


Article Figures & Data
Figures
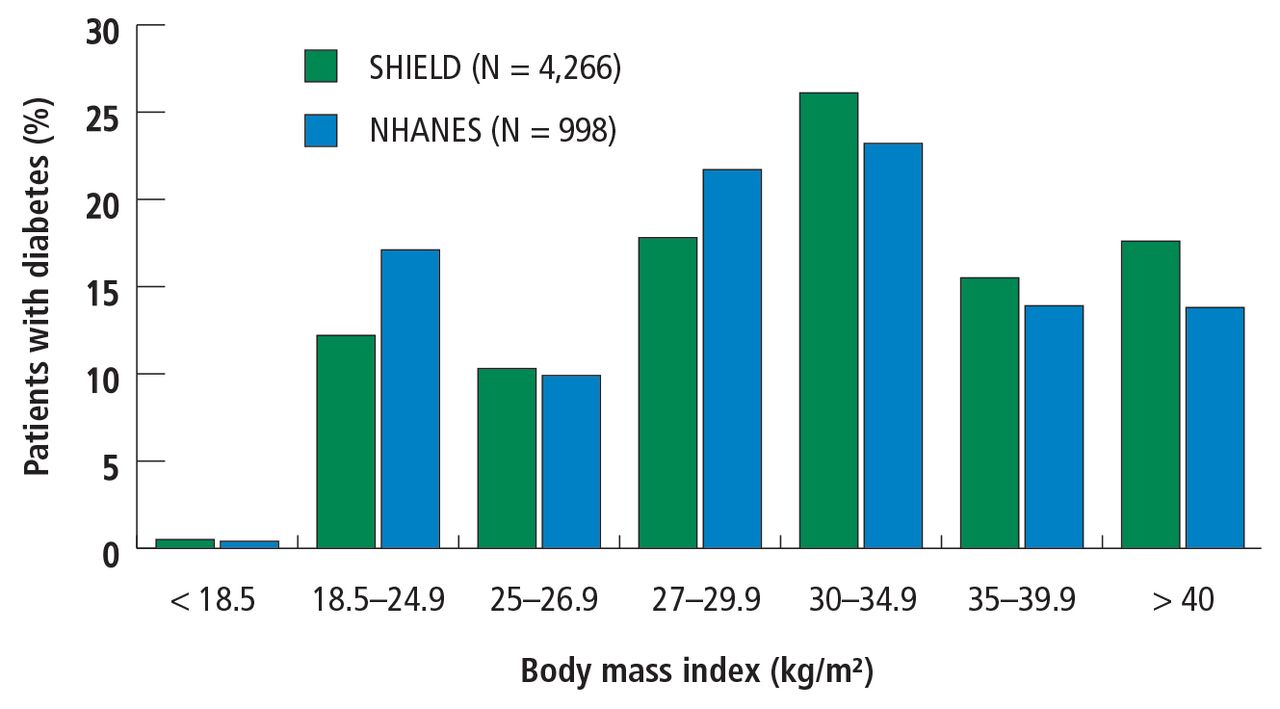
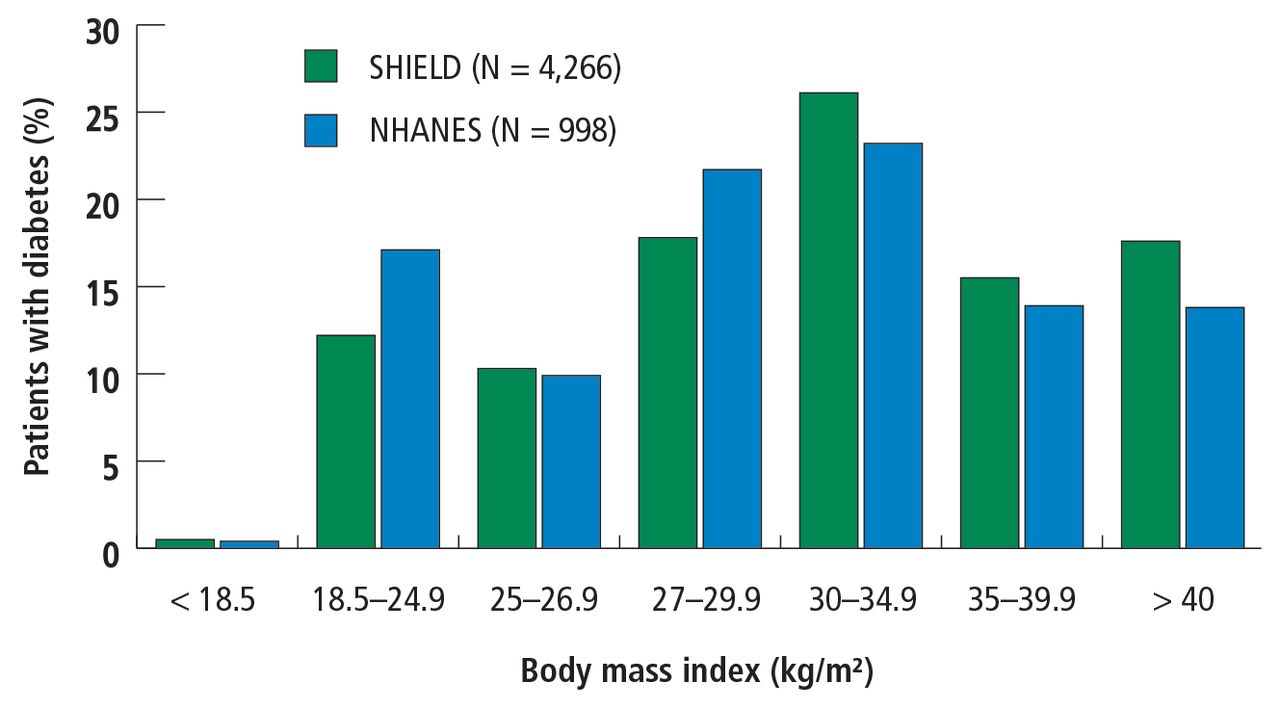
- FIGURE 1
Relative distribution of body mass index of patients with diabetes.
SHIELD = Study to Help Improve Early Evaluation and Management of Risk Factors Leading to Diabetes (2004); 4,266 of 127,420 survey respondents with diabetes (type 1 = 368; type 2 = 3,898).
NHANES = National Health and Nutrition Examination Survey (1999–2002); 998 of 11,441 survey repondents with diabetes (type 1 and 2).
Data from Bays et al.1
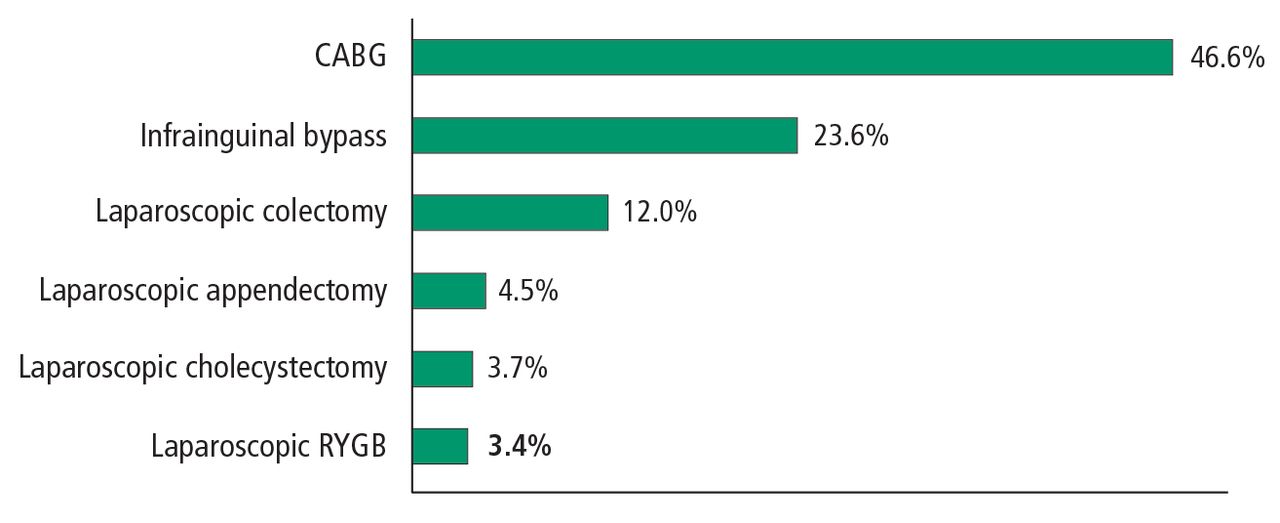
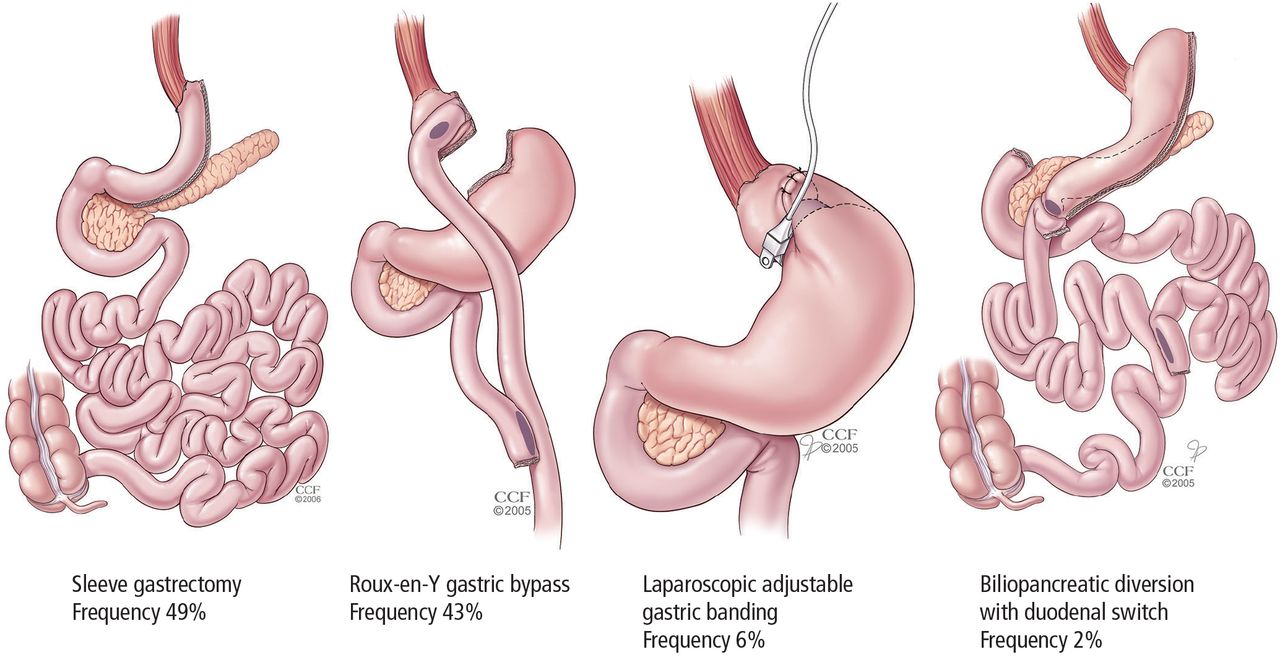
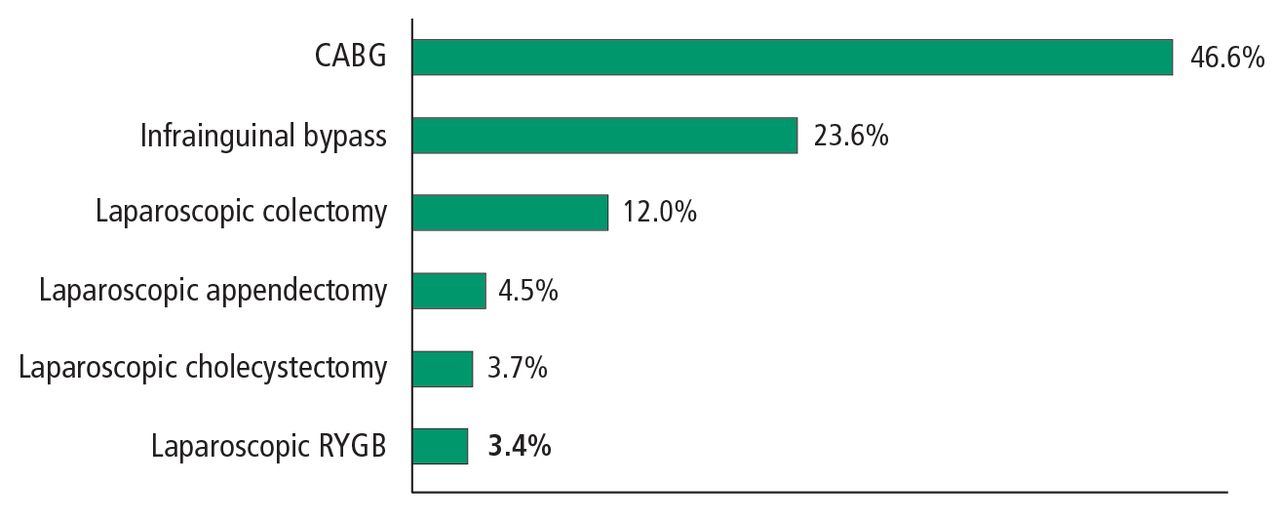
- FIGURE 2
Most common metabolic surgical procedures.
- FIGURE 3
Postoperative complication rates of surgical procedures in patients with type 2 diabetes mellitus: US data.
CABG = coronary artery bypass graft; RYGB = Roux-en-Y gastric bypass
Reprinted with permission from John Wiley & Sons (Aminian A, et al. How safe is metabolic/diabetes surgery? Diabetes Obes Metab 2015; 17:198–201.) ©2014 John Wiley & Sons Ltd.
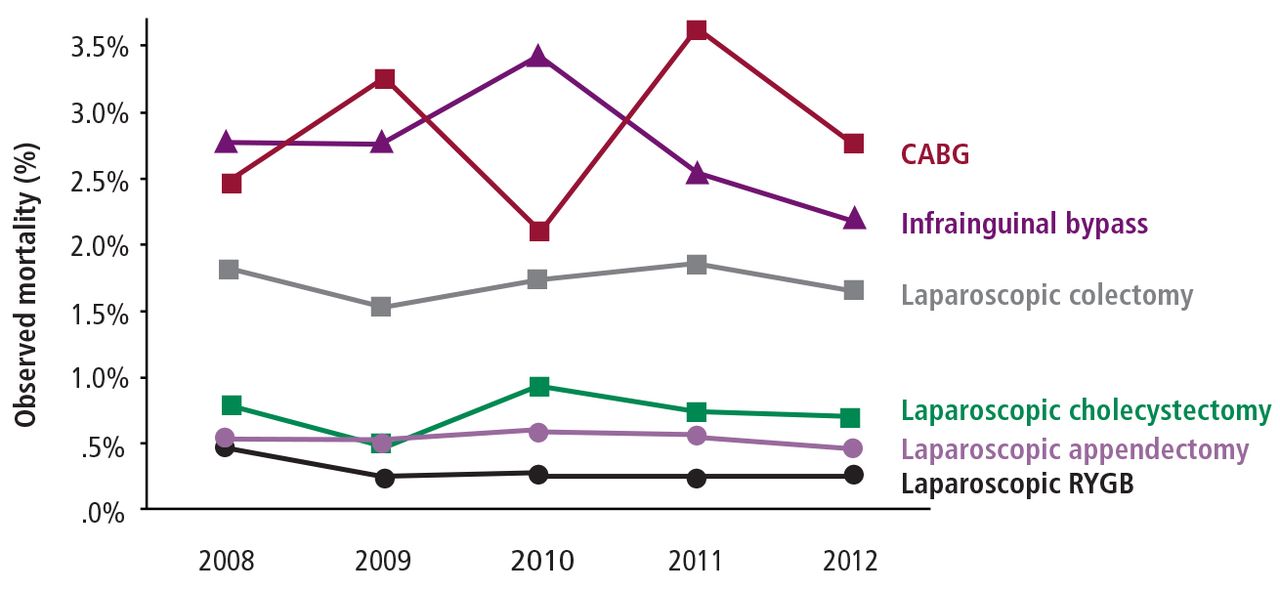
- FIGURE 4
Mortality rates of 8 procedures in patients with diabetes (2008–2012).
CABG = coronary artery bypass grafting; RYGB = Roux-en-Y gastric bypass
Reprinted with permission from John Wiley & Sons (Aminian A, et al. How safe is metabolic/diabetes surgery? Diabetes Obes Metab 2015; 17:198–201.) ©2014 John Wiley & Sons Ltd.
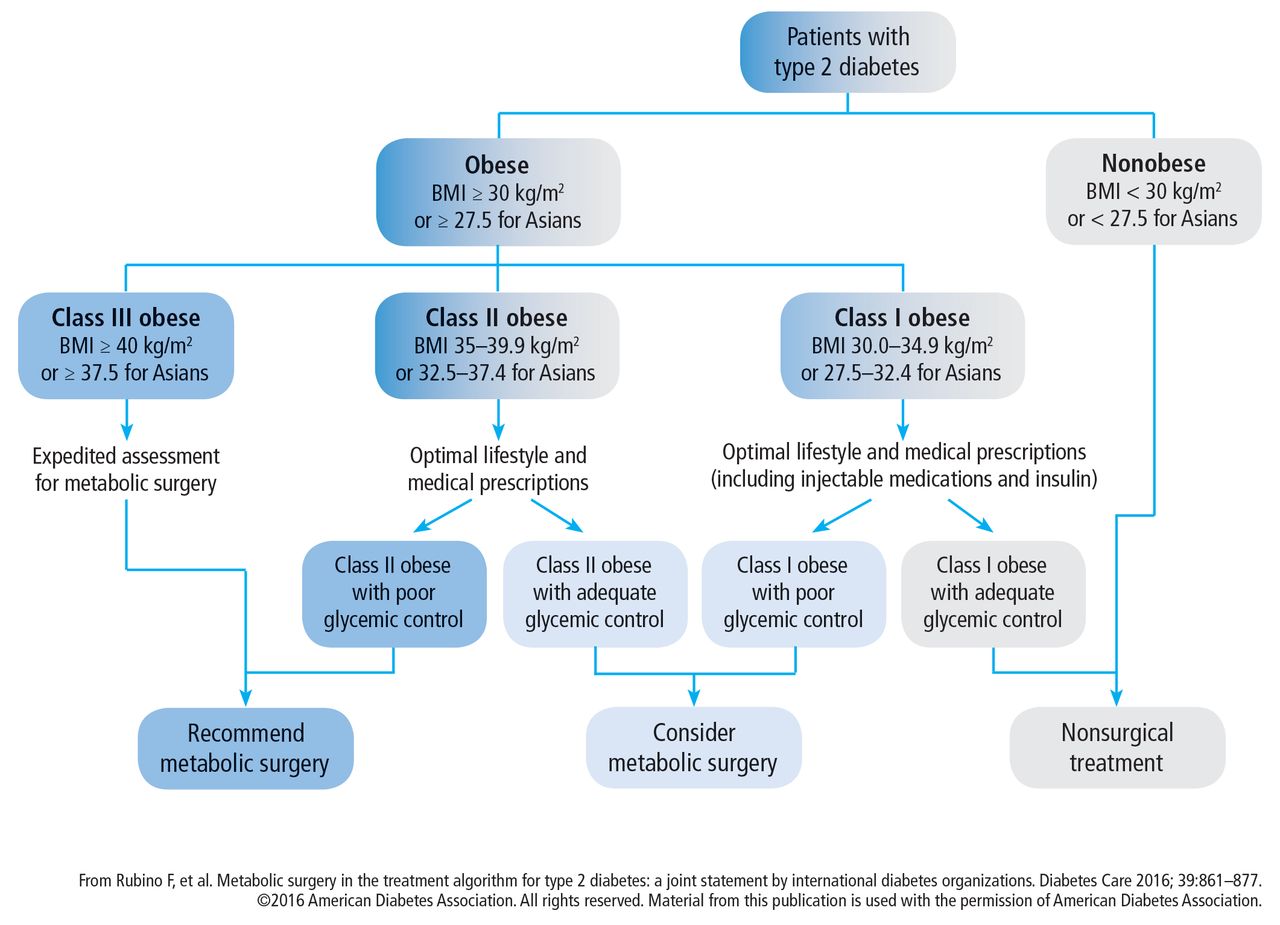
- FIGURE 5
Algorithm for the treatment of type 2 diabetes, as recommended by the 2nd Diabetes Surgery Summit’s voting delegates.



Tables
- TABLE 1
Metabolic surgery for type 2 diabetes mellitus: Randomized controlled clinical trials
Study Pts with BMI < 35 kg/m2 Study design No. pts Follow-up (mo) Remission criteria Remissiona or change in HbA1c (%) P value Dixon28 22% LAGB vs control 60 24 HbA1c < 6.2% 73 vs 13 < .001 Schauer29,30,43 36% RYGB vs SG vs control 150 60 HbA1c ≤ 6.0% 22 vs 15 vs 0 < .05 Mingrone31,32 0% RYGB vs BPD vs control 60 60 HbA1c ≤ 6.5% 42 vs 68 vs 0 .003 Ikramuddin33,34 59% RYGB vs control 120 24 HbA1c < 6.0% 44 vs 9 < .001 Liang35 100% RYGB vs control 101 12 HbA1c < 6.5% 90 vs 0 vs 0b < .0001 Halperin36 34% RYGB vs control 38 12 HbA1c < 6.5% 58 vs 16 .03 Courcoulas37,38 43% RYGB vs LAGB vs control 69 36 HbA1c < 6.5% 40 vs 29 vs 0 .004 Wentworth39 100% LAGB vs control 51 24 FBG < 7.0 mmol/L 52 vs 8 .001 Parikh40 100% RYGB/LAGB/SG vs control 57 6 HbA1c < 6.5% 65 vs 0 .0001 Ding41 34% LAGB vs control 45 12 HbA1c < 6.5% 33 vs 23c .46 Cummings42 25% RYGB vs control 43 12 HbA1c < 6.0% 60 vs 5.9 .002 Shah44 85 RYGB vs control 80 24 HbA1c < 6.5% 60 vs 2.5 < .001 Remission criteria:
↵a Remission was primary or secondary end point; HbA1c value without diabetes medications, unless otherwise specific.
↵b Remission was not precisely defined; HbA1c < 6.5% by extrapolation.
↵c Intermittent diabetes medications.
BMI = body mass index; BPD = biliopancreatic diversion; FBG = fasting blood glucose; HbA1c = glycated hemoglobin; LAGB = laparoscopic adjustable gastric band; RYGB = Roux-en-Y gastric bypass; SG = sleeve gastrectomy
Modified from Schauer PR, et al. Clinical outcomes of metabolic surgery: efficacy of glycemic control, weight loss, and remission of diabetes. Diabetes Care 2016; 39:908–911. ©2016 American Diabetes Association. All rights reserved. Material from this publication is used with the permission of American Diabetes Association.
Complications Frequency (%) Sepsis from anastomotic leak 0.1–5.6 Hemorrhage 1–4 Cardiopulmonary events < 1 Thromboembolic disease 0.34 Death 0.1–0.3 Late complications for LAGB Band slippage 15 Leakage 2–5 Erosion 1–2 Late complications of bypass procedures Anastomotic stricture 1–5 Marginal ulcer 1–5 Bowel obstruction 0.5–2 Micronutrient and macronutrient deficiencies from RYGB 2–3 years postoperatively Iron deficiency 45–52 Vitamin B12 deficiency 8–37 Calcium deficiency 10 Vitamin D deficiency 51 Fat-soluable vitamin deficiencies (A, D, E, and K) and protein calorie malnutrition from BPD-DS procedures 1–5 BPD-DS = biliopancreatic diversion with duodenal switch; LAGB = laparoscopic adjustable gastric banding
From Schauer PR, et al. Clinical outcomes of metabolic surgery: efficacy of glycemic control, weight loss, and remission of diabetes. Diabetes Care 2016; 39:908–911. ©2016 American Diabetes Association. All rights reserved. Material from this publication is used with the permission of American Diabetes Association.
- TABLE 3
American Diabetes Association’s recommendations for the treatment of type 2 diabetes mellitus
Treatment Body mass index category (kg/m2) 23.0a or
25.0–26.927.0–29.9 27.5a
or 30.0–34.935.0–39.9 ≥ 40 Diet, physical activity, and behavioral therapy † † † † † Pharmacotherapy † † † † Metabolic surgery † † † ↵a Cutoff points for Asian American individuals.
↵† Treatment may be indicated for selected motivated patients.
From American Diabetes Association. Obesity management for the treatment of type 2 diabetes. Sec. 7. In: Standards of Medical Care in Diabetes—2017. Diabetes Care 2017; 40(suppl 1):S57–S63. ©2017 American Diabetes Association. All rights reserved. Material from this publication is used with the permission of American Diabetes Association.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.