


Article Figures & Data
Figures
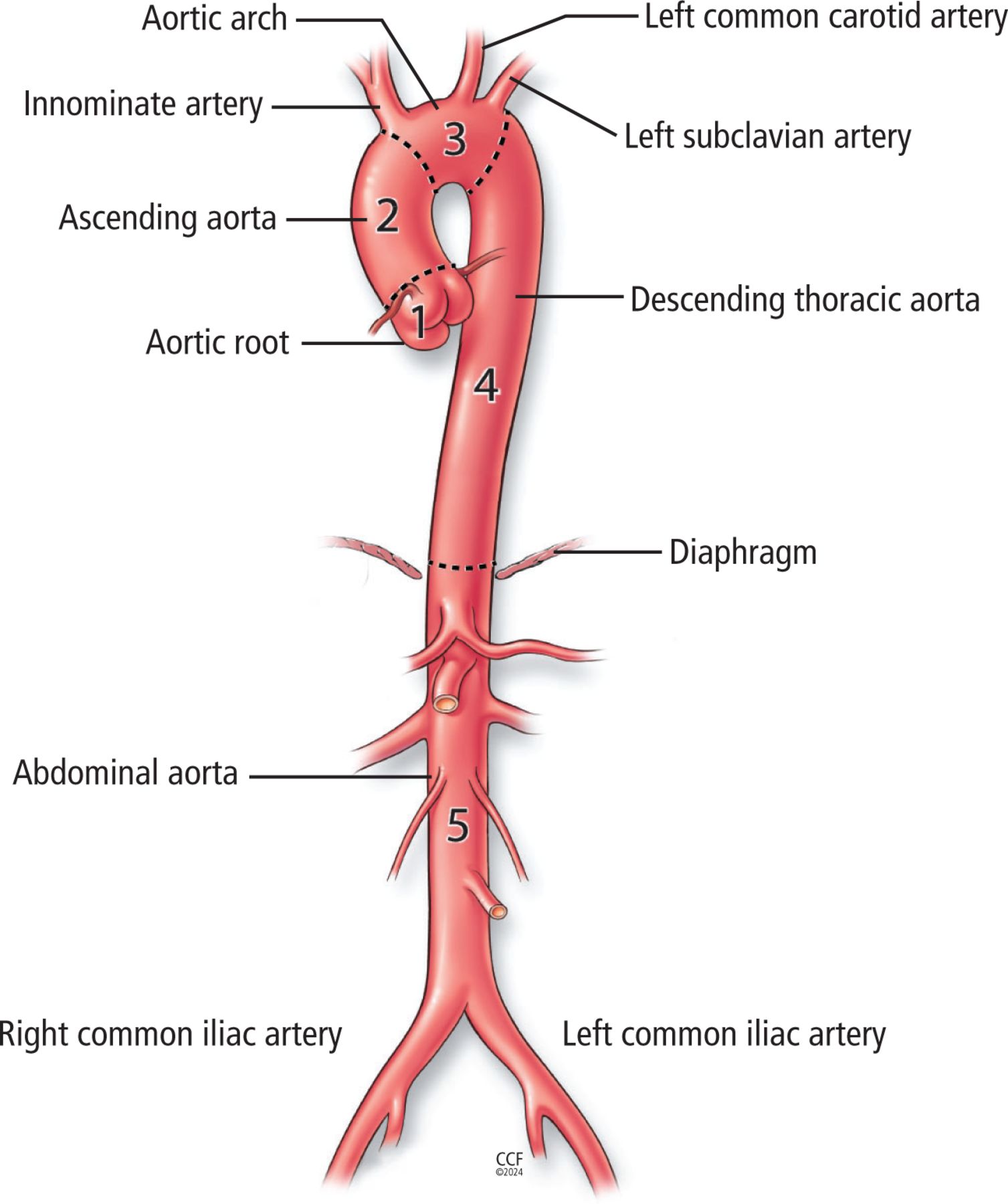
- Figure 1
Anatomy of the aorta. The 5 segments of the aorta are the (1) aortic root (from the aortic valve through the sinotubular junction), (2) ascending aorta (from the sinotubular junction to the innominate artery), (3) aortic arch (from the innominate through the left subclavian artery), (4) descending thoracic aorta (left subclavian artery to the diaphragm), and (5) abdominal aorta (diaphragm to the iliac bifurcation).
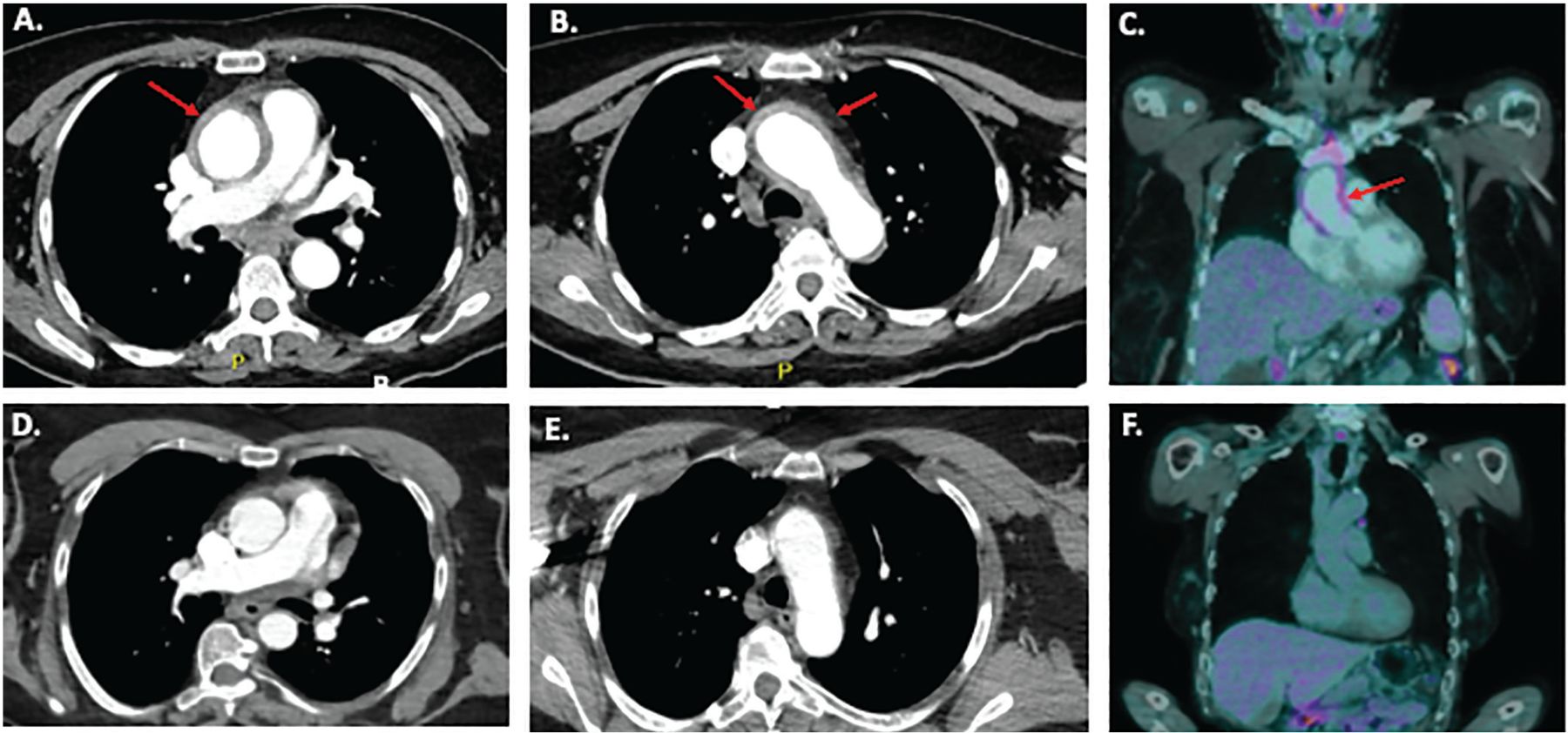
- Figure 2
Imaging studies in a 55-year-old female who presented with fever, chest pain, and a C-reactive protein level of 33 mg/L (normal range < 8 mg/L). (A and B) Computed tomography angiography (CTA) of the chest and abdomen showed diffuse circumferential thickening (up to 6 mm) of the wall of the ascending aorta through the aortic arch consistent with aortitis. Red arrows indicate circumferentially thickened and FDG-avid aortic wall in the ascending aorta and aortic arch. There were no symptoms or physical signs of an underlying systemic vasculitis or autoimmune disease. Laboratory tests were normal or negative, including blood cultures, antinuclear antibody, extractable nuclear antigen, anti-double-stranded DNA, complement components 3 and 4, antineutrophil cytoplasmic antibody, serum immunoglobulin G4 level, urinalysis, interferon-gamma release assay for tuberculosis, and serology for hepatitis B and C and syphilis. (C) Positron-emission tomography with computed tomography (PET-CT) showed longitudinal grade 3 18F-fluorodeoxyglucose (FDG) uptake (ie, more than in the liver) in the ascending aorta and arch, consistent with active aortitis. Prednisone 60 mg daily was initiated, symptoms improved, and C-reactive protein level returned to normal. (D and E) CTA images of a normal ascending aorta and arch, shown for comparison. (F) PET-CT images of a normal ascending aorta without pathologic FDG uptake.
- Figure 3
Approach to aortitis found on imaging or tissue.
Based on information from references 4–8,10–29.



Tables
Diagnosis Age at onset Tissue pattern Core symptoms and signs Typical imaging features Staphylococcus, Streptococcus, Salmonella, or Pseudomonas infection Any Suppurative Fever, constitutional symptoms
History of antecedent infection
High erythrocyte sedimentation rate and C-reactive protein
Positive blood cultures
Positive tissue stain and cultureUsually a single lesion Syphilis Decades after primary infection Lymphoplasmacytic Possible history of untreated primary syphilis
Positive syphilis serology
Positive tissue stain and cultureUsually a single lesion in the thoracic aorta Coxiella burnetii infection (Q fever) Usually older, occurs months to years after primary infection Granulomatous Possible fever, abdominal pain, high C-reactive protein and erythrocyte sedimentation rate
Positive immunoglobulin G
Positive polymerase chain reaction of aortic tissueMore often in the abdominal than the thoracic aorta
Predilection for existing aneurysms or vascular graftsFungal or mycobacterial infection Any Granulomatous (may be suppurative) Constitutional symptoms
Disseminated infection
Positive tissue stain and cultureThoracic or abdominal aorta Based on information from references 10–12.
Diagnosis Age at onset Tissue pattern Core symptoms and signs Typical imaging features Large-vessel vasculitis Giant cell arteritis > 50 years Granulomatous Cranial or limb ischemia
Constitutional symptoms
High erythrocyte sedimentation rate and C-reactive protein
Positive temporal artery biopsy
Positive large-vessel imagingMore often in the thoracic than the abdominal aorta, and often branch vessel involvement Takayasu arteritis < 60 years Granulomatous Cranial or limb ischemia
Constitutional symptoms with or without high erythrocyte sedimentation rate and C-reactive protein
Positive large-vessel imagingMore often in the thoracic than the abdominal aorta, and usually branch vessel involvement Clinically isolated aortitis Any Most often granulomatous, but can be any pattern No constitutional symptoms or symptoms of systemic vasculitis or autoimmune rheumatic disease
Normal C-reactive protein and erythrocyte sedimentation rate, negative serologyMost often in the thoracic aorta
Can involve other segments
No branch vessel involvementSmall-vessel or medium-vessel vasculitis Granulomatosis with polyangiitis Any Granulomatous, may see neutrophils and necrosis Ear, nose, throat, lung, renal vasculitis most commonly, with or without involvement of skin, joints, nerves
High erythrocyte sedimentation rate and C-reactive protein, positive antineutrophil cytoplasmic antibody, active urinalysis, positive lung and ear, nose, and throat imaging, positive tissue biopsyThoracic or abdominal aorta with or without branch vessels Eosinophilic granulomatosis with polyangiitis Any Granulomatous, may see eosinophils Allergic rhinitis, asthma, mononeuritis multiplex, myocarditis, skin vasculitis most commonly
Peripheral eosinophilia, active urinalysis, high erythrocyte sedimentation rate and C-reactive protein, positive lung imaging
Positive antineutrophil cytoplasmic antibody in 50% of cases, positive tissue biopsyThoracic or abdominal aorta with or without branch vessels Behçet syndrome Any Mixed Oral or genital ulcers, uveitis, pathergy
High C-reactive protein
SeronegativeThoracic or abdominal aorta
Pulmonary artery aneurysmsBased on information from references 4–8,10–19.
Diagnosis Age at onset Tissue pattern Core symptoms and signs Typical imaging features IgG4-related disease Any (typically older) Lymphoplasmacytic Lacrimal, salivary gland swelling, pancreatitis, retroperitoneal fibrosis most commonly
C-reactive protein often normal
Elevated serum IgG4, positive tissue IgG4More often in the abdominal than the thoracic aorta
May have periaortitis or retroperitoneal fibrosisRheumatoid arthritis Any, usually long-standing rheumatoid arthritis Granulomatous Small joint, symmetrical polyarthritis
Usually high erythrocyte sedimentation rate and C-reactive protein, positive rheumatoid factor, positive anti-cyclic citrullinated peptide
Erosions on radiographs of hands and feetThoracic or abdominal aorta Spondyloarthritis Any Lymphoplasmacytic Inflammatory back pain
Usually high erythrocyte sedimentation rate and C-reactive protein
Positive human leukocyte antigen B27, positive radiographs or magnetic resonance imaging of sacroiliac joint and spineAortic root with or without aortic insufficiency Systemic lupus erythematosus Any Lymphoplasmacytic Photosensitivity, rash, arthritis, nephritis
Positive antinuclear antibody, extractable nuclear antigen, and anti-double-stranded DNA; low complement components 3 and 4; active urine studiesThoracic or abdominal aorta with or without branch vessels Relapsing polychondritis Any Mixed Chondritis, scleritis, tracheomalacia
High C-reactive protein, seronegativeAortic root and ascending aorta Cogan syndrome Any (often younger) Mixed Interstitial keratitis, hearing loss, vestibular dysfunction, high C-reactive protein Ascending aorta and arch, with or without aortic insufficiency Sarcoidosis Any Granulomatous (well-formed nonnecrotizing granulomas) Lung, lymph node, musculoskeletal, hematologic, central nervous system, cardiac
High C-reactive protein
May have high serum or urine calcium, positive lung or cardiac imaging, positive tissue biopsyThoracic or abdominal aorta Drug exposure (granulocyte-colony stimulating factor, immune checkpoint inhibitors) Any Unknown (usually radiographic diagnosis) Fever, pain in back, chest, or abdomen, high C-reactive protein, relapsing polychondritis, history of exposure
Resolution of imaging changes with drug withdrawal with or without prednisoneThoracic and abdominal aorta Ig = immunoglobulin
Based on information from references 10–12,20–29.




{kind=link}
{kind=link}
{kind=link}