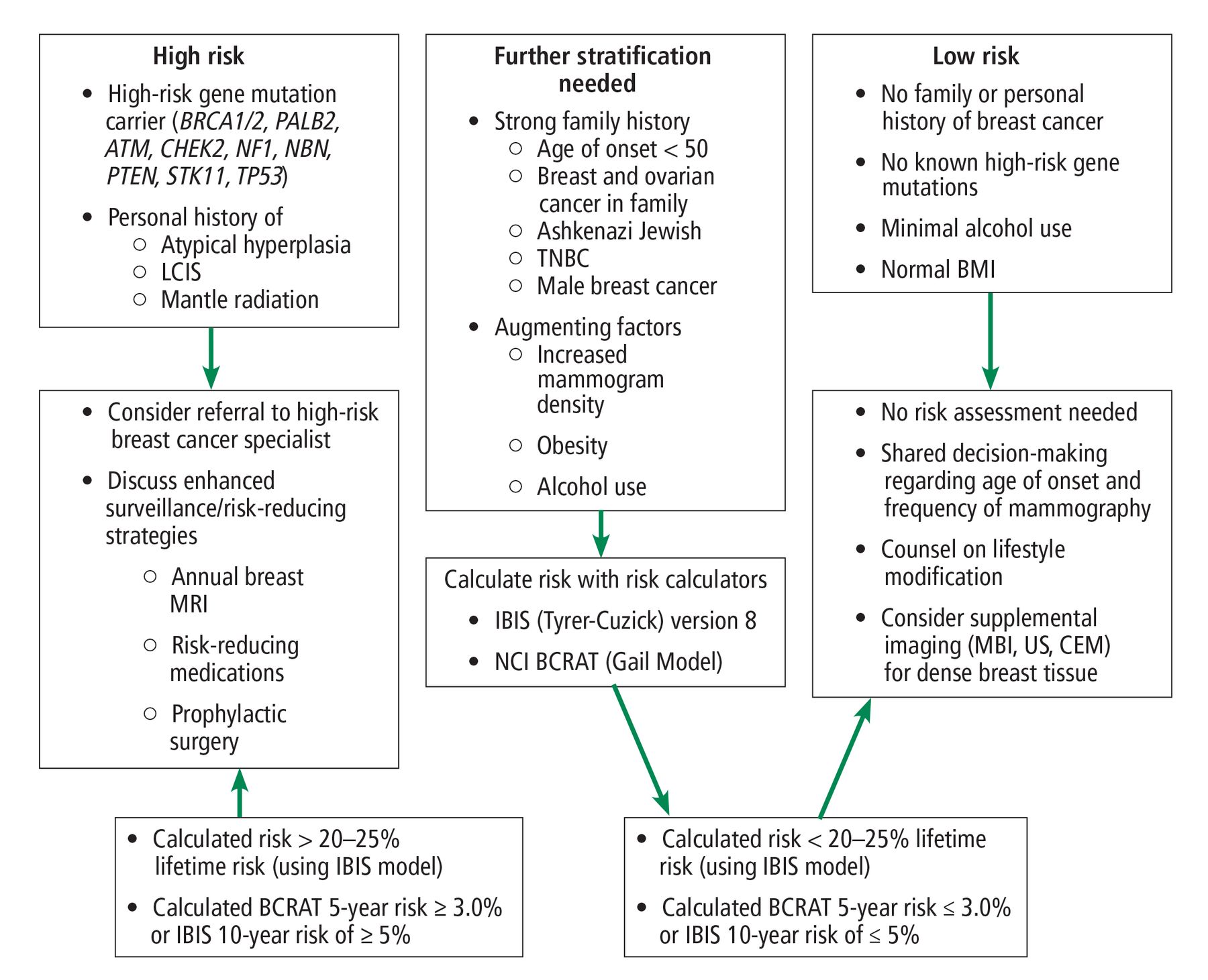
There is no standard approach to initiate BC risk assessment in a primary care office setting. We recommend that clinicians periodically reassess BC risk factors, beginning with the patient’s initial evaluation. Risk should be re-evaluated if patients have a family history of BC or ovarian cancer, and/or breast biopsy or baseline mammogram that demonstrates dense breast tissue, or if they present with a new diagnosis of cancer in the family. Assessment should include reproductive risk factors, prior high-risk breast lesions, exposure to ionizing radiation, lifestyle (eg, smoking, alcohol, diet, physical activity), and family history of cancer. Patients can then be divided into 3 major risk categories, with subsequent evaluation and recommendations appropriate to their level of risk (Figure 1).6,7,9,11,29,31
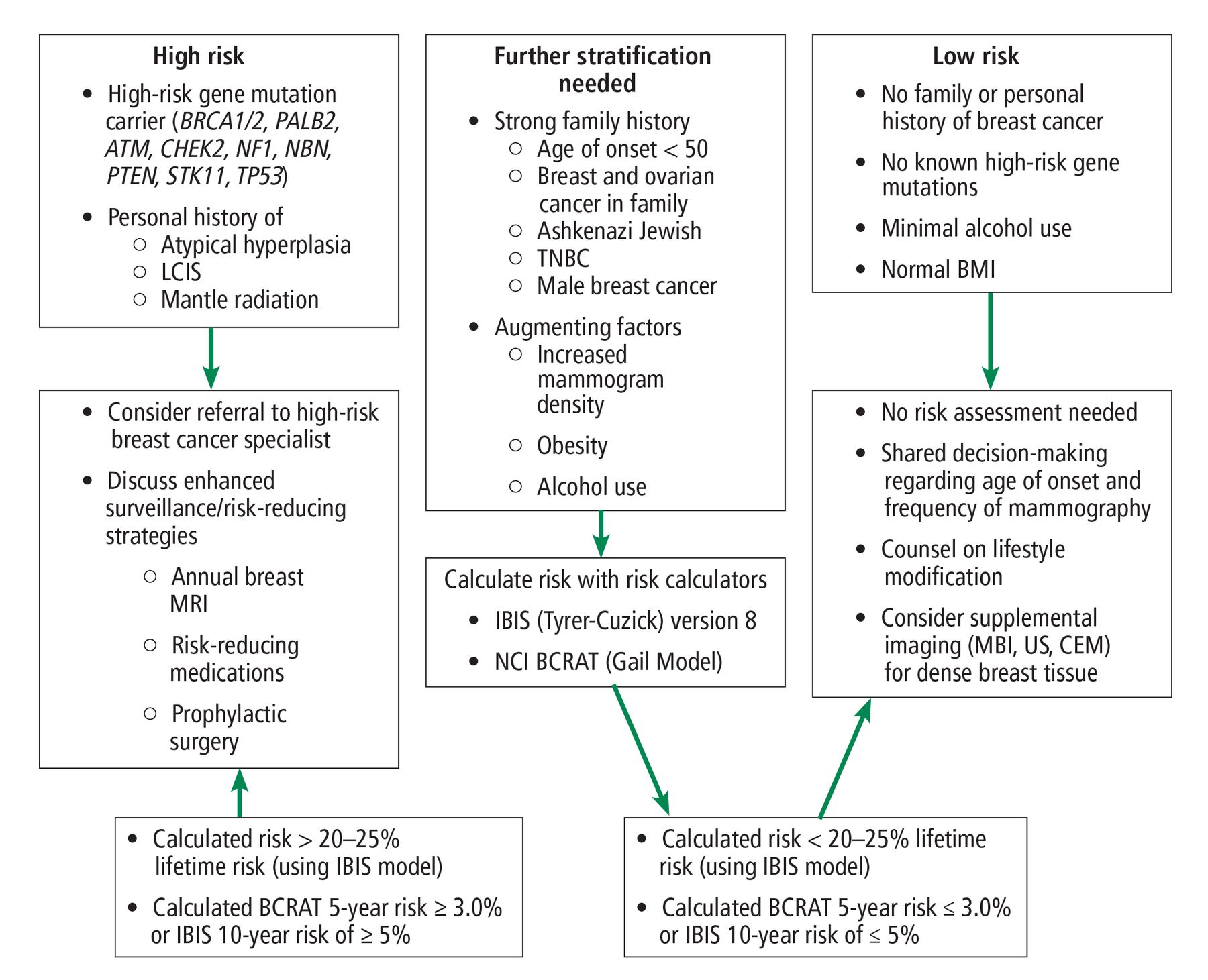
Systematic approach to breast cancer risk evaluation. A step-by-step approach to categorize patients who require further stratification vs patients needing referral to breast specialist.
ATM = arabidopsis thaliana homeobox gene 1; BCRAT = Breast Cancer Risk Assessment Tool; BMI = body mass index; BRCA = BReast CAncer gene; CEM = contrast-enhanced mammogram; CHEK = checkpoint kinase 2; IBIS = International Breast Intervention Study; LCIS = lobular carcinoma in situ; MBI = molecular breast imaging; MRI = magnetic resonance imaging; NBN = nibrin; NCI = National Cancer Institute; NF1 = neurofibromin; PALB = partner and localizer of BRCA; PTEN = phosphatase and tensin homolog; STK = serine/threonine kinase; TNBC = triple-negative breast cancer; TP = tumor protein; US = ultrasonography
The first step of evaluation should be to identify patients who have clearly significantly increased risk for BC and who would benefit from a referral to a high-risk BC specialist for counseling and surveillance. This would include patients with a known gene mutation, history of thoracic radiation, personal history of atypical hyperplasia or LCIS on a biopsy, and/or strong family history of breast and ovarian cancer suggestive of a gene mutation. Owing to known increased BC risk for patients with these conditions as well as inaccuracy of models regarding this risk, these patients would likely benefit from consultation with a high-risk BC specialist to determine the type and frequency of BC screening, to discuss options such as prophylactic mastectomy and preventive medications, and to review indications for genetic consultation and testing. It has also been shown that female patients at high risk are more likely to take risk-reducing medications after a referral to medical oncology/high-risk BC specialists.43
In patients without the above-mentioned high-risk factors, we recommend considering other risk factors. The USPSTF recommends applying the use of a risk assessment tool for any female patient with a family history of BC, ovarian, tubal, or peritoneal cancer or ancestrial association with BRCA1/2 gene mutations, such as Ashkenazi Jewish heritage.3 Additionally, the American College of Radiation and Society of Breast Imaging have recently published guidelines recommending that African American women undergo risk evaluation with consideration for genetic testing by the age of 30 years,44 including a discussion on supplemental screening with breast MRI for risk evaluation of all patients.44
For all patients, cancers on both maternal and paternal sides should be included in the history with special attention to BC at a young age and particular subtypes such as triple negative BC, BC in male family members, cancers in multiple sites. NCCN guidelines have been expanded to include family history in first- and second-degree relatives and potentially include extensive involvement of third-degree relatives. Additional risk factors discussed above can potentially augment that risk. Patients at higher risk could benefit the most from undergoing more formal BC risk stratification using the many validated BC risk assessment tools discussed above.
For patients who do not have significant family history but are found to have a higher-risk lifestyle (eg, obesity, smoking, excessive alcohol use), extensive risk evaluation with use of risk calculators is not necessarily needed. But these patients would clearly benefit from counseling regarding mitigation of these risk factors and reducing BC risk.
Some patients will come without any significant family history of BC or ovarian cancer and without significant lifestyle factors that contribute to BC risk. In this situation, no further risk stratification is indicated. We do recommend discussing society guidelines for BC screening in patients with average risk and using a shared decision-making approach to determining at what age and frequency patients undergo BC screening.
In conclusion, a systematic approach to risk assessment will allow the primary care clinician to identify female patients at high risk for BC and provide an opportunity for shared decision making regarding screening, enhanced screening, referrals to a specialty clinic, genetic counseling, and counseling on risk-reduction strategies including lifestyle modifications and risk-reducing medications. With knowledge and understanding of personal risks, patients may have a higher perceived benefit to intervention and are more likely to use risk-reducing treatment.43
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2022 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.