


ABSTRACT
The term metabolic surgery describes bariatric surgical procedures used primarily to treat type 2 diabetes and related metabolic conditions. Originally, bariatric surgery was used as an alternative weight-loss therapy for patients with severe obesity, but clinical data revealed its metabolic benefits in patients with type 2 diabetes. Metabolic surgery is more effective than lifestyle or medical management in achieving glycemic control, sustained weight loss, and reducing diabetes comorbidities. Perioperative adverse events are similar to other gastrointestinal surgeries. New guidelines for type 2 diabetes expand use of metabolic surgery to patients with a lower body mass index.
Randomized clinical trials have shown that metabolic surgery is statistically superior to medical treatment in achieving targeted glycemic levels along with improvements in weight loss, remission of metabolic syndrome, reduction in medications, and improvements in lipid levels.
The safety of metabolic and bariatric surgery has significantly improved with the advent of laparoscopic surgery, resulting in complication profiles similar to those of cholecystectomy and appendectomy.
Metabolic surgery is now recommended as standard treatment option for type 2 diabetes in patients with body mass index levels as low as 30 kg/m2.
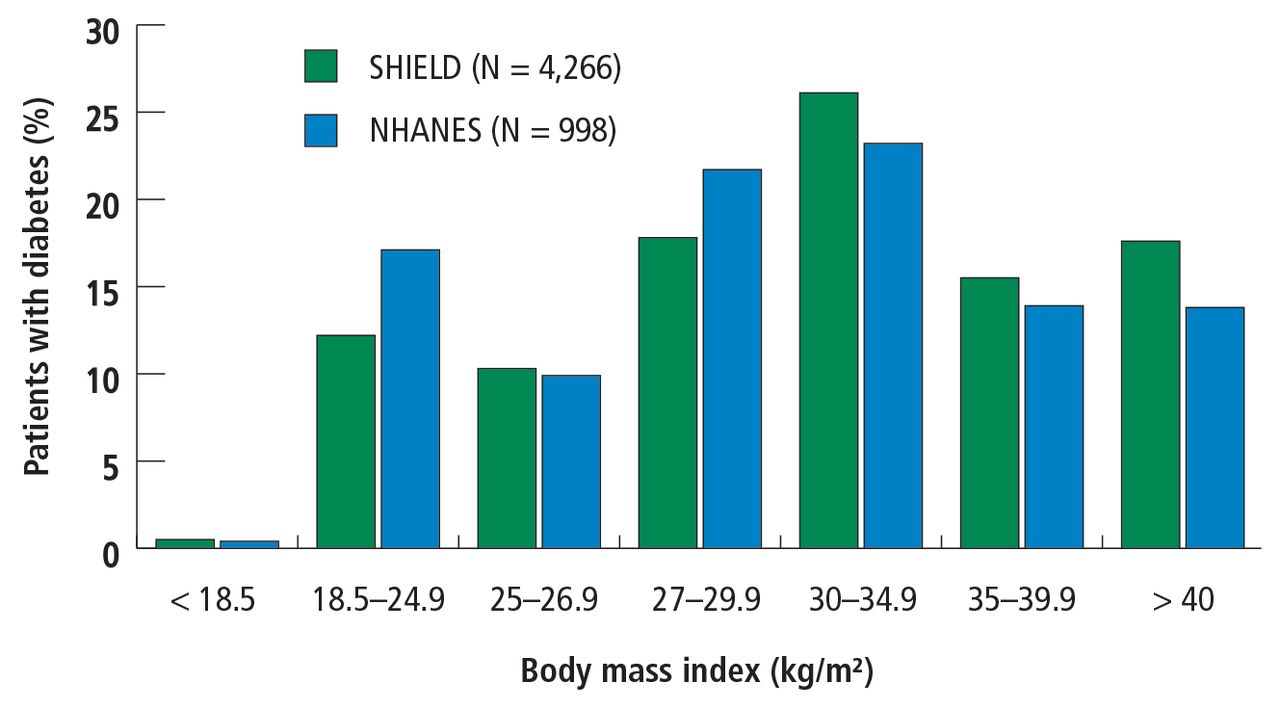
Type 2 diabetes mellitus (DM) and obesity are chronic diseases that often coexist. Combined, they account for tremendous morbidity and mortality. Approximately 85% of all patients with type 2 DM have a body mass index (BMI) categorizing them as overweight (BMI 25.0–29.9 kg/m2) or obese (BMI > 30.0 kg/m2) (Figure 1).1 Obesity is strongly associated with diabetes and is a major cause of insulin resistance that leads to the cascade of hyperglycemia, glucotoxicity, and beta-cell failure, which ultimately leads to the development of microvascular (neuropathy, nephropathy, retinopathy) and macrovascular (myocardial infarction, stroke) complications. Treatment guidelines emphasize that both diabetes and obesity should be treated to optimize long-term outcomes.2–5 Metabolic surgery is the only diabetes treatment proven to result in long-term remission in 23% to 60% of patients depending upon preoperative duration of diabetes and disease severity. This review presents the evidence supporting use of metabolic surgery as a primary treatment for type 2 DM, potential mechanisms for its effects, associated complications, and recommendations for its use in expanded patient populations.
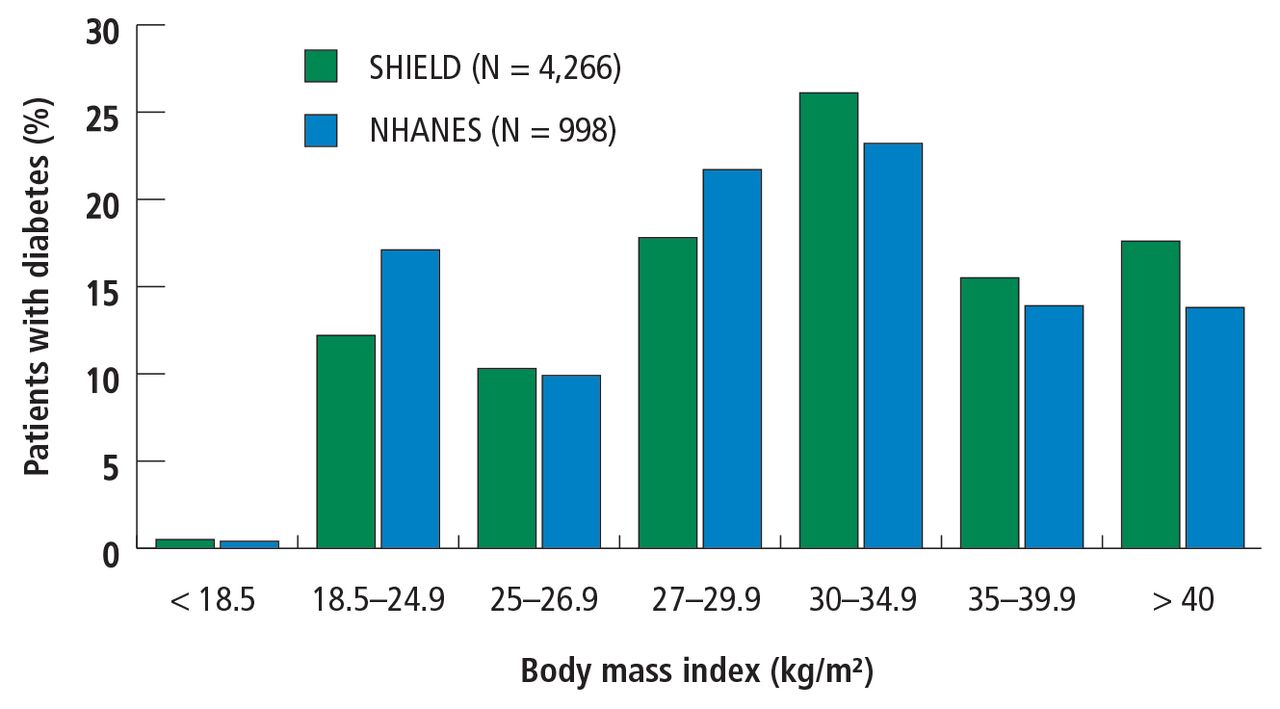
Relative distribution of body mass index of patients with diabetes.
SHIELD = Study to Help Improve Early Evaluation and Management of Risk Factors Leading to Diabetes (2004); 4,266 of 127,420 survey respondents with diabetes (type 1 = 368; type 2 = 3,898).
NHANES = National Health and Nutrition Examination Survey (1999–2002); 998 of 11,441 survey repondents with diabetes (type 1 and 2).
Data from Bays et al.1
LIMITATIONS OF LIFESTYLE MANAGEMENT AND MEDICATIONS
First-line therapy with lifestyle management and second-line therapy with medications, including oral agents and insulin, are the mainstays of type 2 DM therapy. Although these approaches have reduced hyperglycemia and cardiovascular mortality, many patients have poor glycemic control and develop severe diabetes-related complications. A study using data from the National Health and Nutrition Examination Survey (N = 4,926) to evaluate success rates of lifestyle management plus drug therapy found that just 53% of patients with type 2 DM maintained a hemoglobin A1c (HbA1c) below 7%.6 Similarly, only 51% of those patients achieved a systolic and diastolic blood pressure less than 130/80 mm Hg, and only 56% achieved a low-density lipoprotein cholesterol level less than 100 mg/dL. Altogether, only 19% of the study cohort achieved all 3 therapy targets. Documented limitations of lifestyle counseling and drug therapy include behavior maladaptation, limitations in drug potency, nonadherence to medications, adverse effects, and economic deterrents.7
METABOLIC SURGERY FOR TYPE 2 DM
For patients with obesity and type 2 DM in whom lifestyle management and medications do not achieve desired treatment goals, bariatric surgery has emerged as the most effective treatment for attaining significant and durable weight loss. These gastrointestinal (GI) procedures, which reduce gastric volume with or without rerouting nutrient flow through the small intestine, were developed to yield long-term weight loss in patients with severe obesity. It is now known that they also cause dramatic improvement or remission of obesity-related comorbidities, especially type 2 DM. Research has shown that these effects are not only secondary to weight loss but also depend on neuroendocrine mechanisms secondary to changes in GI physiology. For these reasons, bariatric surgery is increasingly used with the primary intent to treat type 2 DM or metabolic disease, a practice referred to as metabolic surgery.
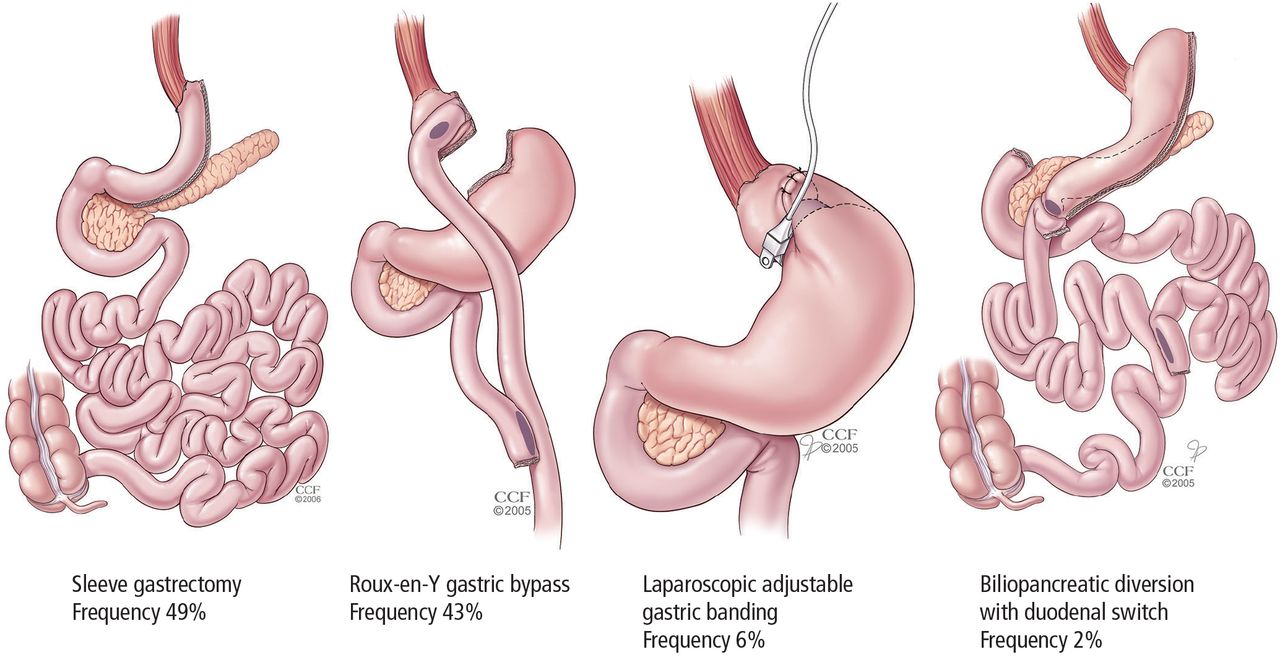
Between 150,000 and 200,000 bariatric procedures are performed annually in the United States, and nearly 500,000 worldwide.8 The most common procedures are sleeve gastrectomy (SG, 49%), Roux-en-Y gastric bypass (RYGB, 43%), laparoscopic adjustable gastric banding (LAGB, 6%), and bilio pancreatic diversion with duodenal switch (BPD-DS, 2%) (Figure 2).9,10 The development of laparoscopic, minimally invasive approaches to these procedures, starting in the mid-1990s, has significantly reduced rates of perioperative morbidity and mortality.

Most common metabolic surgical procedures.
For more than 2 decades, indications for metabolic surgery reflected guidelines from a 1991 National Institutes of Health (NIH) consensus conference, which suggested considering surgery only in patients with a BMI of 40 kg/m2 or greater or a BMI of 35 kg/m2 or greater and significant obesity-related comorbidities.11 Guidelines published in 2013 expanded the recommendations to include adults with a BMI of at least 35 kg/m2 and an obesity-related comorbidity, such as diabetes, who are motivated to lose weight.4 These recommendations were primarily designed to guide the use of surgery as a weight-loss intervention for severe obesity. However, guidelines published in 2016 support use of metabolic surgery as a specific treatment for type 2 DM.5
Potential mechanisms resolving type 2 DM: More than weight loss
Bariatric surgery has been shown to have profound glucoregulatory effects. These include rapid improvement in hyperglycemia and reduction in exogenous insulin requirements that occur early after surgery and before the patient has any significant weight loss.12,13 Additionally, experiments in rodents showed that changes to GI anatomy can directly influence glucose homeostasis, independently of weight loss and caloric restriction.14
Although the exact molecular mechanisms underlying the effects of metabolic surgery on diabetes are not fully understood, many factors appear to play a role, including changes in bile acid metabolism, GI tract nutrient sensing, glucose utilization, insulin resistance, and intestinal microbiomes.15 These changes, acting through peripheral or central pathways, or perhaps both, lead to reduced hepatic glucose production, increased tissue glucose uptake, improved insulin sensitivity, and enhanced beta-cell function. A constellation of gut-derived neuroendocrine changes, rather than a single overarching mechanism, is the likely mediator of postoperative glycemic improvement, with the contributing factors varying according to the surgical procedure.
METABOLIC SURGERY OUTCOMES
Weight loss
Long-term reduction of excess body fat is a major goal of metabolic and bariatric surgery. Weight loss is usually expressed as either the percent of weight loss or the percent of excess weight loss (ie, weight loss above ideal weight). A meta-analysis of mostly short-term weight-loss outcomes (ie, < 5 years) from more than 22,000 procedures found an overall mean excess weight loss of 47.5% for patients who underwent LAGB, 61.6% for RYGB, 68.2% for vertical-banded gastroplasty, and 70.1% for BPD-DS.16 Vertical-banded gastroplasty differs from LAGB in that both a band and staples are used to create a small stomach pouch. Excess weight loss for SG generally averages 50% to 55%, which is intermediate between LAGB and RYGB.17,18
The Swedish Obese Subjects study (N = 4,047), a prospective study of bariatric surgery vs nonsurgical weight management of severely obese patients (BMI > 34), is the largest weight-loss study with the longest follow-up.19 At 20 years, the mean weight loss was 26% for gastric bypass, 18% for vertical-banded gastroplasty, 13% for gastric banding, and 1% for controls. A 10-year study in 1,787 severely obese patients (BMI ≥ 35) who underwent RYGB had 21% more weight loss from their baseline weight than the nonsurgical match.20 At 4-year follow-up in 2,410 patients, there were significant variations in weight loss depending on the procedure: 27.5% for RYGB, 17.8% for SG, and 10.6% in LAGB. Between 2% and 31% regained weight back to baseline: 30.5% for LAGB, 14.6% for SG, and 2.5% for RYGB.20 In contrast, long-term medical (nonsurgical) weight loss rarely exceeds 5%, even with intensive lifestyle intervention.21
Diabetes remission, cardiovascular risk factors, glycemic control
A meta-analysis of 19 mostly observational studies (N = 4,070 patients) reported an overall type 2 DM remission rate of 78% after bariatric surgery with 1 to 3 years of follow-up.22 Resolution or remission was typically defined as becoming “nondiabetic” with normal HbA1c without medications. In the Swedish Obese Subjects study, the remission rate was 72% at 2 years and 36% at 10 years compared with 21% and 13%, respectively, for the nonsurgical controls (P < .001).23 Bariatric surgery was also markedly more effective than nonsurgical treatment in preventing type 2 DM, with a relative risk reduction of 78%.
A systematic review published in 2012 evaluated long-term cardiovascular risk reduction after bariatric surgery in 73 studies and 19,543 patients.24 At a mean follow-up of 57.8 months, the average excess weight loss for all procedures was 54% and rates of remission or improvement were 63% for hypertension, 73% for type 2 DM, and 65% for hyperlipidemia. Results from 12 cohort-matched, nonrandomized studies comparing bariatric surgery vs nonsurgical controls suggest that improvements in surrogate disease markers such as HbA1c, blood pressure, lipids, and body weight after surgery translate to reduced macrovascular and microvascular events and death.25 One of these studies involving male veterans who were mostly at high cardiovascular risk reported a 42% reduction in mortality at 10 years compared with medical therapy.26
In the Swedish Obese Subjects study, the mortality rate from cardiovascular disease in the bariatric surgical group was lower than for control patients (adjusted hazard ratio, 0.47; P = .002) despite a greater prevalence of smoking and higher baseline weights and blood pressures in the surgical cohort.19 For patients with type 2 DM in this study, surgery was associated with a 50% reduction in microvascular complications.27 After 15 years of follow-up, the cumulative incidence of microvascular complications was 41.8 per 1,000 person-years for control patients and 20.6 per 1,000 person-years in the surgery group (hazard ratio, 0.44; P < .001).
These observational, nonrandomized study data suggest that in patients with type 2 DM, bariatric surgery is significantly better than medical management alone in improving glycemic control, reducing cardiovascular risk factors, and lowering long-term morbidity and mortality associated with type 2 DM.
METABOLIC SURGERY: CLINICAL TRIALS
During the past 10 years, 12 randomized controlled trials (RCTs) have compared metabolic surgery vs medical treatment for type 2 DM (Table 1).28–44 All the trials included obese patients with type 2 DM (N = 874; range 38–150 patients per study) with follow-up from 6 months to 5 years. Surgeries were RYGB (9 studies), LAGB (5 studies), SG (2 studies), and BPD-DS (1 study); some studies had multiple surgery types. The severity of type 2 DM varied significantly from mild (mean HbA1c 7.7%, < 2-year onset, no insulin)28 to advanced (mean HbA1c 9.3%, duration 8.3 years, 48% on insulin).29 The BMI ranged from 25 to 53 kg/m2, with 11 of 12 studies including patients with BMI less than 35 kg/m2. Demographics of age, sex, and ethnic background were similar, although 3 studies33–35,44 included a significant number of Asian patients. For most studies, the primary end point was the success rate of reaching remission, defined as an HbA1c target at or below 6.0% to 6.5% without a need for diabetes medications.
Metabolic surgery for type 2 diabetes mellitus: Randomized controlled clinical trials
Collectively, these RCTs showed that surgery was significantly superior to medical treatment in reach ing the designated glycemic target (P < .05 for all). The one exception showed that diabetes remission for LAGB vs medical treatment was 33% and 23%, respectively.41 This result might be due to patients in this study having advanced type 2 DM (HbA1c 8.2% ± 1.2%, with 40% on insulin), and they likely had reduced beta-cell function. Overall, surgery decreased HbA1c by 2% to 3.5%, whereas medical treatment lowered it by only 1% to 1.5%. Most of these studies also showed superiority of surgery over medical treatment in achieving secondary end points such as weight loss, remission of metabolic syndrome, reduction in diabetes and cardiovascular medications, and improvement in triglycerides, lipids, and quality of life. Results were mixed in terms of improvements in systolic and diastolic blood pressure or low-density lipoproteins after surgery vs medical treatment, but many studies did show a corresponding reduction in medication usage.
Durability of the effects of surgery was demonstrated in a 5-year study that showed superior and durable weight loss and glycemic control (remission) with both RYGB and BPD in severely obese patients (BMI ≥ 35) vs medical therapy.32 Similarly, Schauer et al43 showed that RYGB and SG were more effective than intensive medical therapy in improving or, in some cases, resolving hyperglycemia for 5 years. In the RCTs, patients who preoperatively had shorter duration of diabetes, lower HbA1c levels, no insulin requirement, and more postoperative weight loss were more likely to achieve diabetes remission.
Although previous guidelines and payer coverage policies had limited metabolic surgery to severely obese patients (BMI ≥ 35 kg/m2), nearly all RCTs showed that the surgical procedures, especially RYGB and SG, were equally effective in patients with BMI 30 to 35 kg/m2. This is particularly important given that most patients with type 2 DM have a BMI less than 35 kg/m2. The effect of surgery in these patients with mild obesity is also durable out to at least 5 years.43
No RCT was sufficiently powered to detect differences in macrovascular or microvascular complications or death, especially at the relatively short follow-up, and no such differences have been detected thus far. The STAMPEDE (Surgical Therapy and Medications Potentially Eradicate Diabetes Efficiently) trial43 showed that bariatric surgery (RYGB or SG) did not appear to worsen or improve retinopathy outcomes at 5 years compared with intensive medical management.
METABOLIC SURGERY: ADVERSE EVENTS
Surgical complications
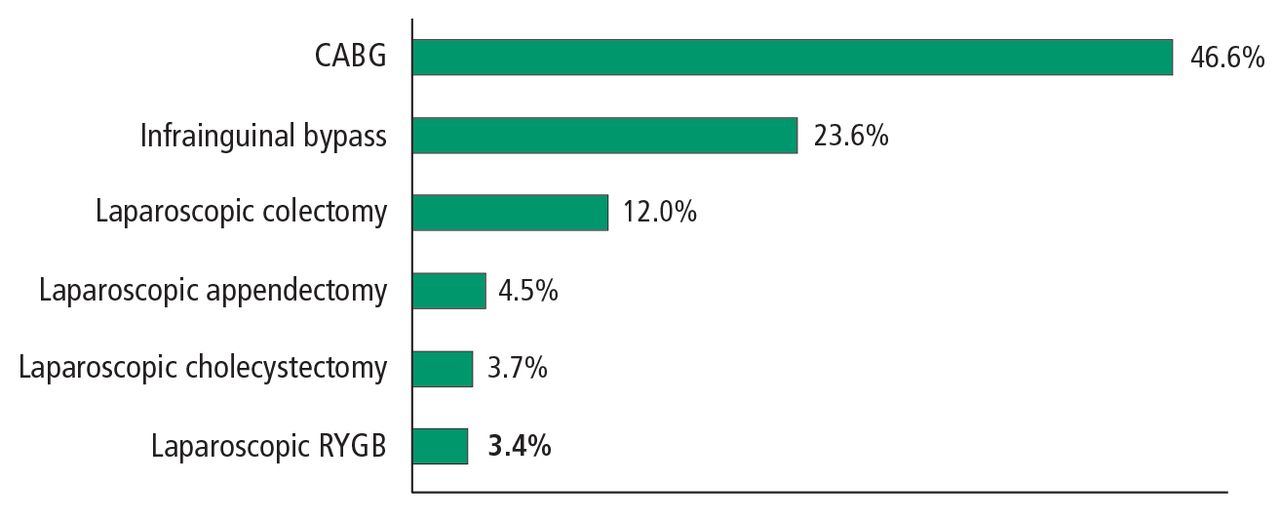
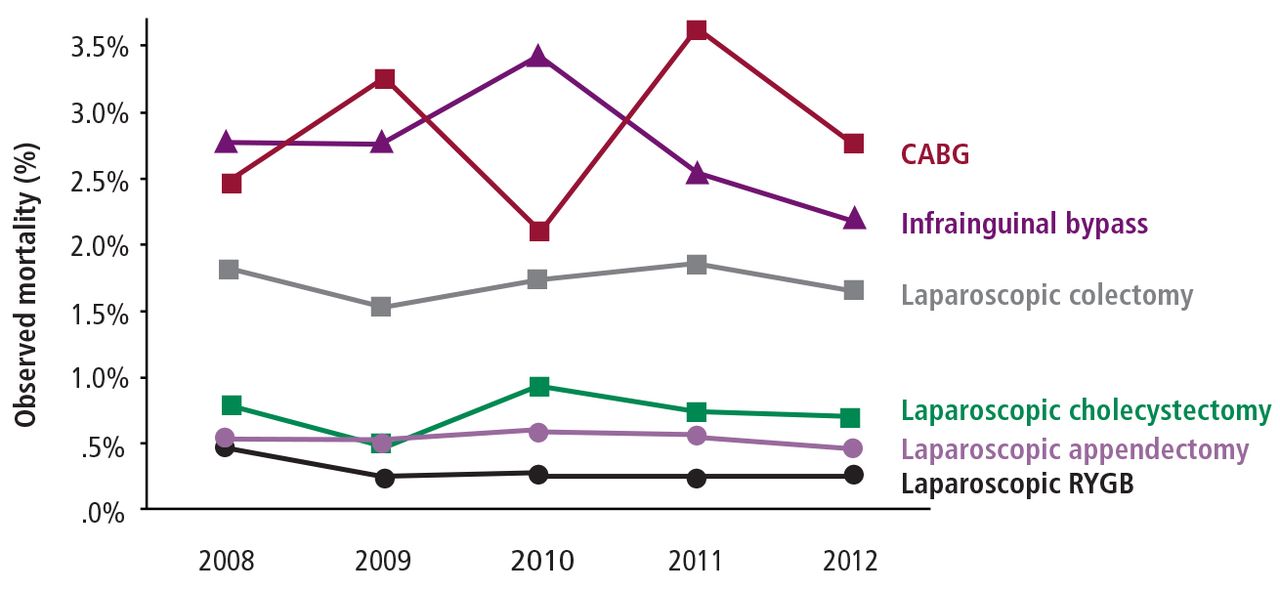
Overall, rates of perioperative morbidity and mortality of bariatric surgery are similar to those of common, relatively low-risk abdominal procedures such as cholecystectomy and appendectomy. The NIH-supported Longitudinal Assessment of Bariatric Surgery study reported a low 30-day mortality rate of 0.3% in 4,776 patients and a 4.3% incidence of major adverse events in the early postoperative period.45 A study from the American College of Surgeons (> 65,000 patients) showed that laparoscopic RYGB had perioperative morbidity and mortality rates of 3.4% and 0.3%, respectively, similar to those for laparoscopic cholecystectomy (3.7% and 0.7%) and appendectomy (4.5% and 0.5%) (Figures 3 and 4) and much lower than for laparoscopic colectomy (12.0% and 1.7%).46
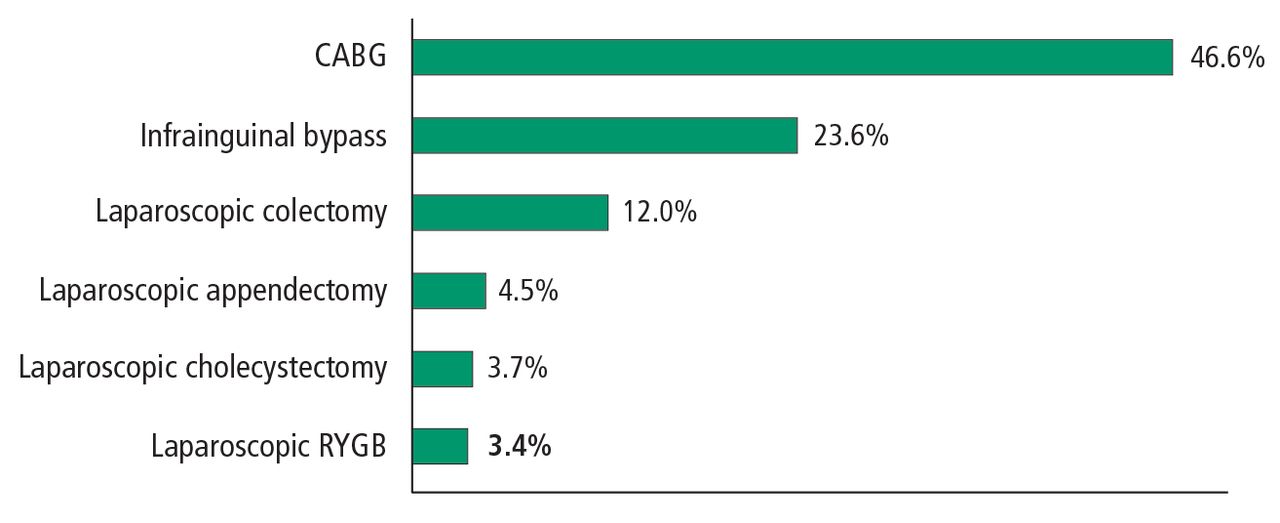
Postoperative complication rates of surgical procedures in patients with type 2 diabetes mellitus: US data.
CABG = coronary artery bypass graft; RYGB = Roux-en-Y gastric bypass
Reprinted with permission from John Wiley & Sons (Aminian A, et al. How safe is metabolic/diabetes surgery? Diabetes Obes Metab 2015; 17:198–201.) ©2014 John Wiley & Sons Ltd.

Mortality rates of 8 procedures in patients with diabetes (2008–2012).
CABG = coronary artery bypass grafting; RYGB = Roux-en-Y gastric bypass
Reprinted with permission from John Wiley & Sons (Aminian A, et al. How safe is metabolic/diabetes surgery? Diabetes Obes Metab 2015; 17:198–201.) ©2014 John Wiley & Sons Ltd.
Table 2 summarizes early and late postoperative complications of metabolic surgery. Although rare (< 1%), cardiopulmonary complications such as myocardial infarction and pulmonary embolism are the major causes of mortality, representing 70% of all perioperative deaths.45 Intestinal leakage at the anastomosis or staple line is the most serious early surgical complication after RYGB (0.1%–5.6%) and may potentially lead to peritonitis. Bowel obstruction (0.5%–2%) and marginal ulcers (1%–5%) may also occur months to years after RYGB.47,48 Staple-line leakage (1%–5%) and gastric stenosis (1%–5%) are the most common surgical complications of SG.17
Complications after metabolic surgery
For BPD-DS, perioperative complications are similar to those for RYGB. Although LAGB is safe, with a very low mortality rate (< 0.3%), late complications such as band slippage, erosion, migration, and surgical port infection occur in about 20% of patients.49 Reoperation for poor weight loss or complications after LAGB is common, occurring in approximately 50% of patients.50 In general, patients at higher risk of complications after bariatric surgery are those with high BMI, older age, multiple comorbidities, smoking, or previous revisional operations; men are also at higher risk.45
Nutritional deficiencies
Postoperative nutritional deficiencies are typically associated with diminished nutrient intake or the malabsorptive effect of bariatric procedures. They are more common after RYGB and BPD-DS and less common after SG and LAGB. In addition, there is a high prevalence of nutritional deficiencies (35%–80%) in patients seeking bariatric surgery; thus, poor preoperative nutrition may be a factor in the development of postoperative deficiencies. Common preoperative nutrient deficiencies are vitamin A (11%), vitamin B12 (13%), vitamin D (40%), zinc (30%), iron (16%), ferritin (9%), selenium (58%), and folate (6%).51 Recommendations are to assess for these deficiencies and correct any identified before surgery.
Mild anemia after bariatric procedures is common, occurring in 15% to 20% of cases, and it is believed to result from reduced absorption of iron and B12, as well from pre-existing iron deficiency anemia in premenopausal patients.52 Deficiencies in trace minerals (selenium, zinc, and copper) and vitamins (B12, B1, A, E, D, and K) can occur after bariatric procedures, especially after BPD-DS.53 Nutrient deficiencies can be prevented or corrected with appropriate vitamin, iron, and calcium supplementation.54
Bone mineral density may decrease after bariatric surgery (14% in the proximal femur).55 Reduced mechanical loading after weight loss, reduced consumption and malabsorption of micronutrients (calcium, vitamin D), and neurohormonal alterations are potential underlying mechanisms of bone mineral density reduction after bariatric surgery. Rates of bone fracture and osteoporosis are not well delineated, raising questions about whether bone loss after bariatric surgery is clinically relevant or a functional adaptation to skeletal unloading. However, the extreme malabsorptive procedures of BPD-DS have been associated with severe calcium and vitamin D deficiencies, leading to decreased bone mineral density and osteoporosis.
Protein malnutrition also can occur after these extreme malabsorptive procedures. Patients require postoperative oral protein supplementation (80–100 g/day) and lifelong monitoring for nutritional complications after these procedures.56
Additional complications
Other late complications of bariatric surgery that are less clear in incidence and cause include kidney stones, alcohol abuse, depression, and suicide. One study of patients after RYGB (N = 4,690) reported a significantly higher prevalence of kidney stones than in obese controls: 7.5% vs 4.6%, respectively.57 Proposed causes of kidney stone formation following bariatric surgery include hyperoxaluria, hypocitraturia, and elevated urine acidity.58
The prevalence of alcohol-use disorder after bariatric surgery ranges from 7.6% to 11.8% and appears to be higher in patients with a history of alcohol use.59 Paradoxically, while bariatric surgery has been shown to significantly decrease depression,60 some studies suggest that a slight increase in the risk of suicide may occur,61 while others do not.62 A recent review concluded that accurate rates of suicide after bariatric surgery are not known, but practitioners should be aware of this concern and appropriately screen and counsel their patients.63
Although the 12 RCTs reported in Table 1 were not powered to detect differences in treatment-related complications, the overall rates of complications were consistent with those in observational studies.9 The most common surgical complications were anemia (15%), need for reoperation (8%), and GI (5%–10%). The 30-day surgical mortality rate was 0.2% (1 death) among the 465 surgical patients. Complications were not limited to the surgical patients. In the medical-treatment control group of the STAMPEDE trial,30 anemia (16%) and weight gain (16%) were common. Investigators reported challenges with medication compliance, including adverse effects leading to discontinuation of medications. Mild hypoglycemia was common, with no significant differences between the surgical and medical treatment groups.
METABOLIC SURGERY: COST EFFECTIVENESS
The cost of bariatric procedures varies considerably but, in general, ranges from $20,000 to $30,000, similar to the cost of cholecystectomy, hysterectomy, and colectomy. Retrospective analyses and modeling studies indicate that metabolic surgery is cost-effective and may present a cost savings in patients with type 2 DM, with a break-even time between 5 and 10 years.64,65 The cost savings, largely based on assumptions of long-term effectiveness and safety, result from reductions in medication use, outpatient care costs, and long-term complications of type 2 DM.
WHO SHOULD HAVE METABOLIC SURGERY?
Until recently, there was no clear national or international consensus on the role of metabolic surgery in treating type 2 DM. In 2015, the 2nd Diabetes Surgery Summit (DSS-II) Consensus Conference published guidelines that were endorsed by more than 50 diabetes and medical organizations.5 The recommendations cover many clinically relevant issues, including patient selection, preoperative evaluation, choice of procedure, and postoperative follow-up. The consensus conference delegates concluded that there is sufficient evidence demonstrating that metabolic surgery achieves excellent glycemic control and reduces cardiovascular risk factors.
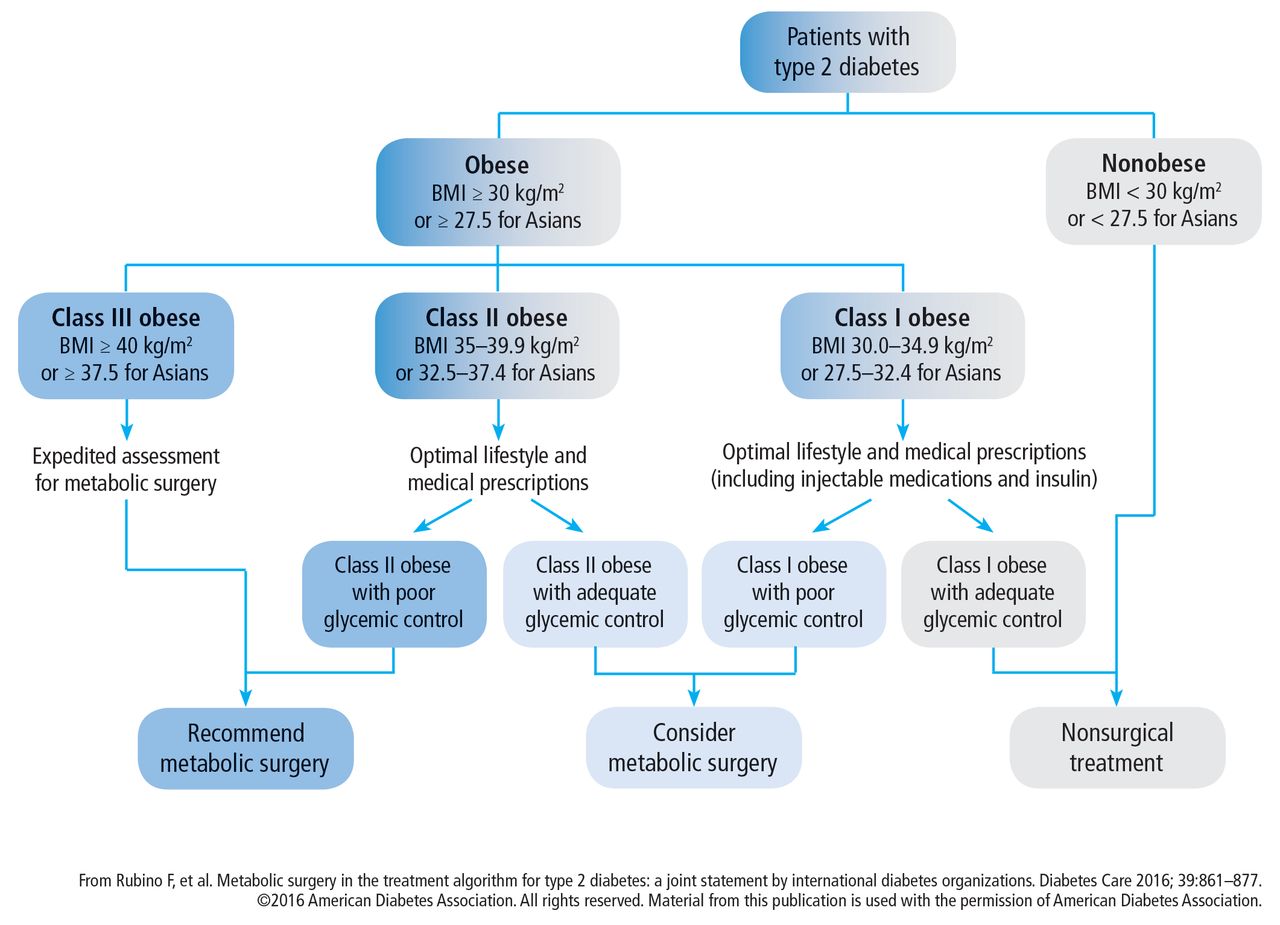
According to the DSS-II guidelines, metabolic surgery should be recommended to treat type 2 DM in patients with class III obesity (BMI ≥ 40 kg/m2) regardless of glycemic control and in those with class II obesity (BMI 35.0–39.9 kg/m2) when hyperglycemia is inadequately controlled by lifestyle and optimal medical therapy. Surgery should also be considered for patients with type 2 DM and BMI 30.0 to 34.9 kg/m2 if hyperglycemia is inadequately controlled despite optimal treatment with either oral or injectable medications. These BMI thresholds should be reduced by 2.5 kg/m2 for Asian patients.
The treatment algorithm from DSS-II incorporates appropriate use of all 3 treatment modalities: lifestyle intervention, drug therapy, and surgery (Figure 5).5 The 2017 Standards of Care for Diabetes from the American Diabetes Association include those key indications in the recommendations for metabolic surgery (Table 3).2

Algorithm for the treatment of type 2 diabetes, as recommended by the 2nd Diabetes Surgery Summit’s voting delegates.
American Diabetes Association’s recommendations for the treatment of type 2 diabetes mellitus
SUMMARY
Recent evidence from multiple RCTs has provided level 1a evidence supporting metabolic surgery as an effective treatment for type 2 DM. These studies have shown the superiority of surgery vs medical therapy in achieving excellent and durable glycemic control as well as benefits in long-term weight loss, medication reduction, dyslipidemia, overall quality of life, and other cardiovascular risk factor reductions. Metabolic surgery is the only diabetes treatment proven to result in long-term remission in 23% to 60% of patients.
The safety of metabolic surgery has significantly improved with the advent of laparoscopic surgery and recent national quality improvement initiatives that have made gastric bypass and SG as safe as cholecystectomy and appendectomy. Although observational studies suggest that metabolic surgery is associated with a reduction in cardiovascular and diabetes complications and mortality, these observations have not been confirmed in long-term RCTs.
Based on the published evidence, metabolic surgery is now endorsed as a standard treatment option, which provides patients and practitioners with a powerful tool to help combat the life-impairing effects of type 2 DM.
Footnotes
Dr. Schauer reported research grant support from Ethicon, Medtronic, and Pacira Pharmaceuticals; consulting fees from The Medicines Company, AMAG Pharmaceuticals, GI Dynamics, and Neurotronics; honoraria for speaking from Novo Nordisk; and ownership interest in SE HQC LLC. Dr. Nor Hanipah reported no financial interests or relationships that pose a potential conflict of interest with this article. Dr. Rubino reported research grant support from NIMR (UK Gov) and Ethicon; consulting fees from Fractyl and GI Dynamics; and honoraria for speaking from Medtronic and Ethicon.
- Copyright © 2017 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.