


Article Figures & Data
Figures
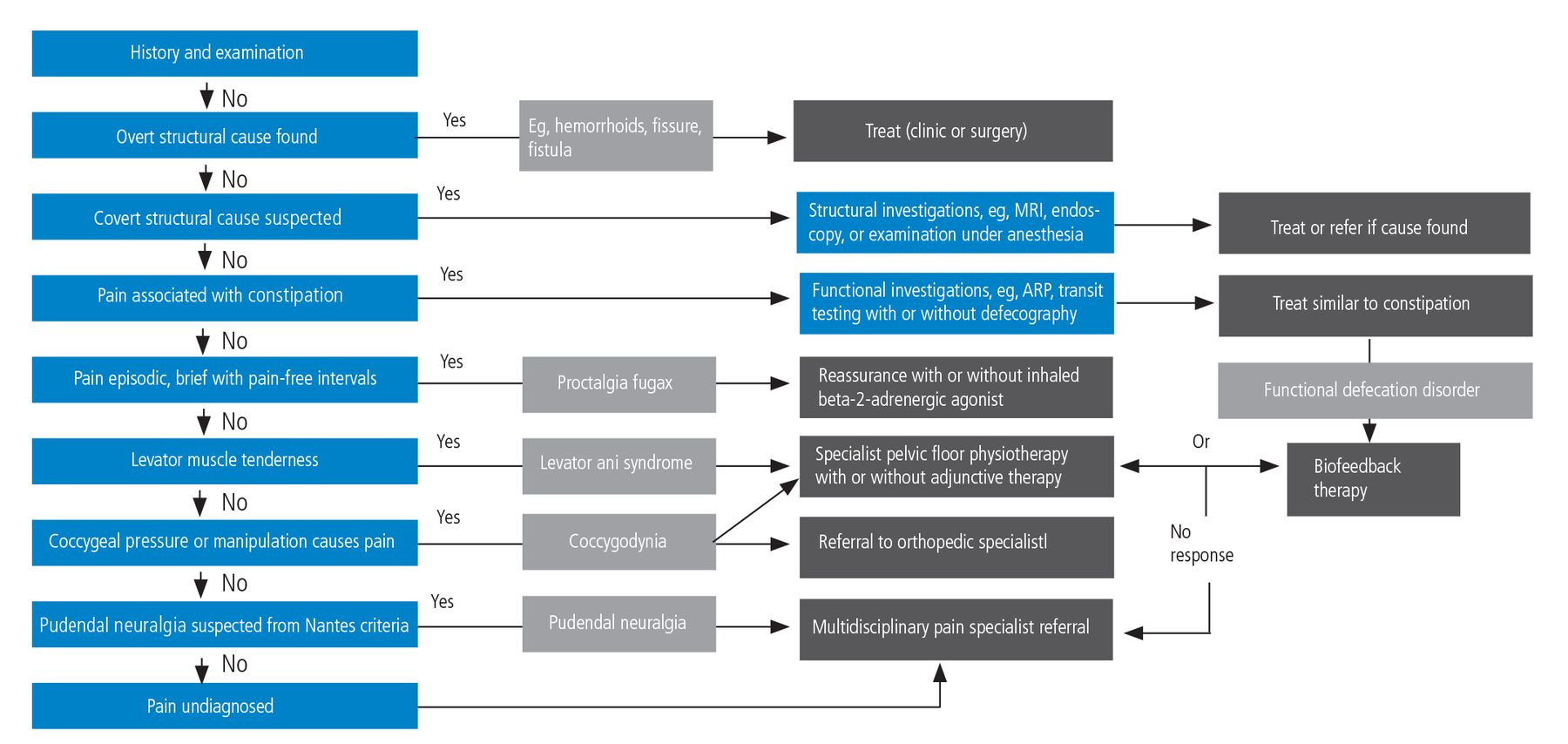
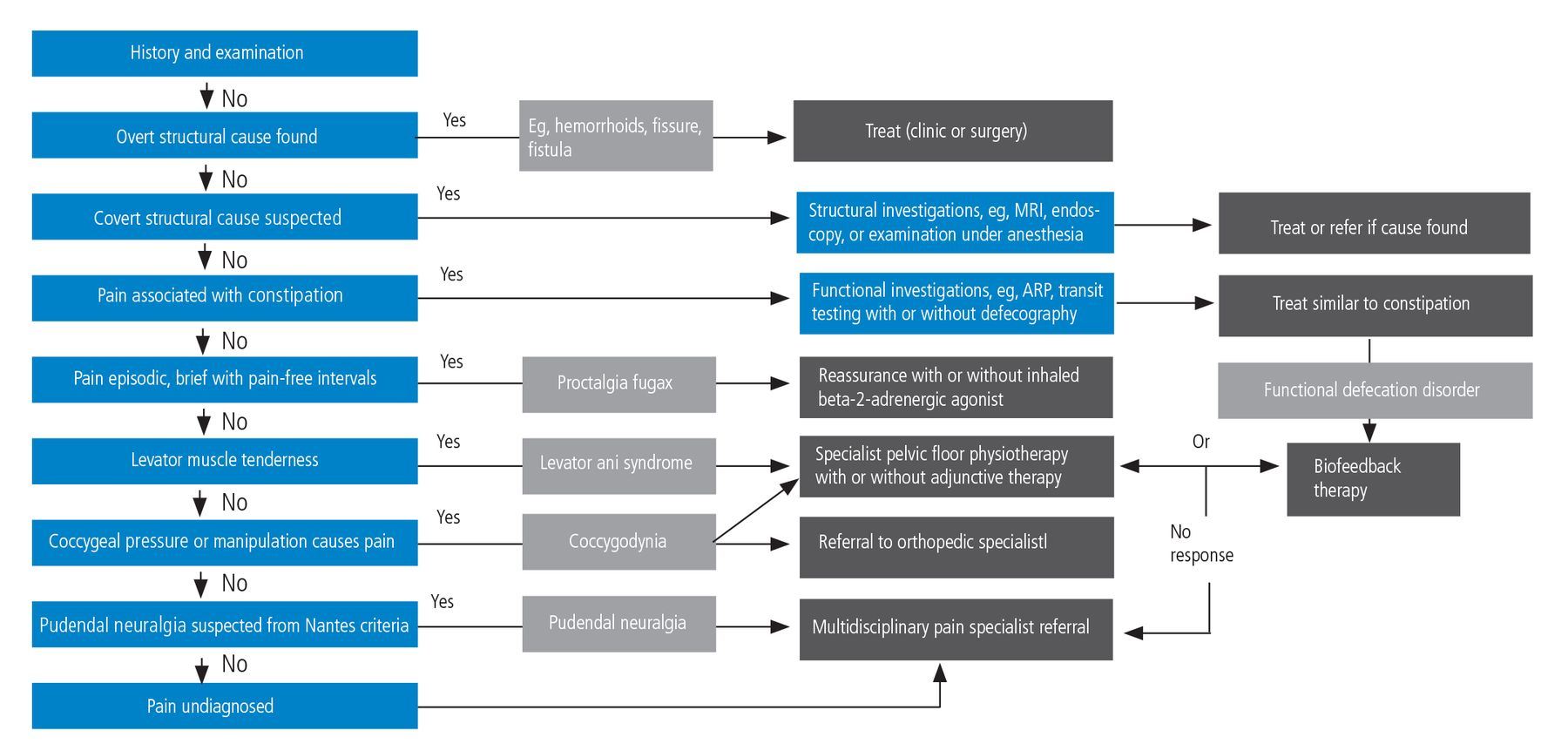
- Figure 1
Algorithm for diagnosis and management of chronic anal pain.
ARP = anorectal physiologic testing; MRI = magnetic resonance imaging
Based on information in reference 3.
Tables
Diagnostic category Diagnosis or syndrome Assumed etiology Main symptoms Examination findings Local anorectal conditions Fissure, perianal sepsis, tumor, ulcers, thrombosed hemorrohoids, severe proctitis Specific to disorder Common symptoms: Bleeding, discharge, lump, pruritis ani Overt findings (may require EUA) Functional anorectal conditions Proctalgia fugax Unknown Short-lasting (seconds or minutes) sharp deep rectal stabbing or cramping. No radiation. No anorectal pain between episodes No findings Levator ani syndrome Pelvic floor muscle tension or spasm Chronic (> 30 minutes) dull rectal ache or pressure sensation. Radiation to buttock, vagina, thigh. Other functional diagnoses common (eg, IBS, FDD, fibromyalgia) Tender puborectalis, replicates pain (usually left side) Unspecified functional anorectal pain Unknown Chronic (> 30 minutes) dull rectal ache or pressure sensation. Other functional diagnoses very common (eg, IBS, FDD, fibromyalgia) No findings Neuropathic pain syndromes Coccygodynia Coccyx trauma leading to peripheral sensitisation Perineal pain triggered by sitting Tender on pressure or manipulation of coccyx Pudendal neuralgia Pudendal nerve entrapment: peripherally generated or neuropathic pain Unilateral perineal pain with paresthesia.
Worse on sitting. Nantes criteria2Pain on transvaginal pressure on ischial spine Phantom rectum syndrome Neuropathic pain (deafferentation) Specific to disorder Specific to disorder Paroxysmal extreme pain disorder Neuropathic pain (genetic) Specific to disorder Specific to disorder EUA = examination under anesthesia; FDD = functional defecation disorder; IBS = irritable bowel syndrome
Author, year Diagnosis Intervention Comparator(s) Main findings Eckardt et al 199610 N = 16 (crossover) Proctalgia fugax Inhaled salbutamol Placebo Salbutamol shortened duration of severe pain vs placebo (P = .019); effect most marked in patients having prolonged attacks Abbott et al 200611 N = 60 Pelvic floor myofascial pain Botulinum toxin A; pelvic floor injection Placebo: saline injection Significant reductions in dyspareunia and pelvic floor pressure with both botulinum toxin and placebo Dessie et al 201912 N = 59 Myofascia pelvic pain Botulinum toxin A; pelvic floor injection Placebo: saline injection No significant clinical effect Rao et al 200913 N = 10a (crossover) Levator ani syndrome Botulinum toxin A; transanal injection Placebo No effect of either botulinum toxin or placebo Chiarioni et al 201014 N = 157 Levator ani syndrome Biofeedback EGS; levator muscle massage 12-month results
Pain days: 14.7 (baseline)
3.3 (biofeedback) vs 8.9 (EGS) and 13.3 (massage)
Pain intensity: 6.8 (baseline)
1.8 (biofeedback) vs 4.7 (EGS) and 6.0 (massage)
Adequate relief: 87% (biofeedback) vs 45% (EGS) and 22% (massage)Zoorob et al 201515 N = 29 Levator ani syndrome Steroid injections in levator ani trigger points Pelvic floor physiotherapy Both groups improved equally (60% achieved 50% reduction in symptoms) ↵a Only 7 had complete data.
EGS = electrogalvanic stimulation
Category Examples Level of Evidence Comments Behavior therapy Biofeedback to improve defecation dynamics B Most effective treatment for LAS in single RCT14 Muscle relaxant Electrogalvanic stimulation B More effective than massage in single RCT14; benefits decrease in long-term Muscle relaxant Diazepam C Poorly effective in the long-term; addictive potential Muscle relaxant Digital massage of puborectalis muscle D No standardized methodology; often provided with sitz bath Anticholinergic Botulinum toxin A injection B Ineffective as transvaginal or transanal injection in three RCTs11–13 Anti-inflammatory Pelvic floor muscle steroid Injection D Equally effective as physiotherapy in pilot RCT15 Antidepressants Amitriptyline D Unclear mechanism of action; diverse dosage Neuromodulation Sacral neuromodulation D Conflicting results in small observational studies LAS = levator ani syndrome; RCT = randomized controlled trial
Essential criteria
Pain in the pudendal nerve area from the anus to the penis or clitoris
Pain is predominantly experienced while sitting
Pain does not wake the patient at night
Pain with no objective sensory impairment
Pain is relieved by diagnostic pudendal nerve block
Complementary diagnostic criteria
Burning, shooting, stabbing pain, numbness
Allodynia or hyperalgesia
Rectal or vaginal foreign body sensation
Worsening of pain during the day
Predominantly unilateral pain
Pain is triggered by defecation
Presence of exquisite tenderness on palpation of the ischial spine
Clinical neurophysiology findings in men or nulliparous women
Exclusion criteria
Exclusively coccygeal, gluteal, pubic, or hypogastric pain
Pruritus
Exclusively paroxysmal pain
Imaging abnormalities able to account for the pain
Associated signs not excluding the diagnosis
Buttock pain on sitting
Referred sciatic pain
Pain referred to the medial aspect of the thigh
Suprapubic pain
Urinary frequency and/or pain on a full bladder
Pain occurring after ejaculation
Dyspareunia and/or pain after sexual intercourse
Erectile dysfunction
Normal clinical neurophysiology
Reprinted with permission from John Wiley & Sons. From Labat JJ, Riant T, Robert R, Amarenco G, Lefaucheur JP, Rigaud J. Diagnostic criteria for pudendal neuralgia by pudendal nerve entrapment (Nantes criteria). Neurourol Urodyn 2008; 27(4):306–310. doi:10.1002/nau.20505.2




{kind=link}