


Article Figures & Data
Figures
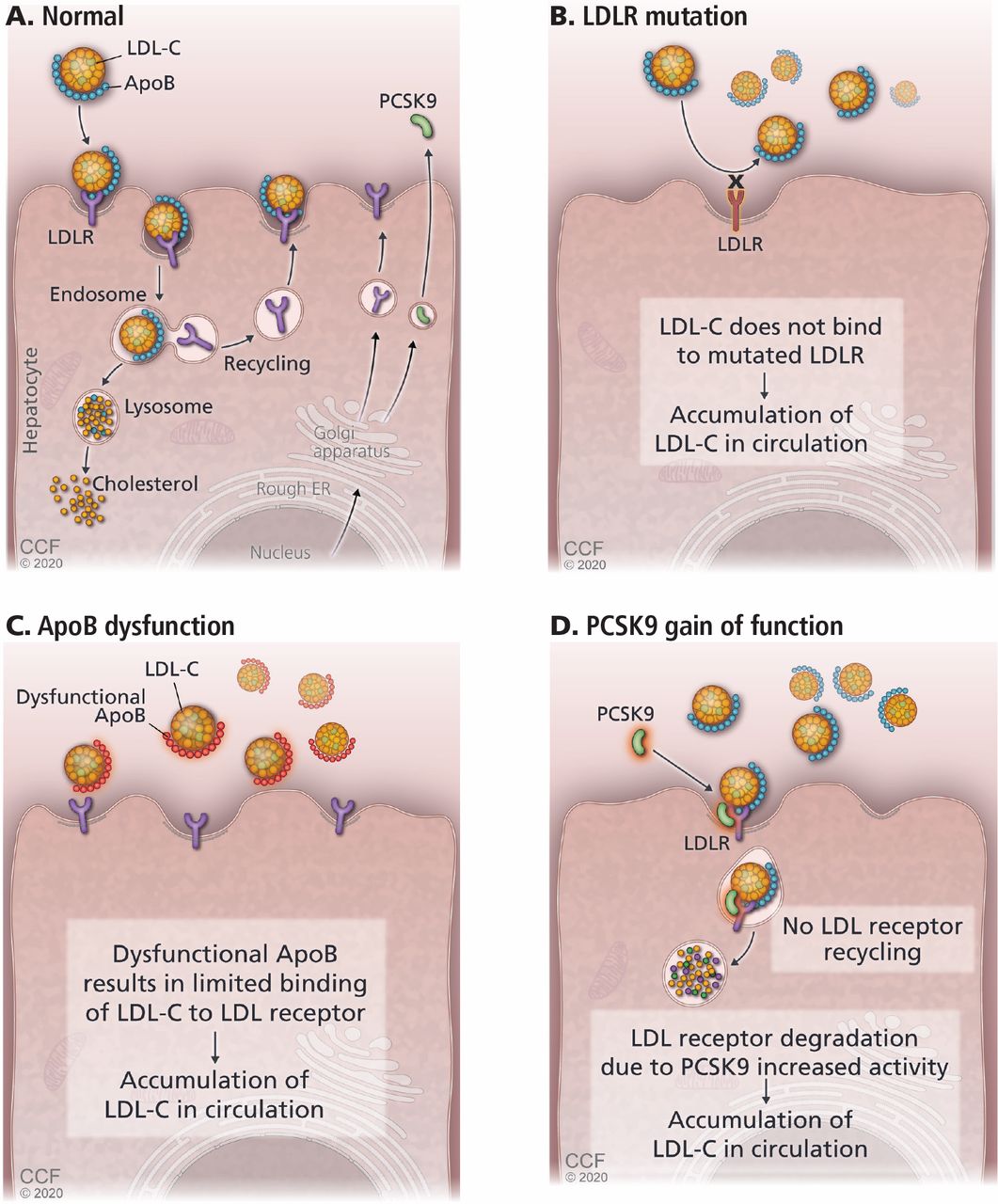
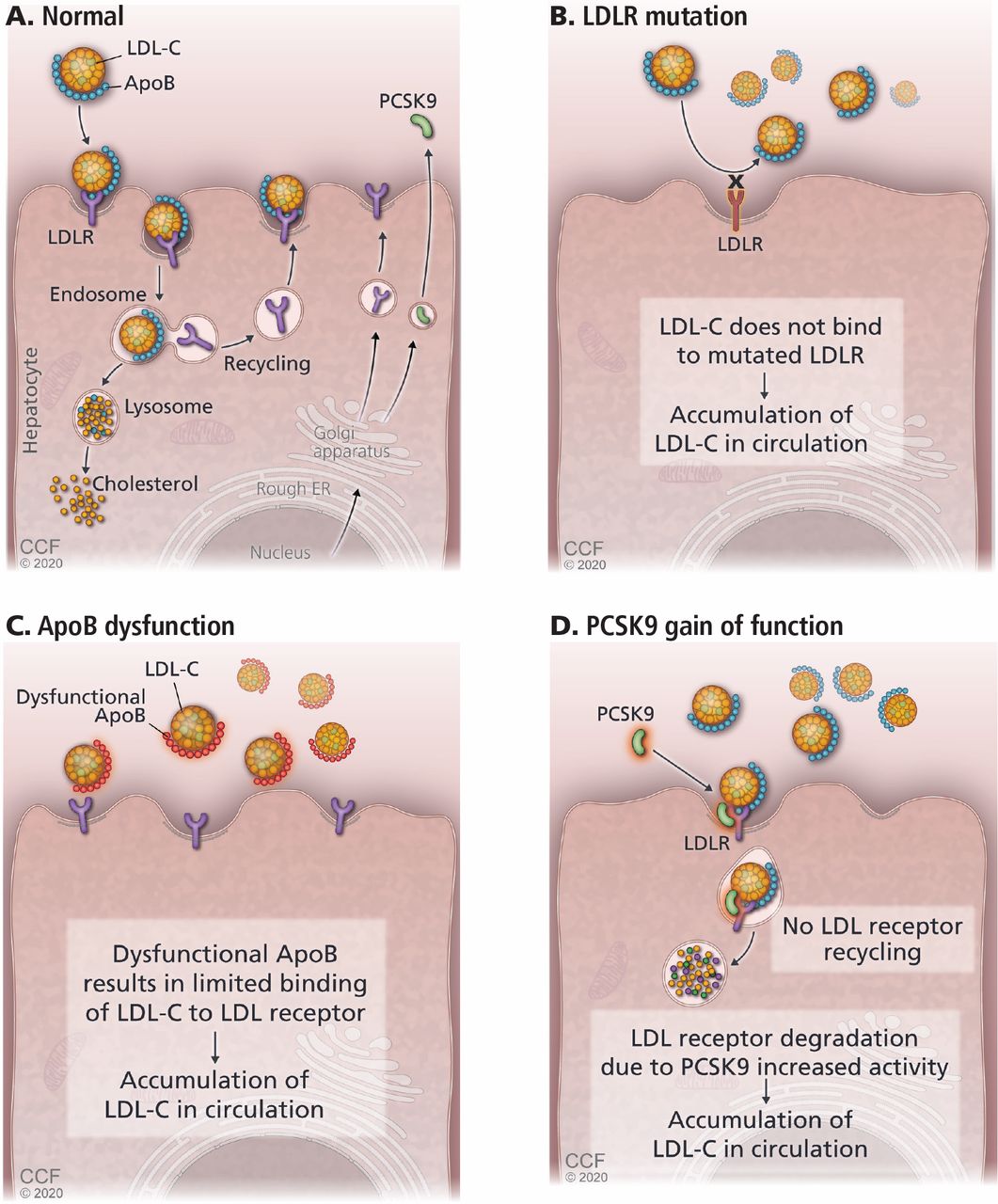
- Figure 1
(A) Low-density lipoprotein cholesterol (LDL-C) binds to its receptor (LDLR), using apolipoprotein B (ApoB) as its ligand. Defects in LDLR (B) or ApoB (C) result in less binding of LDL-C, raising LDL-C levels. (D) Proprotein convertase subtilisin kexin type 9 (PCSK9) binds to LDLR and escorts it into the interior of the hepatocyte, where it is destroyed, resulting in fewer receptors and higher LDL-C concentrations. Gain-of-function mutations in PCSK9 raise LDL-C levels.
- Figure 2
Xanthomas of the Achilles tendons. Note the position used for examination, with the patient kneeling on a chair.
From Sibley and Stone, reference 27.
- Figure 3
Corneal arcus.
From Sibley and Stone, reference 27.
- Figure 4
Algorithm for cascade screening.
Reprinted from Sturm AC, Knowles JW, Gidding SS, et al; Convened by the Familial Hypercholesterolemia Foundation. Clinical genetic testing for familial hypercholesterolemia: JACC Scientific Expert Panel. J Am Coll Cardiol 2018; 72(6):662–680. Copyright 2018, with permission from Elsevier.



Tables
- TABLE 1
The Dutch Lipid Clinic Network diagnostic criteria for familial hypercholesterolemia
Criteria Points Family history First-degree relative with known premature atherosclerotic cardiovascular disease (age < 55 in men, age < 60 in women) or first-degree relative with LDL-C > 95th percentile 1 First-degree relative with tendon xanthomas or arcus cornealis, or child under age 18 with LDL-C > 95th percentile 2 Clinical history Premature coronary artery disease 2 Premature cerebral or peripheral vascular disease 1 Physical examination Tendon xanthomas 6 Arcus cornealis before age 45 4 LDL-C levels, mg/dL ≥ 330 8 250–329 5 190–249 3 155–189 1 DNA analysis Functional mutation in the LDLR, APOB, or PCSK9 gene 8 Interpretation Total Definite familial hypercholesterolemia > 8 Probable familial hypercholesterolemia 6–8 Possible familial hypercholesterolemia 3–5 Unlikely familial hypercholesterolemia < 3 From the World Health Organization, reference 24.
Criteriona Description A Total cholesterol level > 290 mg/dL or LDL-C > 190 mg/dL in adults (age ≥ 16) Total cholesterol level > 260 mg/dL or LDL-C > 155 mg/dL in children (age < 16) B Tendon xanthomas in the patient or in a first- or second-degree relative C DNA-based evidence of a mutation in LDLR, APOB, or PCSK9 D Family history of myocardial infarction before age 50 in a second-degree relative, or before age 60 in a first- degree relative E Total cholesterol > 290 mg/dL in a first- or second-degree relative ↵a “Definite” familial hypercholesterolemia requires criterion C by itself, or criterion A plus B; “probable” familial hypercholesterolemia requires either A plus D, or A plus E.
Information from the Simon Broome Register Group, reference 25.
- TABLE 3
MED-PED diagnostic criteria for probable heterozygous familial hypercholesterolemia
Age Closest relative with familial hypercholesterolemia First-degree Second-degree Third-degree None Threshold cholesterol level (mg/dL) in the patient Total LDL-C Total LDL-C Total LDL-C Total LDL-C < 20 220 155 230 165 240 170 270 200 20–29 240 170 250 180 260 185 290 220 30–39 270 190 280 200 290 210 340 240 ≥ 40 290 205 300 215 310 225 360 260 Reprinted from Williams RR, Hunt SC, Schumacher MC, et al. Diagnosing heterozygous familial hypercholesterolemia using new practical criteria validated by molecular genetics. Am J Cardiol 72(2):171–176, copyright 1993, with permission from Elsevier.
- TABLE 4
The Montreal FH score to predict cardiovascular risk in familial hypercholesterolemia
Cutoff Points Age ≤ 21 0 22–28 4 29–35 8 36–42 12 43–49 16 50–56 20 57–63 24 > 63 28 High-density lipoprotein cholesterol, mg/dL ≤ 23 12 23–34 9 35–46 6 47–58 3 > 58 0 Hypertension Yes 2 No 0 Smoking Yes 1 Never 0 Sex Male 3 Female 0 A score > 20 is associated with a 10-fold higher cardiovascular risk. Reprinted from Paquette M, Brisson D, Dufour R, Khoury É, Gaudet D, Baass A. Cardiovascular disease in familial hypercholesterolemia: validation and refinement of the Montreal-FH-SCORE. J Clin Lipidol 11(5):1161–1167.e3. Copyright 2017, with permission from Elsevier.




{kind=link}
{kind=link}
{kind=link}
{kind=link}