


Article Figures & Data
Figures
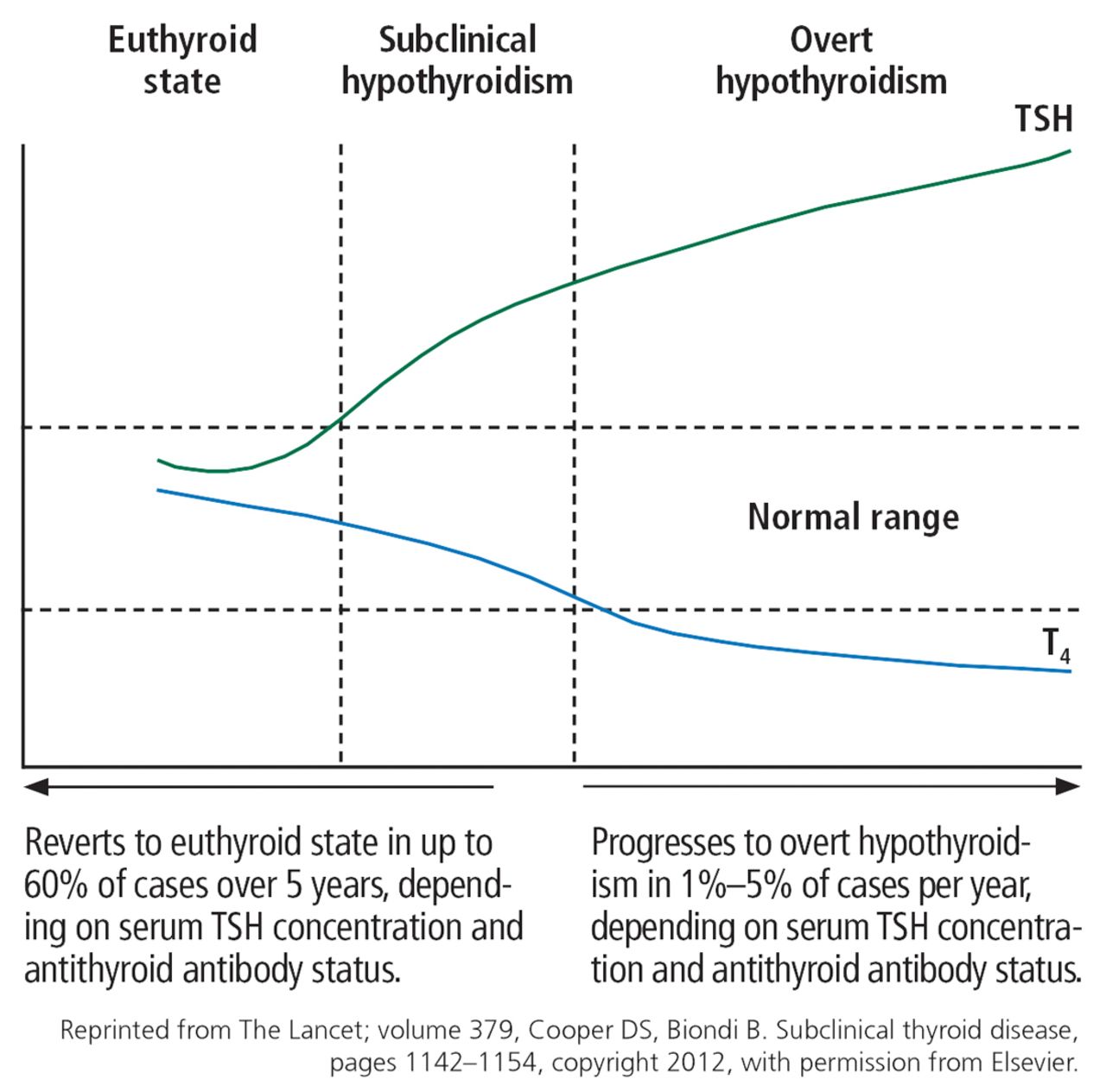
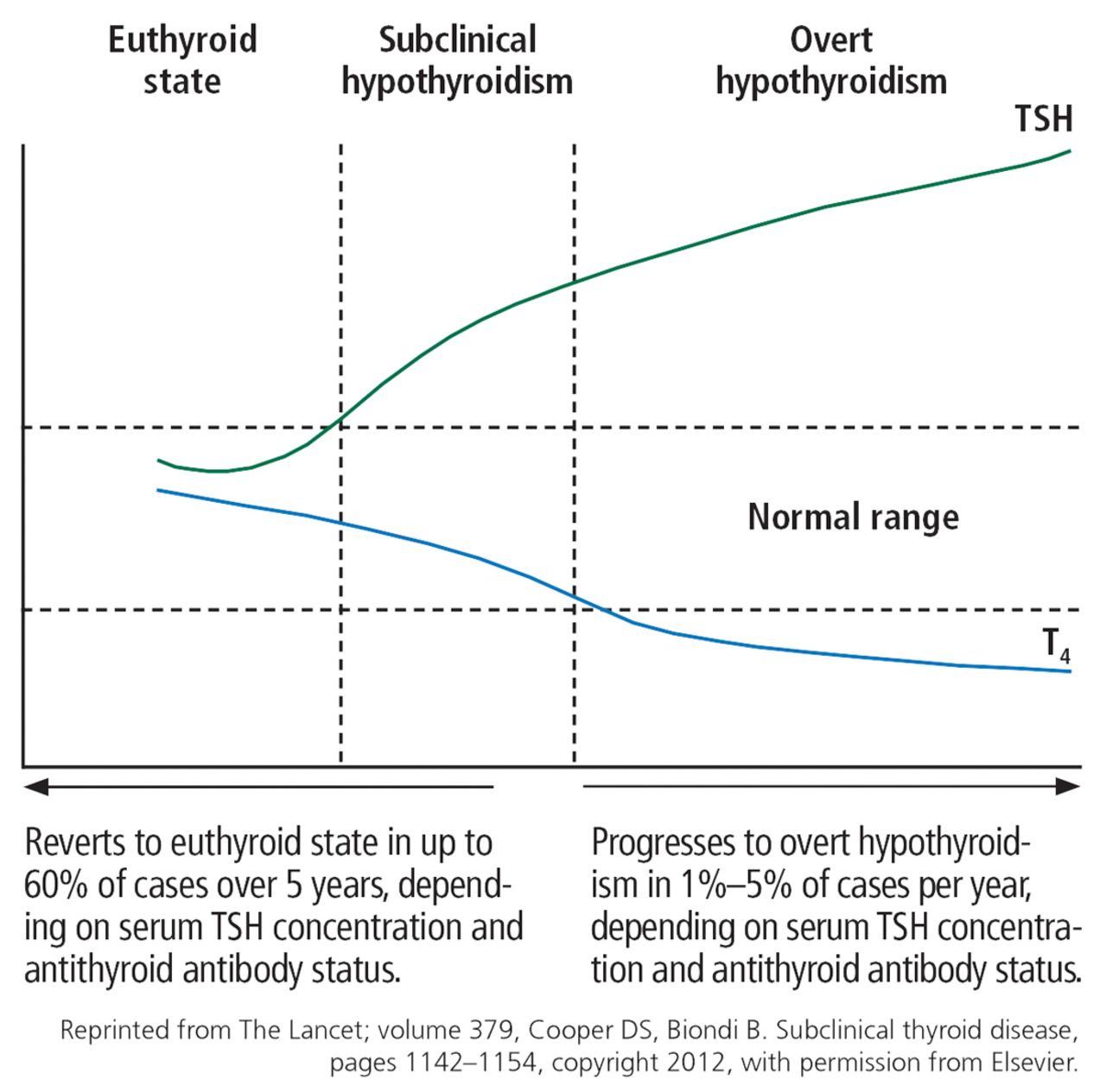
- Figure 1
Natural course of subclinical hypothyroidism (TSH = thyroid-stimulating hormone, T4 = free thyroxine).
- Figure 2
Treatment algorithm for subclinical hypothyroidism in nonpregnant patients.

Tables
Subclinical hypothyroidism
Autoimmune (Hashimoto) thyroiditis
Suboptimal treatment of overt hypothyroidism
Partial thyroidectomy
Radioactive iodine ablation
External beam radiation of head and neck
Infiltrative diseases of the thyroid (amyloidosis, sarcoidosis, hemochromatosis, Riedel thyroiditis, scleroderma)
Drugs, eg, iodine contrast, amiodarone, lithium, tyrosine kinase inhibitors (sunitinib, sorafenib), interferon alpha, or immune response modulators (ipilimumab, alemtuzumab, pembrolizumab)
Iodine deficiency
Excess iodine
Thyroid dysgenesisPhysiologic increases
Diurnal variation
Recovery phase of euthyroid sick syndrome
Recovery phase of subacute, painless, or postpartum thyroiditisOther causes
Assay variability
Substances that interfere with TSH assays (heterophile antibodies, rheumatoid factor, biotin, macro-TSH or abnormal TSH isoforms)
Central hypothyroidism or hyperthyroidism
Thyroid hormone resistance
Impaired renal function
Adrenal insufficiency
Obesity
Older ageBased on information in references 1, 2, and 16.
Adverse effect Evidence of adverse effect Role for treatment with levothyroxine Metabolic syndrome, obesity, diabetes Associations observed, but cause and effect are unclear23,24 No evidence to support Dyslipidemia Relationships observed between thyroid-stimulating hormone (TSH) elevation and altered lipid profiles13,43 Associated with improved lipid profiles2,34,44–46 Cardiovascular endothelial dysfunction Increased risk of myocardial infarction, atherosclerosis, aortic calcification,48 cardiovascular disease and mortality37; increased arterial stiffness and systemic vascular resistance45,53 Lessens cardiovascular risk and mortality in patients < 65 years Stroke Conflicting data: no association in patients ≥ 65 years, but some association in those < 65 Lessens cardiovascular risk and mortality in patients < 65 years Psychiatric and cognitive dysfunction Associated with worsened preexisting depression and bipolar disease; may affect cognition65 May improve mood, anxiety, cognition in older patients35 Neuromuscular dysfunction, exercise intolerance Associated with skeletal muscle dysfunction, exercise intolerance71 Limited data on treatment; role is unclear75 Bone health Associated with increased risk of hip fracture attributed to suppression of bone turnover by elevated TSH18,76,77 Too few clinical studies to define a role Thyroid cancer Some data suggest elevated TSH is associated with higher risk79–82 More studies needed to understand association Infertility, recurrent miscarriage Inconclusive evidence links subclinical hypothyroidism with infertility86; infertility rate is higher in women who also have positive thyroid peroxidase antibody than in women without autoimmunity87 Some studies have shown lower rates of miscarriage with levothyroxine when TSH > 4.0 mlU/L86,91–92; insufficient data to support its use in patients with subclinical hypothyroidism and infertility; however, consider in euthyroid patients with positive peroxidase antibody and recurrent miscarriage90 Pregnancy complications Associated with several pregnancy-related complications including preeclampsia, hypertension, placental abruption, and postpartum hemorrhage in some studies,26,96 but not in others; if present, screen for autoimmunity No recommendations; insufficient evidence to evaluate role of treatment Preterm delivery, pregnancy loss Associated with high risk of miscarriage, preterm delivery, pregnancy loss at even mildly elevated TSH levels (2.5-5 mIU/L)99;104–107; risk is as high as 60% with TSH levels > 6 mIU/L and higher with positive thyroid peroxidase antibody108–110 Improves maternal and fetal outcomes, including risk of low birth weight and low Apgar score, in women with subclinical hypothyroidism and TSH 2.5-10 mIU/L93,106; evidence less clear with TSH 2.5-4 mIU/L86; not recommended for the subgroup of pregnant patients with negative thyroid peroxidase antibody and TSH within pregnancy-specific range or < 4 mIU/L Thyroid-stimulating hormone (TSH) level > 2 times the upper limit of normal or > 8 mIU/L
Progressive rise in TSH
Goiter
Positive antithyroid antibodies
Pregnancy or planning pregnancy
Infertility or ovulatory dysfunction
Childhood or adolescence
Dyslipidemia
Established cardiovascular disease or risk factors for cardiovascular disease
Depression or bipolar disease
Therapeutic trial for clinical symptoms of hypothyroidism
Patient preference




{kind=link}
{kind=link}
Jump to section
- Article
- ABSTRACT
- HIGH TSH, NORMAL FREE T4 LEVELS
- WHAT IS THE UPPER LIMIT OF NORMAL FOR TSH?
- SUBCLINICAL HYPOTHYROIDISM IS COMMON
- A VARIETY OF CAUSES
- SUBCLINICAL HYPOTHYROIDISM CAN RESOLVE OR PROGRESS
- GUIDELINES FOR SCREENING DIFFER
- CLINICAL PRESENTATION
- ADVERSE EFFECTS OF SUBCLINICAL HYPOTHYROIDISM, EFFECTS OF THERAPY
- INDIVIDUALIZED MANAGEMENT AND SHARED DECISION-MAKING
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.