


Article Figures & Data
Figures
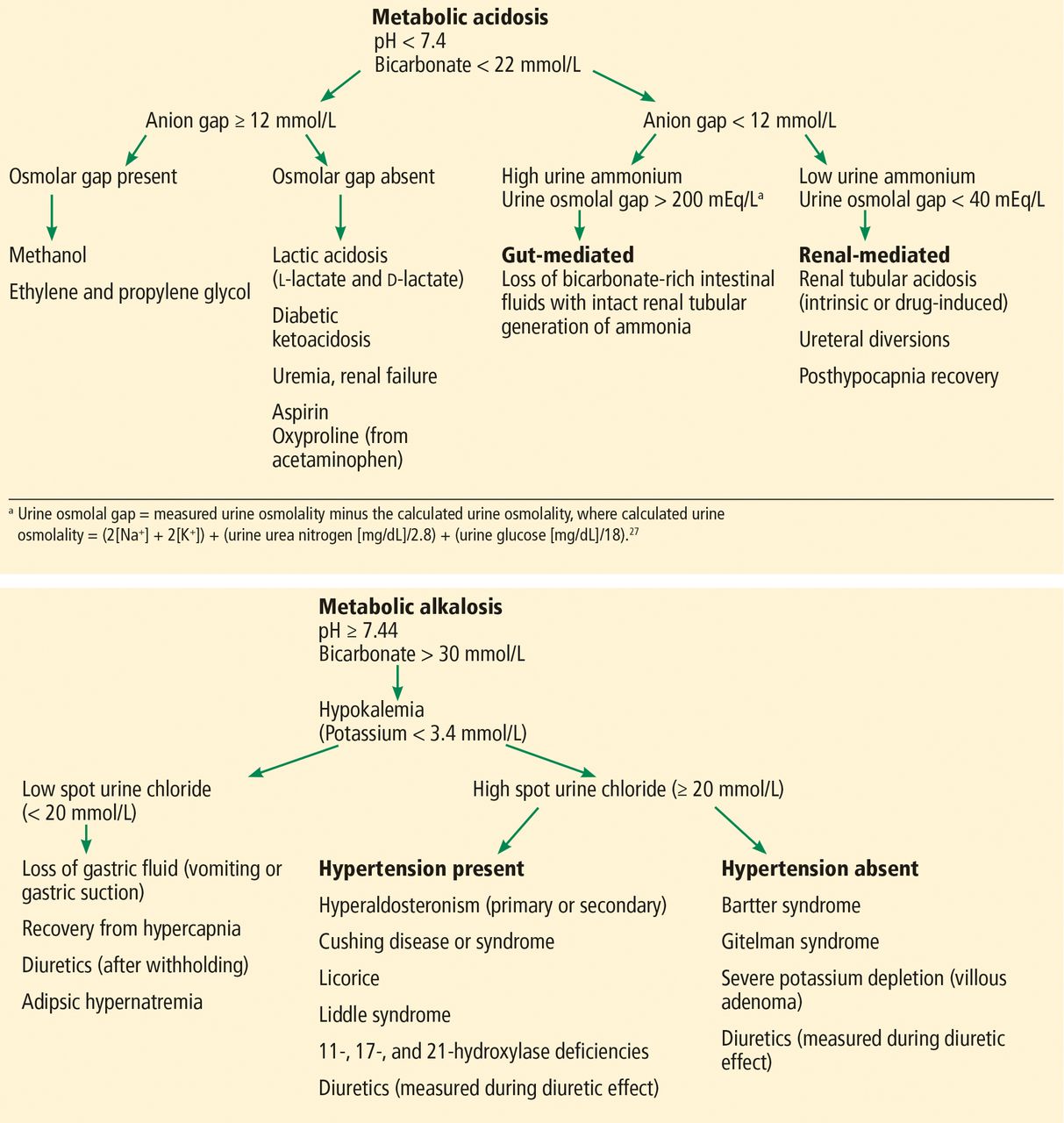
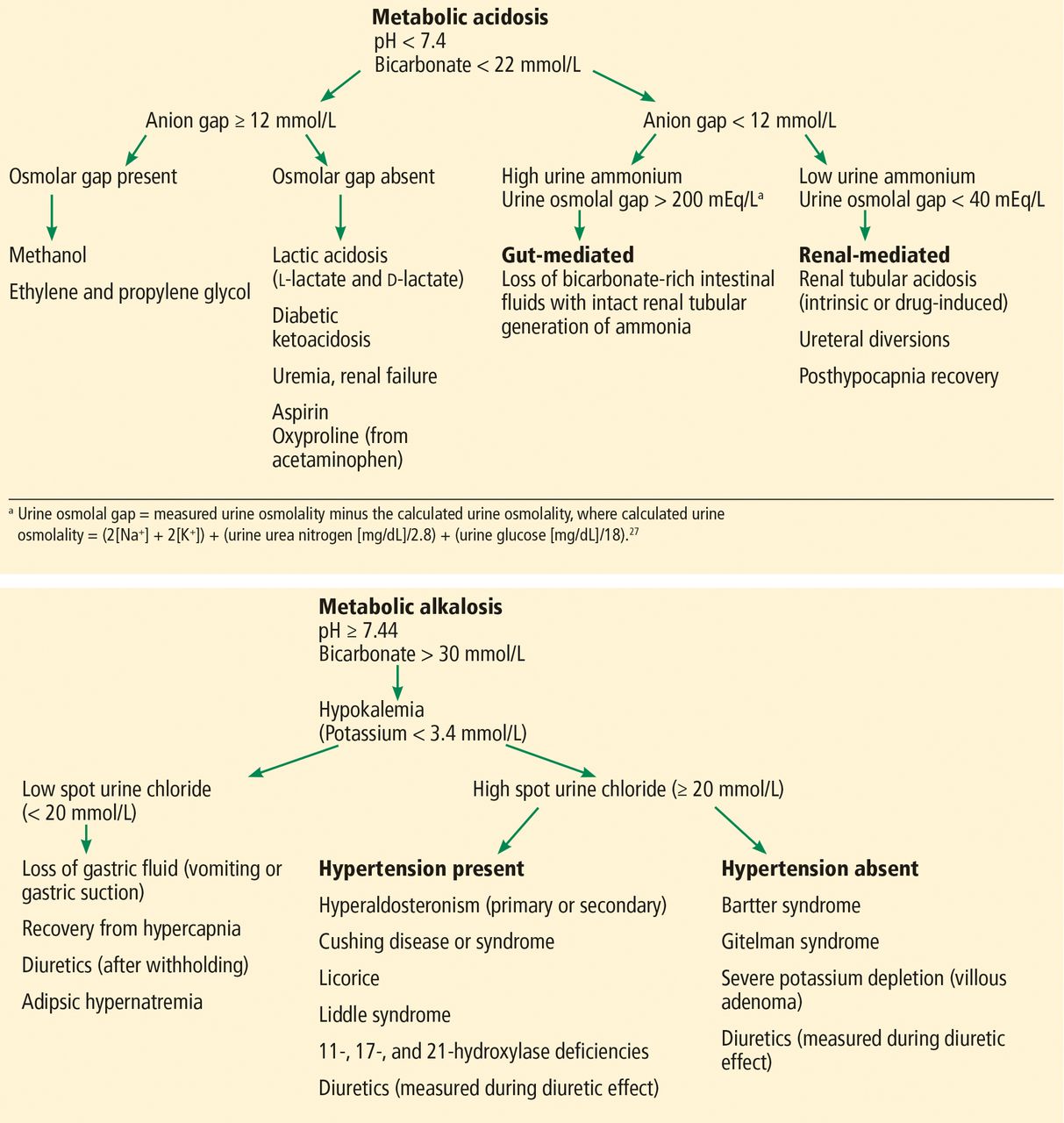
- Figure 1
Algorithms for determining causes of metabolic acid-base disturbances.
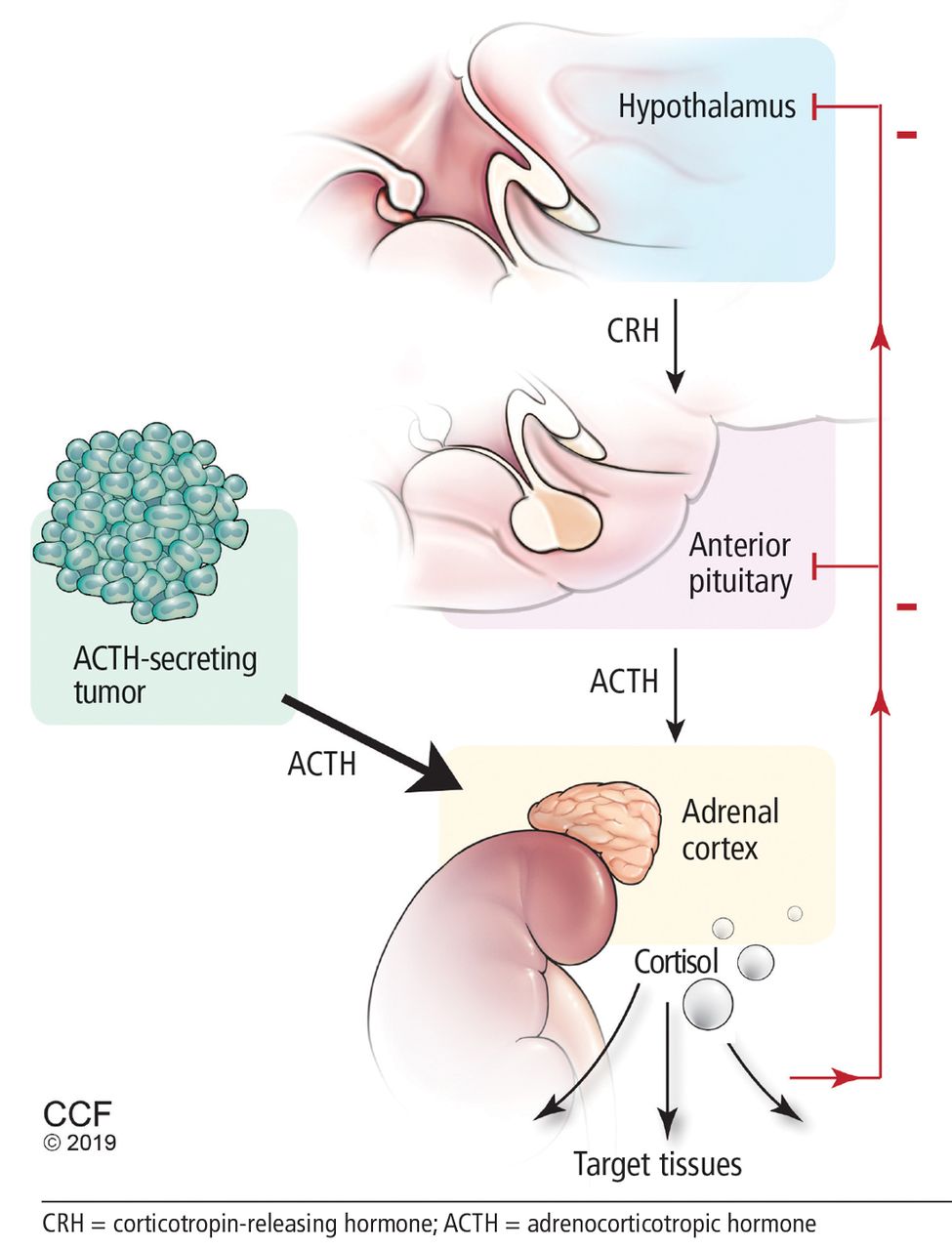
- Figure 2
The hypothalamic-pituitary-adrenal axis.
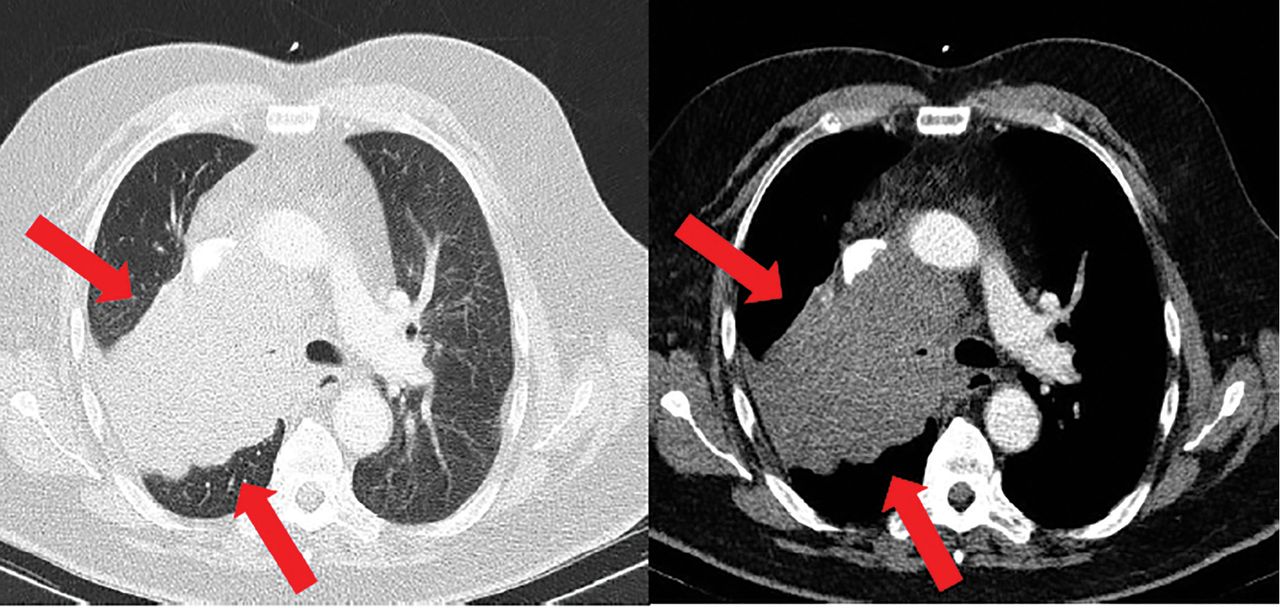
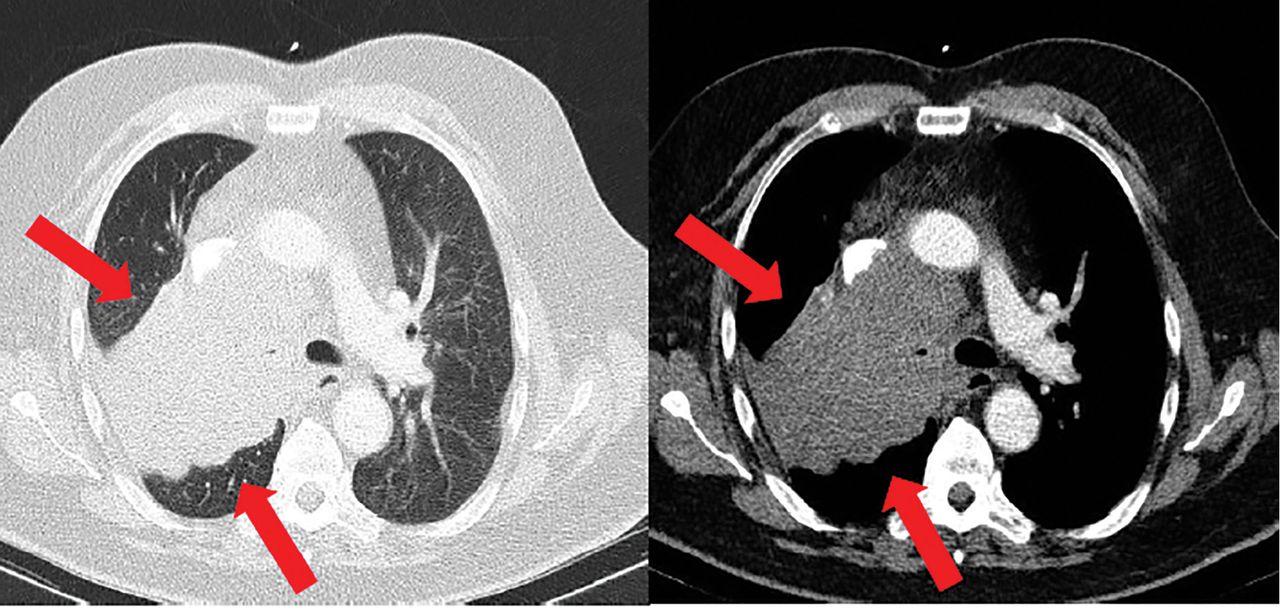
- Figure 3
Computed tomography of the chest depicting biopsy-proven small-cell carcinoma (arrows).

Tables
Test Current levela 1 year earlier Reference range Sodium (mmol/L) 144 135 136–144 Potassium (mmol/L) 2.8 4.0 3.7–5.1 Chloride (mmol/L) 96 100 97–105 Bicarbonate (mmol/L) 40 28 22–30b Serum creatinine (mg/dL) 1.2 1.2 0.58–0.96 Blood urea nitrogen (mg/dL) 28 19 7–21 Glucose (mg/dL) 197 74–99 Calcium and magnesium Normal Arterial blood gases pH 7.50 7.34 7.35–7.45 PCo2 (mm Hg) 51 40 34–46c PaO2 (mm Hg) 75 76 85–95 Bicarbonate (mmol/L) 40 22–26 1 Determine the arterial pH pH < 7.38 is acidemic, pH > 7.42 is alkalemica
Normal pH does not rule out an acid-base disorder2 If the arterial pH is abnormal, determine whether the primary process is respiratory, metabolic, or both pH PCO2 HCO3 Respiratory acidosisa Low High — Metabolic acidosis Low — Low Mixed respiratory and metabolic acidosis Low High Low Respiratory alkalosis High Low — Metabolic alkalosis High Variesb High Mixed respiratory and metabolic alkalosis High Low High 3 Calculate the anion gap Anion gap = sodium – (chloride + bicarbonate)
If serum albumin is low, add 2.5 mmol/L to the anion gap for every 1 g the serum albumin is below normal4 Check the degree of compensation (respiratory or metabolic) Pco2 and bicarbonate should increase or decrease together Normal levels: bicarbonate 25 mmol/L, PCO2 40 mm Hg Acute respiratory acidosis: For every 10-mm Hg increase in Pco2, bicarbonate should increase by 1 mmol/L Chronic respiratory acidosis (> 48 hours): For every 10-mm Hg increase in Pco2, bicarbonate should increase by 4 mmol/L Metabolic acidosis: For every 1-mmol/L decrease in bicarbonate, Pco2 should decrease by 1.3 mm Hg Acute respiratory alkalosis: For every 10-mm Hg decrease in Pco2, bicarbonate should decrease by 2 mmol/L Chronic respiratory alkalosis (> 48 hours): For every 10-mm Hg decrease in Pco2, bicarbonate should decrease by 5 mmol/L Metabolic alkalosis: For every 1-mmol/L increase in bicarbonate, Pco2 may increase by 0.6 mm Hg 5 If the patient has metabolic acidosis with an elevated anion gap, assess for ‘delta gap’ (whether the decrease in bicarbonate = the increase in anion gap) Delta gap = change in anion gap / change in bicarbonate ([anion gap – 10] / [24 – bicarbonate]) > 1: Additional metabolic alkalosis 1: No additional disturbance present < 1: Additional non-anion gap metabolic acidosis present ↵a Acidosis and alkalosis refer to acid-base disturbances with determined metabolic or respiratory etiologies. Alkalemia and acidemia refer to disturbances in blood pH prior to determination of the underlying metabolic/respiratory cause.
↵b Pco2 in metabolic alkalosis may vary depending on the clinical context, as compensation for metabolic alkalosis requires decreased respiratory drive, which may be influenced by other factors (ie, hypoxia).
Pco2 = partial pressure of carbon dioxide
Adapted from Mani S, Rutecki GW. A patient with altered mental status and an acid-base disturbance. Cleve Clin J Med 2017; 84(1):27–34. Copyright © 2017 The Cleveland ClinicFoundation. All rights reserved.
- TABLE 3
Renin and aldosterone values in hypokalemic metabolic alkalosis with high urine chloride
Renin and aldosterone Elevated blood pressure Normotensive High renin, high aldosterone, normal ratio of plasma aldosterone concentration(PAC) to plasma renin activity(PRA) Renal artery stenosis
Renin-secreting tumor
DiureticsBartter syndrome
Gitelman syndrome
Severe potassium depletion (villous adenoma)
DiureticsLow renin, high aldosterone, high PAC–PRA ratio Primary hyperaldosteronism Low renin, low aldosterone, normal PAC–PRA ratio Licorice
Cushing disease or syndrome
Hydroxylase deficiencies
Liddle syndrome Organ system Manifestation Cardiovascular Hypertension, thromboembolism, cardiomyopathy Metabolic Glucose intolerance/diabetes, hyperlipidemia, obesity Reproductive Menstrual irregularities, hirsutism, changes in libido, virilization Dermatologic Easy bruisability, striae, skin atrophy, hyperpigmentation, oily skin Musculoskeletal Proximal muscle wasting, osteopenia/ osteoporosis Neuropsychiatric Psychosis, emotional lability, depression, anxiety, sleep apnea Immunologic function Increased susceptibility to fungal and bacterial infection, opportunistic infections Ophthalmologic Glaucoma, cataracts, central serous chorioretinopathy, hypertensive retinopathy




{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- ASSESSING ACID-BASE DISORDERS
- WHICH TEST TO FIND THE CAUSE?
- IS HIS HYPERTENSION SECONDARY? IF SO, WHAT IS THE CAUSE?
- HYPERALDOSTERONISM
- TESTING FOR HYPERCORTISOLISM IN OUR PATIENT
- CUSHING SYNDROME
- ACTH-SECRETING TUMORS
- TREATMENT OF CUSHING SYNDROME DUE TO ECTOPIC ACTH SECRETION
- DISCUSSION
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.