


Article Figures & Data
Figures
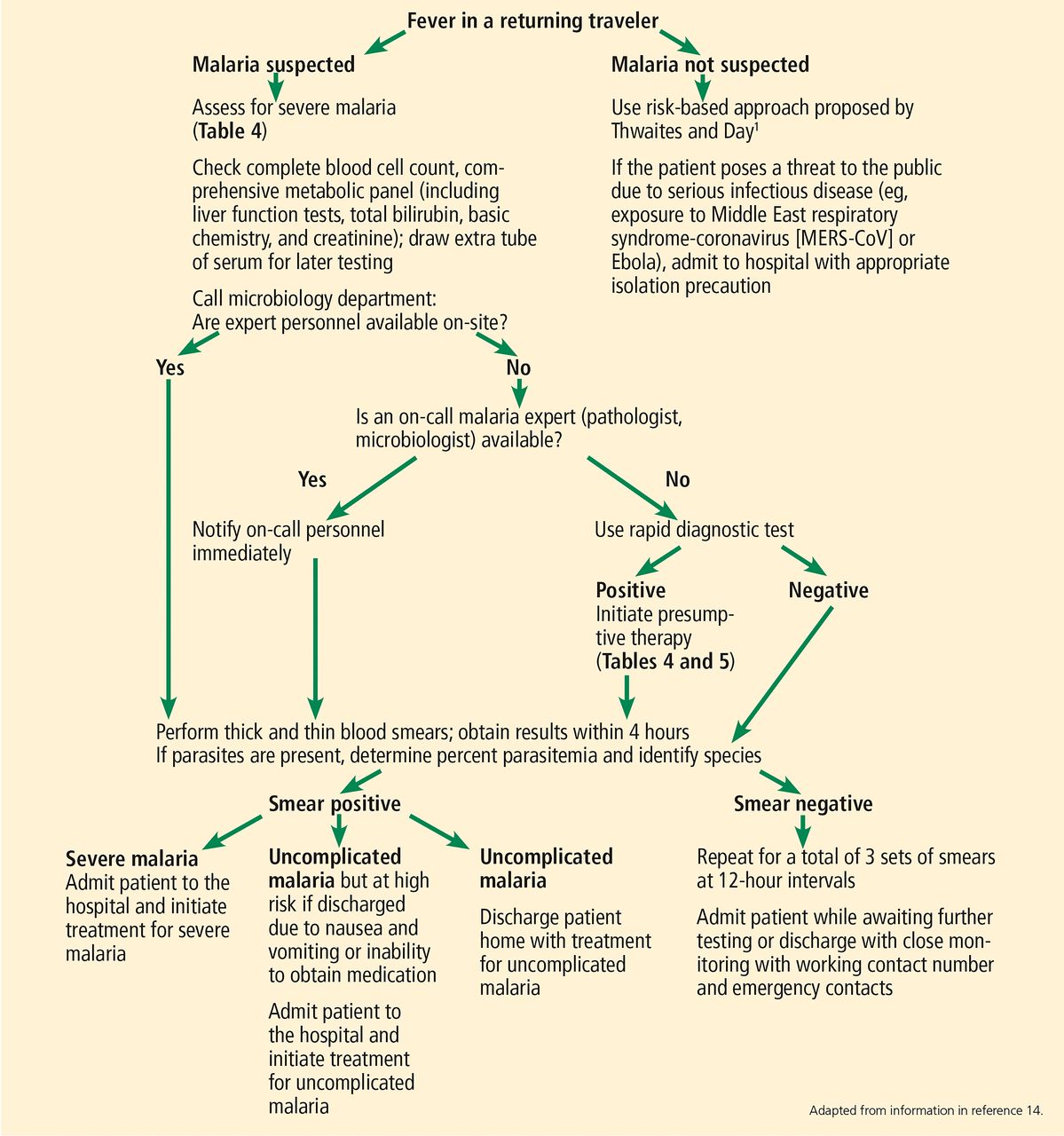
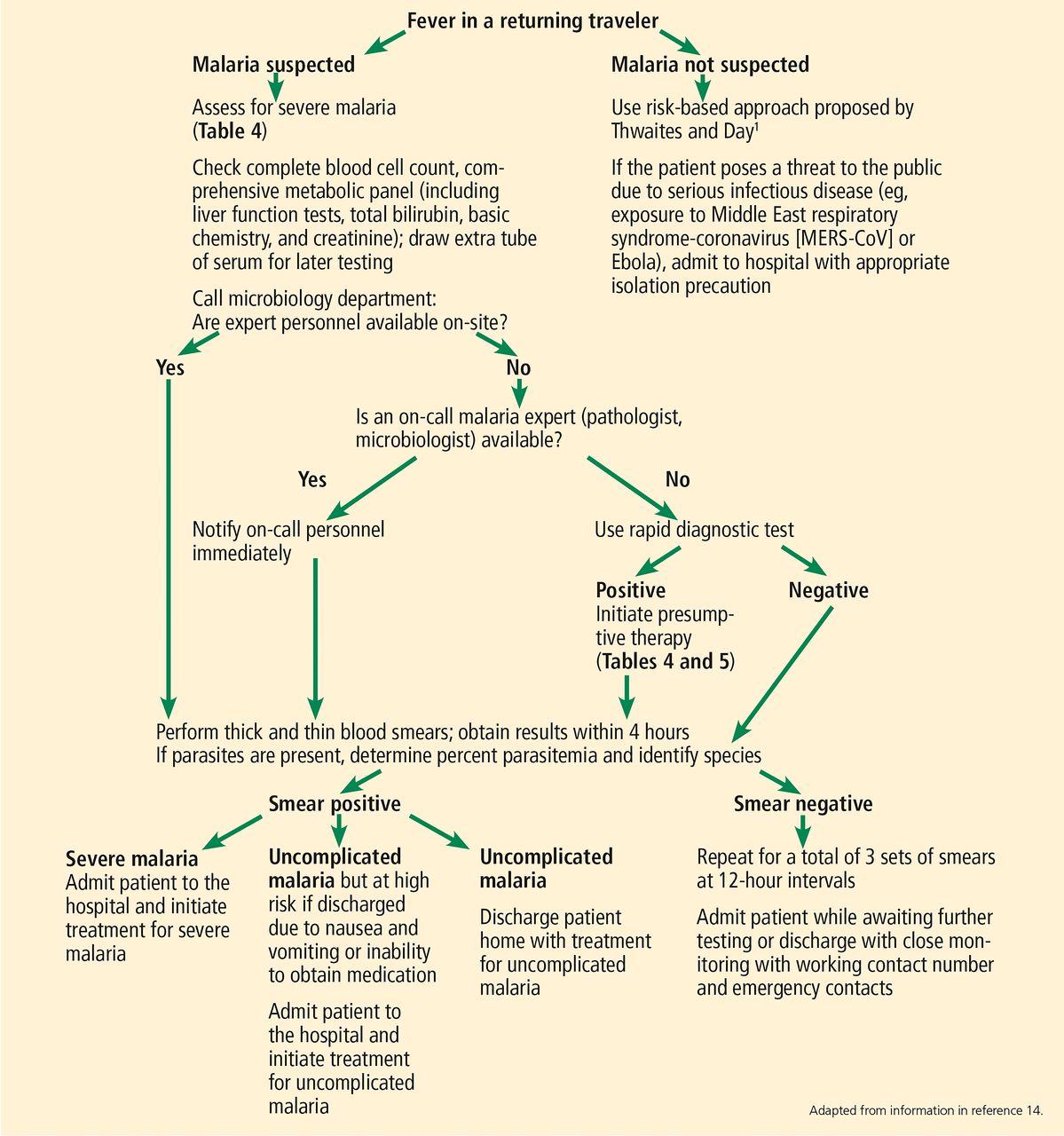
- Figure 1
Workup of fever in a returning traveler.
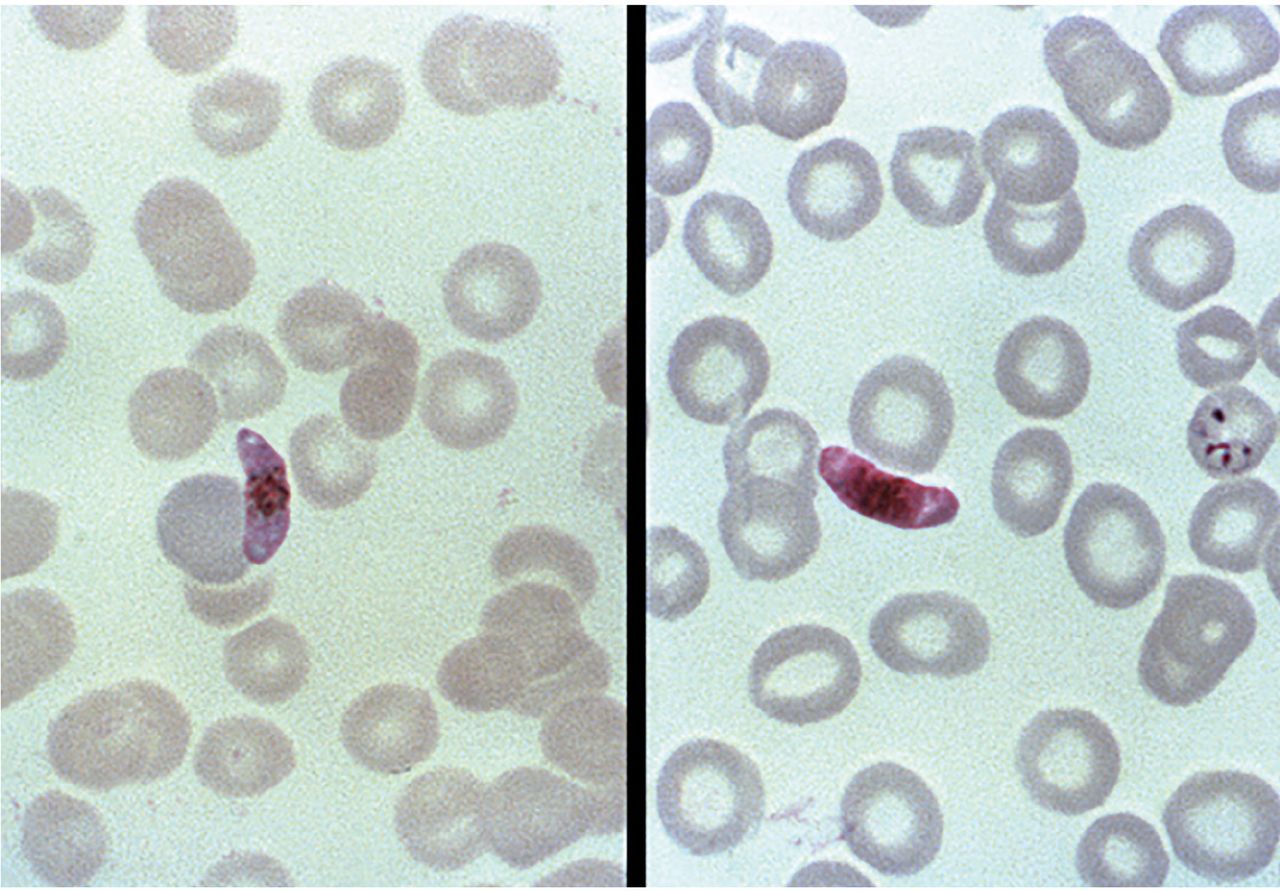
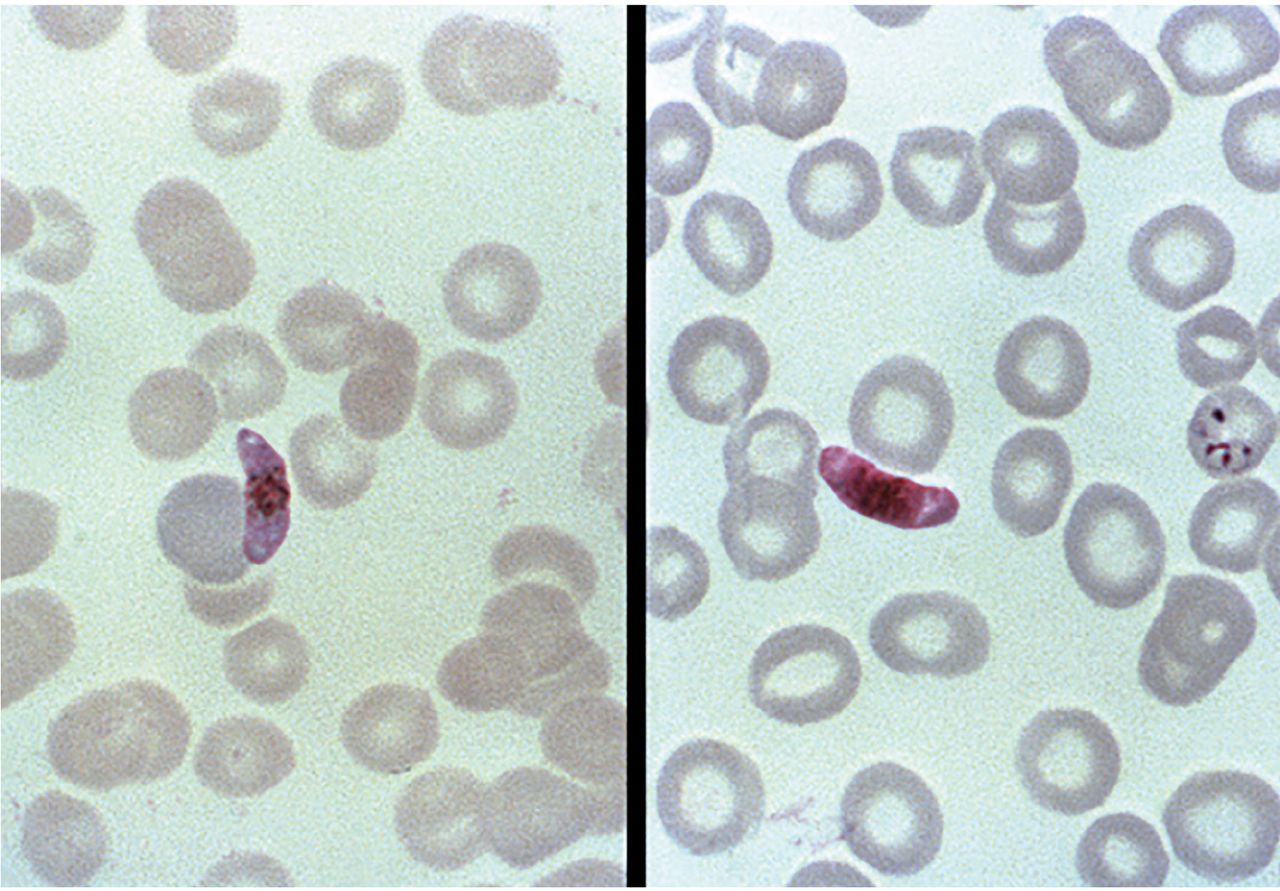
- Figure 2
Two Giemsa-stained, thin-film blood smear photomicrographs. Left, a Plasmodium falciparum macrogametocyte; right, a microgametocyte. Image by US Centers for Disease Control and Prevention, Steven Glenn, Laboratory & Consultation Division 1979.
Tables
Short (< 10 days) Medium (10–21 days) Long (> 21 days) Bacteria
Typhoid and paratyphoid
Bacterial diarrhea
Bacterial pneumonia
Neisseria meningitidis
Brucella species
Rickettsia species
Spirochetes
Relapsing fever (Borrelia recurrentis)
Leptospirosis
Viruses
Hemorrhagic feversb
Respiratory viruses
Influenza, Middle East respiratory syndrome coronavirus (MERS-CoV)
Measles
Protozoa
Malaria
African trypanosomiasis
Amoebic dysentery
Parasite
Fascioliasis
Bacteria
Typhoid and paratyphoid
Brucella species
Rickettsia species
Spirochete
Leptospirosis
Viruses
Hemorrhagic feversb
Human immunodeficiency virus (acute)
Cytomegalovirus
Hepatitis A
Rabies
Measles
Chicken pox (varicella)
Protozoa
Malaria
Giardia
Toxoplasma
African trypanosomiasis
Parasite
Babesia
Bacteria
Rickettsia species
Brucella species
Bartonellosis
Tuberculosis
Spirochetes
Leptospirosis
Syphilis
Viruses
HIV (acute)
Hepatitis B, hepatitis C
Epstein-Barr virus
Cytomegalovirus
Rabies
Measles
Protozoa
Malaria
Leishmaniasis
African trypanosomiasis
Parasites
Filariasis
Leishmaniasis
Amebic liver abscess
Babesia
↵a Bold-face type indicates a serious transmissible infection; isolation precaution is mandatory when such infections are suspected.
↵b Viruses that cause hemorrhagic fevers in humans comprise 5 distinct families:
Arenaviridae (lymphocytic choriomeningitis virus, Junin virus, Machupo virus, Lassa virus, Guanarito virus, Sabia virus, Chapare virus, Lujo virus)
Bunyaviridae (orthobunyavirus, phlebovirus [eg, Rift Valley fever virus], nairovirus [eg, Crimean-Congo hemorrhagic fever], hantavirus)
Flaviviridae (yellow fever, dengue fever, Japanese encephalitis, West Nile virus, Zika virus)
Filoviridae (cuevavirus, Marburgvirus, Ebolavirus)
Paramyxoviridae (measles, mumps, Newcastle disease virus, Hendra virus, Nipah virus).
Diseases that cause relative bradycardiaa Infections
Legionella
Psittacosis
Q fever
Typhus (Rickettsia typhi, Orientia tsutsugamushi)
Typhoid fever (Salmonella typhi)
Babesiosis
Malaria
Leptospirosis
Yellow fever
Dengue
Viral hemorrhagic fevers
Rocky Mountain spotted feverNoninfectious causes
Beta-blockers
Drug fever
Central nervous system lesions
Lymphomas
Factitious feverDiseases not associated with relative bradycardia Infections
Mycoplasma pneumoniae
Streptococcus pneumoniae
Salmonella (nontyphoidal)↵a A median increase in heart rate of less than 10 beats per minute for every increase of 1ºC in body temperature.
Anopheles
Malaria (Plasmodium species)
O’nyong’nyongAedes
Dengue fever
Yellow fever (Africa)
West Nile fever
Chikungunya
Eastern equine encephalitis
Zika virusCulex
West Nile virus
Japanese encephalitis
St. Louis encephalitisHaemogogus
Yellow fever (South America)Definition Treatment Positive blood smear and at least one of the following criteria: Impaired consciousness or coma
Severe normocytic anemia (hemoglobin < 7 g/dL)
Acute kidney injury
Acute respiratory distress syndrome
Hypotension
Disseminated intravascular coagulation
Spontaneous bleeding
Acidosis
Hemoglobinuria
Jaundice
Repeated generalized convulsions
Parasitemia ≥ 5%
Intravenous artesunate is available under an expanded-access investigational new drug protocol (call the US Centers for Disease Control and Prevention)
and
Artemether-lumefantrine, atovaquone-proguanil, doxycycline (clindamycin in pregnant women); if no other options, mefloquine↵a Severe malaria is most often caused by Plasmodium falciparum.
Plasmodium species Region Recommended medication P falciparum or species not identified Chloroquine-resistant (all areas except Central America or the Caribbean) or unknown Atovaquone-proguanil
Artemether-lumefantrine
Quinine sulfate + doxycyline, clindamycin, or tetracycline
MefloquineaChloroquine-sensitive (Central America or the Caribbean) Chloroquine phosphate
HydroxychloroquineP malariae or P knowlesi All Chloroquine phosphate
HydroxychloroquineP vivax or P ovale Chloroquine-sensitive Chloroquine phosphate + primaquine phosphate or tafenoquine
Hydroxychloroquine + primaquine phosphate or tafenoquineP vivax Chloroquine-resistant (Papua New Guinea or Indonesia) Quinine sulfate + doxycyline or tetracycline + primaquine phosphate or tafenoquine
Atovaquone-proguanil + primaquine phosphate or tafenoquine
Mefloquine + primaquine phosphate or tafenoquineAlternatives for pregnant women Chloroquine-sensitive Chloroquine phosphate
HydroxychloroquineChloroquine-resistant P falciparum and P vivax Artemether-lumefantrine (2nd or 3rd trimester only)
Quinine sulfate + clindamycin (all trimesters)
Mefloquine (all trimesters)a↵a Do not use in mefloquine-resistant areas (eg, Thailand, Myanmar, Cambodia, Vietnam).
Risk factors Not risk factors Rural setting Urban setting Camping Air-conditioned environment Longer duration of stay Shorter duration of stay Altitude of destination (< 2,000 m above sea level) High altitude (≥ 2,000 m above sea level) Inappropriate chemoprophylaxis Appropriate chemoprophylaxis with good adherence Visiting friends and relatives (eg, immigrants who return to home country to visit friends and relatives) Drug Adult dosage Adverse effects and cautions Pricea Chloroquine phosphateb 500 mg (300 mg base) once every week
Start 1–2 weeks before travel; stop 4 weeks after leaving malaria-endemic areaHypoglycemia, potential retinopathy from prolonged use
Only in chloroquine-sensitive areas (Central America and Caribbean)$23.11–$55.60 (7 tablets) Atovaquone-proguanil 250 mg/100 mg daily
Start 1–2 days before travel; stop 1 week after leaving malaria-
endemic areaDiarrhea, dreams, oral ulcers, headache
Take with food or whole milk
Contraindicated in severe renal impairment (creatinine clearance < 30 mL/min)$64.10–$86.02 (30 tablets) Doxycycline 100 mg daily
Start 1–2 days before travel; stop 4 weeks after leaving malaria-endemic areaDrug-induced esophagitis, photosensitivity
Do not use in children < 8 years old or in pregnant women$13.65–$52.23 (30 tablets)b,c Mefloquineb,d 250 mg once every week
Start 2 or more weeks before travel; stop 4 weeks after leaving malaria-endemic areaDo not use in individuals with cardiac conduction abnormalities, history of seizures, or serious psychiatric illnesses
Do not use in first trimester of pregnancy$30–$46.97 (8 tablets) Primaquine phosphate 30 mg daily
Start 1–2 days before travel; stop 1 week after leaving malaria-endemic areaContraindicated in glucose-6 phosphate dehydrogenase (G6PD) deficiency and women who breastfeed G6PD-deficient infants $37.68–$47.73 (28 tablets) Tafenoquine Loading: 200 mg daily starting 3 days before travel
Maintenance: 200 mg/week while in malaria-endemic area, starting 7 days after the last loading dose
Terminal prophylaxis: 200 mg once, 7 days after the last maintenance doseContraindicated in G6PD deficiency and women who breastfeed G6PD-deficient infants
Contraindicated in patients with history of psychotic disorders or current psychotic symptoms$37.52–$42.41 (2 Krintafel 150-mg tablets) ↵a Drug price obtained from www.goodrx.com on 10/25/19 at 11:33 AM.
↵b Can be used in pregnancy.
↵c Doxycyline monohydrate.
↵d Do not use if traveling to mefloquine-resistant areas (eg, Thailand, Myanmar, Cambodia, Vietnam).
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.